
Abstract
The brain needs body image to plan movements. Our recent studies use an ischemic block of a limb to study the mechanisms of changes in body image. First, if the fingers, wrist, elbow, ankle, and knee are extended before and during the block, then the perceived limb is flexed at the joint and vice versa. The final position of the phantom limb depends on its initial position. Second, the perceived size of the hand increases gradually as anesthesia develops. The start of these perceptual changes occurs when input from large-diameter sensory nerve fibers is declining. Third, at the end of the block, when participants are allowed to see their foot, its perceived position reverts to that indicated by them earlier.
Over the past century, the pioneering concept of body schema (Head & Holmes, 1911) has led to a proposal of two distinct body representations: body image and body schema (de Vignemont, 2010; Proske & Gandevia, 2012). The body schema derives from somatosensory, visual, and vestibular inputs and is generated in the parietal cortex. A function of the parietal cortex is proposed to update and integrate actual and predicted (efference copy) sensory feedback about the lengths of body segments and the position and movement of joints (Shadmehr & Krakauer, 2008). The efference copy reaches the premotor cortex to drive movement corrections when errors arise (Wolpert, Ghahramani, & Jordan, 1995). Thus, changes in body schema could occur within the parietal cortex as well as within the premotor cortex.
Carruthers (2008) further proposed “on-line” and “off-line” representations of the body. The on-line representation is provided by inputs such as vision, touch, and proprioception, and it updates perception of the body from moment to moment. The off-line representation is constructed in part from current sensory inputs and in part from stored memories. The concept of off-line representation is useful to account for phenomena such as the development of phantom limbs after amputation.
The attempt to produce an acute block of peripheral nerves to a limb to create an experimental phantom provides insight into how an on-line representation of the body might be constructed. Phantom limbs generally adopt a habitual posture or a posture that resembles that prior to amputation (Ramachandran & Hirstein, 1998; Paqueron, Leguen, Gentili, Riou, Coriat, & Willer, 2004). Melzack and Bomage (1973) asked prone participants to describe the position of a phantom arm after an anesthetic nerve block at the brachial plexus. The phantom arm lies at the side of the body, above the lower abdomen, or above the lower chest. Orderly perceived changes in posture occur spontaneously between these three positions during the block. However, the extent to which the phantom limbs depend on afferent input and the mechanisms underlying any perceptual changes and distortion of the phantom limbs is poorly understood. Slightly, Gentili, Verton, Kinirons, and Bonnet (2002) suggest that the posture of an experimental phantom is close to the posture of the limb when the nerve block is induced. It is anticipated that the initial posture of an experimental phantom influences the final posture of the phantom. The initial position of a limb before anesthesia was critical for the subsequent illusory changes in posture in a series of studies from our laboratory (Inui, Walsh, Taylor, & Gandevia, 2011; Inui, Masumoto, Beppu, Shiokawa, & Akitsu, 2012; Inui, Masumoto, Ueda, & Ide, 2012; Inui & Masumoto, 2013). In addition, we have identified a key parameter for the illusory changes in limb position.
This article provides and overview and discussion of our recent studies on body image reported elsewhere. The article is divided into six sections. The first section reviews systematic changes in the perceived posture of an experimental phantom hand following cuff inflation of the upper arm (Inui, et al., 2011). Changes in sensation following an ischemic nerve block are reported in the second section (Inui, et al., 2011). The third section points out that the extreme posture of a limb is essential for systematic changes in the perceived posture during the block (Inui, Matsumoto, Beppu, et al., 2012). The fourth section describes systematic changes in the perceived posture by interactions between biarticular muscles across two joints during the block (Inui, Matsumoto, Ueda, et al., 2012). The fifth section quantitatively describes effects of visual information on the perceived posture of the foot and leg at the end of the block (Inui & Masumoto, 2013). The sixth section describes changes in the perceived size of the hand following an ischemic nerve block (Inui, et al., 2011).
Development of a Phantom Wrist and Fingers
We conducted an ischemic block of peripheral nerves to the upper arm to create an experimental phantom hand. We then examined how an on-line representation of the body might be constructed, and determined whether the initial posture of the wrist and fingers before anesthesia systematically changed the final posture of the phantom hand.
Ten participants were seated and the right hand held in mid-pronation in a manipulandum that rotated in the flexion–extension plane of the wrist. The apparatus, hand, and arm to above the elbow were screened from the participant's view. A wide cuff with two chambers (Zimmer, Dover, OH, USA) was positioned on the upper arm and connected to a regulated pressure source so that the cuffs could be simultaneously inflated to 300 mmHg in less than 1 sec. To measure the development of the phantom hand, the participants indicated the perceived angular positions of their phantom fingers and wrist using a wooden hand, the posture of which allowed positioning in flexion and extension at the metacarpophalangeal and interphalangeal joints of the fingers. To assess perceived position at the wrist, a rotating pointer on the model was used. The model was positioned on the table about 20 cm in front of the participants and 30 cm to the left of the midline. The participants were asked to “signal the perceived finger positions of your right hand by using the wooden hand” and to “think about each finger individually.” The wooden hand and wrist pointer were photographed with a digital camera mounted above the model to provide an indication of the perceived angular positions of the fingers and wrist. After each estimate of wrist and finger posture, the joints of the model hand were alternately placed in full extension or full flexion.
A control study reveals that there was no significant adaptation of the participants' perceived position of their intact wrist and fingers over a period of 40 min. when the hand is maintained in the test posture with the wrist and fingers held comfortably extended. However, after cuff inflation, despite the position of the hand and wrist being fixed in either flexion or extension, the perceived position of the wrist and fingers changed systematically. This change was evident after 10–15 min., and surprisingly, the direction of the change depended on the posture in which the hand was held. If the wrist and fingers were extended fully before and during an ischemic block, then the hand was finally perceived as flexed at the wrist and fingers. Conversely, if the hand was flexed fully, then the perceived position of the wrist and fingers moved towards extension. The final position of the perceived hand depended on its initial position. The change in position did not involve anatomically impossible hand postures and changes were in the same direction. In all participants, the hand is perceived to move continuously with no default position. Figure 1 illustrates changes in the perceived posture of the hand during the block. Figure 2 shows mean data (±95% confidence interval) for the changes in perceived joint angle at the wrist and three index finger joints. When the ischemic block was applied with the wrist and finger joints extended (data in red), these joints were perceived to flex gradually as the block develops. In contrast, the wrist and finger joints were perceived as extended progressively when the block was applied with them in a flexed position (data in blue). For the mean data, the progression of these changes in joint angle was approximately linear until a final stable posture was reached. The magnitude of the perceived changes in joint angle was less when the hand was flexed than when it was extended. However, after about 40 min. of ischemia, the final perceived position of the wrist and finger joints had ‘crossed over.’
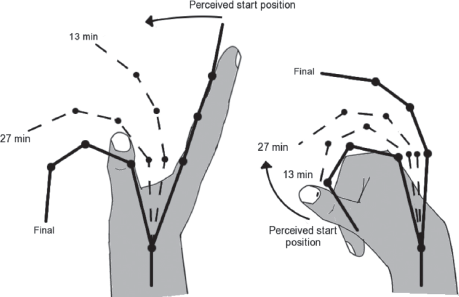
Actual and perceived posture of the hand during an ischemic block. Data are obtained from 10 participants for the two versions of the main experiment (wrist and hand extended on left, wrist and hand flexed on right). Shaded hands show the true maintained posture of the hand. Thick black lines show the perceived starting position of the hand prior to cuff inflation and the perceived final position of the phantom hand at the end of the block. The dashed lines are the mean perceived position of the developing phantom at intermediate times of 13 min. and 27 min. Data at these times were determined from the regression fitted for each participant. Time zero is the time of cuff inflation. The direction of the perceived change is given by the curved arrow. (Inui, et al., 2011, Redrawn with permission from the Journal of Physiology).

Perceived angle of the wrist and index finger joints during an ischemic block. The solid lines represent regression lines of the average of all 10 participants with 95% confidence intervals (dashed lines) for the wrist, metacarpophalangeal joint (MC), proximal interphalangeal joint (PIP) and distal interphalangeal joint (DIP). 180° represents a straight joint (Modified from Inui, et al., 2011).
To determine whether the changes in posture of the hand depend on one posture for 10 min. before inflation, we repeated the block for two participants. Again, the hand was fixed in the fully flexed position for 10 min. but just before the cuff was inflated the hand was moved into the fully extended position and held there. The wrist and fingers are perceived to flex in a qualitatively similar way to when the hand has been held for 10 min. in the extended posture before inflation. Hence, holding the wrist and hand positions constant for 10 min. before inflation was not critical for generation of the subsequent illusory changes in position.
In a series of studies (Inui, et al., 2011; Inui, Matsumoto, Beppu, et al., 2012; Inui, Matsumoto, Ueda, et al., 2012), the extended wrist and elbow become perceived as the flexed phantom joints during ischemic anesthesia. In an extreme posture, the perceived posture of the body part may be determined by the muscle group stretched by that posture, which would generate a higher proprioceptive discharge. Nerve block lowers the discharge and leads to a perceived change in posture. In contrast, the low discharge from the muscle group shortened by that posture plays no role in the observed changes. Transcranial magnetic stimulation studies show that muscles proximal to an ischemic block have increased motor evoked potential amplitudes (Brasil-Neto, Valls-Sole, Pascual-Leone, Cammarota, Amassian, Cracco, et al., 1993; Ridding & Rothwell, 1995) and larger motor representation maps (Ridding & Rothwell, 1995). Loss of sensory input caused by an ischemic block could lead to the release of afferent inhibition, which might produce the increase in cortical excitability observed after an ischemic block (Vallence, Reilly, & Hammond, 2012). The release of afferent inhibition is supported by a decrease in GABA levels in the primary motor cortex measured using magnetic resonance spectroscopy during an ischemic block (Levy, Ziemann, Chen, & Cohen, 2002). These previous studies thus suggest that the change in body image from the extreme posture during the ischemic block in the present study was induced by changes in cortical excitability.
Changes in Sensation Following Cuff Inflation
In this section we compare the timing of impairment of different sensory modalities with development of changes in the body image. During the development of the ischemic block there was a progressive degradation in touch sensation. The changes in body image thus appeared to occur as input from large-diameter sensory nerve fibers was declining. Measurements of touch (detection of light touch and von Frey hair thresholds) in the hand, just proximal to the wrist and just distal to the elbow, changed systematically. Cutaneous touch sensation was impaired progressively, beginning distally (Fig. 3). The initial impairment (an increase in von Frey threshold) began at 16.5 [15.0–18.5] (median [interquartile range]) min. for the hand and at 20.5 [16.5–25.5] min. for the elbow. Complete loss of detection of light touch followed the same pattern, again occurring earlier at the hand (19.5 [18.3–20.6] min.) than at the elbow (37.5 [29–39] min.). At 20–25 min., thresholds for cold sensation began to change throughout the arm while a computer-driven thermode was used to assess thermal pain thresholds. Cold is initially reported at a mean of 28.3°–28.8° at the three sites. These temperatures dropped by 5–9° at the end of cuff inflation, with the change being slightly greater distally than proximally. Then, cold stimuli were commonly reported as painful. Changes in von Frey thresholds preceded changes in cold sensation for all 10 participants at the hand, 9 participants at the wrist and for 6 participants at the elbow. Even after 30– 40 min. of ischemia, high skin temperatures still elicited a distinct sensation of heat pain. This index of C-fiber function changed only slightly at each site. The thresholds rise from 43° to 44° by the end of cuff inflation.

Timing of changes in sensation following an ischemic block of the upper arm. Data are shown for assessments made over the base of the thumb (upper panel), just proximal to the wrist (middle panel) and just proximal to the elbow (lower panel). Mean and interquartile range plotted for the start of a change in von Frey threshold, the loss of light touch and the onset of elevation in cold thresholds (Inui, et al., 2011, Redrawn with permission from the Journal of Physiology).
The perceived postures of the finger and wrist are changed from 10–15 min. after inflation. For this short period (about 10 min.), the right hand and forearm constituted an incomplete phantom limb because of incomplete loss of detection of touch in the hand, wrist, and elbow. Brasil-Neto, et al. (1993) reported that corticospinal excitability increased in muscles proximal to an ischemic nerve block within 7 to 8 min. following the block. The starting time of the increase in corticospinal excitability approximately corresponded to that of a change in the finger and wrist postures in this study. The existing cortical circuits might be disinhibited from this time after the block. The finding that the incomplete phantom hand was perceived as having moved suggests a change in body image on the basis of the rapid changes of the cortical circuits.
In the conventional view (Gasser & Erlanger, 1929; Mackenzie, Burke, Skuse, & Lethlean, 1975), pressure on a nerve can cause loss of conduction in large-diameter motor, touch, and pressure fibers while pain sensation remains relatively intact. Conversely, local anesthetics depress transmission in the group C fibers before they affect group A touch fibers. Inui, et al. (2011) assessed thermal and pain thresholds, showing resistance to prolonged ischemia of small fibers (presumably group C fibers), which signal heat pain. Smaller fibers (presumably group Aδ fibers) also included the main population of cold (Johnson, Darian-Smith, & LaMotte, 1973; Mackenzie, et al., 1975), and by the end of the ischemic period (40 min.), we found a marked impairment of cold thresholds (by 5–10°). These observations make it likely that a change in body image can be initiated and driven by incomplete loss of background input from large-diameter sensory axons.
Extreme Postures are Essential for Changes in Body Image During Anesthesia
In this section we review what happens if the hand is held in the mid-position before and during ischemic block, because a fully flexed or extended hand becomes perceived as an extended or flexed phantom hand sensation as the block progressed in our previous study (Inui, et al., 2011). By holding the wrist in the fully extended, fully flexed, and mid-positions before and during the ischemic block, this study demonstrated that a fully flexed or extended position of the wrist was essential for systematic perceived changes in the wrist joint during the block.
A wide cuff was positioned on the right upper arm and connected to the automatic tourniquet system (Zimmer ATS 750) so that the cuff could be simultaneously inflated to 250 mmHg in less than 1 sec. To measure perceived arm and hand postures during the development of the ischemic block, participants were instructed to demonstrate the perceived positions of the right elbow and wrist using the left arm and hand attached to a flexible two-axis goniometer system (DKH, Tokyo, Japan). While the locations of the left and right hands and arms were symmetric with respect to the median line before each testing trial, the left arm and wrist were extended on a bed. Sensory tests included assessments of tactile sensation with von Frey hairs and the ability to detect a light touch with a cotton swab. Pain perception was also assessed by firmly pinching the skin of the thumb and elbow.
The major finding was that, despite the position of the arm and hand being fixed in either flexion or extension, after cuff inflation the perceived position of the elbow and wrist changed systematically in all participants. If the actual arm and hand were fully extended, then the perceived position of the elbow and wrist moved towards flexion. Conversely, if they were fully flexed, then the perceived position of the joints moved toward extension. The new finding was that, when the hand was held in the mid-position before and during the ischemic block, the posture of the wrist was perceived to be in the same position.
The important difference between an extreme and mid-position was that in mid-position the firing of afferents signaling flexion and extension was balanced so that as afferent firing disappeared, it did so in a balanced way. In contrast, at an extreme position, one signal will be high and the other very low so that disappearance of afferents will mainly alter the high signal. The perceived hand posture was determined largely by activity coming from afferents in muscle and skin stretched by extreme posture. As ischemic anesthesia progresses, the stretch receptor activity falls and this fall is perceived as a change in hand posture. However, the firing rate of the muscle spindles in the both extensor and flexor when the hand was held in the mid-position may have been less than that in the extreme position before and during the anesthesia. Hence, these results suggested that the loss of signals from muscle spindles in the fully flexed or extended position of a limb was essential for systematic changes in the perceived posture of a limb during anesthesia.
Changes in Perceived Postures by Interactions Between Biarticular Muscles
In previous studies (Inui, et al., 2011; Inui, Matsumoto, Beppu, et al., 2012), the elbow, wrist, and fingers were fixed in the same direction during an ischemic block. To further examine posture illusions during the block, we have to consider that many muscles are biarticular. For example, the flexors of both upper arm and forearm overlap across the elbow joint. When an ischemic block is performed with the wrist in full flexion, but with the elbow in full extension, we anticipate that there are changes in the perceived posture due to the afferent signal coming from the main muscles acting at the two joints. Hence, this section examines what happens if the wrist is fixed in full extension while the elbow in full flexion before and during the anesthesia, and vice versa. The study reviewed in this section was conducted using the same experimental procedure and measurements as described in previous sections. While a wide cuff was positioned on the right upper arm and connected to the automatic tourniquet system, the perceived positions of the right elbow and wrist were measured using the left arm and hand attached to a goniometer system.
The new finding of this study was that, in all participants after cuff inflation, if the actual wrist was fully extended while the actual elbow was fully flexed, then the perceived position of the wrist moved towards flexion and that of the elbow moved toward extension. Conversely, if the actual wrist was fully flexed while the actual elbow was fully extended, then the wrist was perceived to extend and the elbow was perceived to flex. These systematic changes in position did not involve arm and hand postures that were anatomically impossible, and the changes were in the same direction. The arm and hand were perceived to move continuously with no default position. In addition, the final position of the phantom limb depended on its initial position.
The two perceived postures at the two joints obviously moved in opposite directions. These results thus indicated that there were changes in the perceived posture due to the loss of the afferent signal coming from the main muscles acting at the two joints. Similar to the perceptions when the wrist and elbow were fixed in the same direction in our previous studies (Inui, et al., 2011, 2012), changes in the perceived posture at each joint depended on its initial position even when the two joints were fixed in the opposite direction.
Effect of Visual Information on Perceived Posture
Visual information plays an important role in the formation of body image. On the role of the visual image of the body, Ramachandran and Rogers-Ramachandran (1996) and Hunter, Katz, and Davis (2003) have observed that mirrors can induce synesthesia in a phantom limb. Botvinick and Cohen (1998) have also found that illusions of ownership of a rubber hand can be elicited by synchronized visual and tactile stimuli in normal participants. Paqueron, Leguen, Rosenthal, Coriat, Willer, and Danziger, (2003) further reported the effect of sight following the description of the changes in body image induced by local anesthesia. When most participants saw their anesthetized limb, the illusion of the position and posture of the anaesthetized limbs was influenced by visual information, whereas the sensation of body shape alteration itself was not modified by the information. Silva, Bataille, Jucla, Minville, Samii, Fourcade, et al. (2010) also reported that visual information caused a rapid superposition of the position of the phantom limb on the real posture of the anesthetized limb in all participants. Most participants again reported the position illusion following the reintroduction of the visual mask. However, Paqueron, et al. (2003) and Silva, et al. (2010) did not describe the effects of visual information on the body image quantitatively. This section thus examined quantitative effects of visual information on changes in perceived posture following an ischemic block.
A wide cuff was positioned on the right thigh and connected to the automatic tourniquet system. Sensory tests were conducted at three sites: the dorsum of the big toe, just proximal to the dorsum of the ankle, and the volar surface of the leg just distal to the knee. To measure perceived foot and leg postures during the development of the ischemic block, participants demonstrated the perceived positions of the right ankle and knee using the left foot and leg attached to a flexible two-axis goniometer system. The participants were instructed to demonstrate the perceived ankle and knee positions of their right foot and leg using their left foot and leg. To examine the effects of visual information on the perceived posture of both joints, the participants demonstrated the perceived posture of both joints using their left foot and leg after they looked at their right foot and leg at the end of the block.
The main observation of the present study is that, if the actual foot and leg are fully extended before and during the block, then the joints at the ankle and knee were perceived as flexed in all participants, and vice versa. These results corroborate and extend the findings of our previous studies on the hand and arm (Inui, et al., 2011; Inui, Matsumoto, Beppu, et al., 2012; Inui, Matsumoto, Ueda, et al., 2012) that the final position of the perceived hand depends on its initial position and that the hand and arm are perceived to move continuously with no default position. However, the perceived posture of both joints returns to the position perceived at 0–25 min. after the block after they look at their right foot and leg at the end of the block. Although these results of our study are consistent with the observations of previous studies (Melzack & Bromage, 1973; Paqueron, et al., 2003; Silva, et al., 2010), our study finds for the first time the quantitative effect of visual information on the correction of illusory perception of a limb's position using ischemic block of the limb.
While the multisensory neurons in the parietal and premotor cortices code the position of body parts, they favor visual input over proprioceptive input (for a review, Giummarra, Gibson, Georgiou-Karistianis, & Bradshaw, 2008). The perceived positions of body parts regarding on-line proprioceptive input drift from their actual positions when they are hidden from view (Gross & Melzack, 1978), in particular when they are resting or supported passively in a constant position (Wann & Ibrahim, 1992; Lloyd, 2007) or are passively moved (Botvinick, 2004). However, visual input is not always more accurate than proprioceptive input. The classic finding that vision overrides proprioception only holds for specific conditions and spatial directions. For example, when the visual location of the body part falls within the region where bimodal visuo-proprioceptive neurons in the premotor and posterior parietal cortices encode spatial proximity around the body (peripersonal space; Lloyd, 2007), the posture of the body part is perceived by vision more dominant than by proprioception. Similarly, in the present study, because the visual location of the foot falls within peripersonal space around the foot, visual information corrects the perceived posture of the ankle and knee to the real posture.
Holmes and Spence (2005) have examined the integrative process of visual and proprioceptive information concerning the location of an unseen hand, using a mirror positioned along the mid-sagittal plane. Participants made reaching movements following active visuomotor or passive visual exposure to a mirror, or following passive exposure without the mirror. Reaching was biased more by the visual location following active visuomotor compared to passive visual exposure. These results suggest that visual information is weighted more strongly under active visuomotor experience than under passive visual experience. What participants looked at their right foot and leg at the end of an ischemic block in the present study corresponds to passive visual experience in the study of Holmes and Spence (2005). The effect of visual information on perceived position at the ankle and knee appeared to be weak in the present study. Thus, the perceived posture of both joints did not always return to the initial position before the block after the participants looked at their foot and leg at the end of the block.
Change in Perceived Size of a Phantom Hand
When the sensory input from a body part was removed by peripheral anesthesia, the part was commonly perceived as swollen (Gandevia & Phegan, 1999; Paqueron, Gentili, Willer, Coriat, & Riou, 2004). Such perceptual distortions of body segment size have been linked to loss of input from small-diameter afferents (Calford & Tweedale, 1991). However, it was unclear whether the background firing of the large-diameter fibers was involved. In this section we describe the perceived size of the hand following acute ischemic anesthesia of the upper arm. The form of anesthesia was chosen because ischemic anesthesia developed slowly with loss of conduction in large-diameter axons occurring before that in small-diameter axons.
Perceived size of the hand was estimated by selection of a simple two-dimensional outline or template of the hand, in a neutral position, which best matched its perceived size. Templates of different sizes were randomly arranged on sheets (Gandevia & Phegan, 1999). The range of magnifications was 50% to 190%, in 10% increments, with 100% being the size of a typical adult hand. Participants were asked to “select the template which best matches how big your hand feels or the perceived size of your hand.” The participants chose one template from each of three sheets on each occasion. The participants gave their responses within 10–15 sec. Template selections were made four times prior to cuff inflation and at intervals of 5 min. after inflation.
Fig. 4 shows changes in the perceived size of the hand. Across participants, there was a progressive increase in perceived size which began shortly after cuff inflation. By the end of cuff inflation, the mean increase is 34 ± 4% (mean ± 95% confidence interval).

The mean change in perceived size of the hand during an ischemic block. The solid line represents a regression line of the average of all 10 participants with 95% confidence interval (dashed line). The insets show two templates of the hand to illustrate the magnitude of the average increase in perceived size. Perceived size of the hand was estimated by selection of a simple two-dimensional outline or template of the hand, in a neutral position, which best matched its size. Templates of different sizes were randomly arranged on sheets. The range of magnifications was 50%–190% in 10% increments, with 100% being the size of a typical adult hand. Participants were asked to ‘select the template which best matches how big your hand feels or the perceived size of your hand.’ Participants chose one template from each of three sheets on each occasion. Participants gave their responses within 10–15 sec. Template selections were made 4 times prior to cuff inflation and at intervals of 5 min. after inflation (Modified from Inui, et al., 2011).
Perceived swelling of a deafferented body part has been documented previously after complete anesthesia of the thumb produced by lignocaine (Gandevia & Phegan, 1999). Paqueron, et al. (2003) also found illusions of swelling, enlongation or shortening of the deafferented limb produced by similar compounds. Previous authors (Calford & Tweedale, 1991; Paqueron, et al., 2003) claimed that such perceptual distortion of shape and size of body parts differed cleary from posture illusion. The results of our study suggested that loss of large-fiber input from the hand was sufficient to initiate both the illusion of limb swelling and the alterations in perceived posture of the hand and wrist. However, whereas the mean increase for the perceived size of the hand was 34% in our study, the increase for the perceived size of the finger was 60–70% in Gandevia and Phegan (1999). It is unclear whether this difference is produced by different paralyzed peripheral nerves or by different sizes of the body part (hand and finger).
General discussion
The main findings from a series of studies from our laboratory are that if the fingers, wrist, elbow, ankle, and knee are extended fully before and during an ischemic block, then the body parts finally are perceived as flexed at the joints. Conversely, if the body parts are flexed fully, then the perceived position of the body parts moves toward extension (Inui, et al., 2011; Inui, Matsumoto, Beppu, et al., 2012; Inui & Masumoto, 2013). However, if the hand is held in the mid-position before and during the ischemic block, the posture of the wrist is perceived to be in the same position (Inui, Matsumoto, Beppu, et al., 2012). In addition, after participants look at their foot and leg blocked by cuff inflation at the end of the ischemic block, the perceived posture of both the ankle and knee returns to the position perceived at 0–25 min. after the block (Inui & Masumoto, 2013).
The brain holds an image of the limb that depends on the background sensory input. As input from somatosensory receptors fades during ischemic anesthesia, the perceived limb moves away from its initial position. At an extreme posture, one signal will be high and the other very low so that disappearance of afferents will mainly alter the high signal. As the anesthesia progresses, the stretch receptor activity falls and this fall is interpreted by participants as a change in limb posture. In contrast, in mid-position the firing of afferents signaling flexion and extension is balanced so that as afferent firing disappears, it does so in a balanced way. These observations highlight that the body image as an on-line body representation is updated by moment-to-moment input coming from the body periphery. The key parameter for the illusory changes in limb position may be the difference in discharge rates between afferents in flexor and extensor muscles at a joint.
A series of our studies (Inui, et al., 2011; Inui, Matsumoto, Beppu, et al., 2012; Inui, Matsumoto, Ueda, et al., 2012; Inui & Masumoto, 2013) indicates that the changes in posture of the limb depend on one posture immediately before inflation. This finding suggests that a body image refers incoming proprioceptive information for determination of starting points and endpoints during the generation of movements. In addition, our studies consistently indicated that the change in position did not involve limb postures which are anatomically impossible. This observation suggests that illusory posture is constrained by body maps or representations.
Goodwin, McCloskey, and Matthews (1972) found that if vibration is applied over the belly and the tendon of biceps while the arm is being moved by the experimenter, participants consistently overestimate the angle of extension at the elbow. Albert, Bergenheim, Riot-Ciscar, and Roll (2006) and Roll, Albert, Thyrion, Ribot-Cisar, Bergenheim, and Mattei (2009) further recorded the actual proprioceptive feedback from a series of muscles while participants performed movements. Then the firing frequencies of the muscle spindle afferents were translated into a vibration frequency, and the vibration was applied to participants. The illusory movements mimicked writing or drawing movements. These studies on vibration-induced illusions of movements indicate that awareness of movements matches quite well the information in the muscle spindles. Neuroimaging studies (Naito, Ehrsson, Geyer, Zilles, & Roland, 1999; Naito, Roland, & Ehrsson, 2002) show that the primary motor cortex codes the sensation of movements in the presence of vibration-induced illusions of movements in spite of no performance of movements. In our studies, because a body image constantly referred to incoming proprioceptive information, the results were in part similar to those of the studies on vibration-induced illusions of movements. In contrast to our studies, Craske (1977) showed vibration-induced illusions of movements that were biomechanically impossible to achieve. In addition, Lackner (1988) asks participants to pinch their nose with their index finger and thumb, and vibrated their biceps tendon. The participants then felt that their nose became longer (also see Naito, et al., 2002), indicating that the Pinocchio illusion involves a body shape, i.e., anatomically distorted. Long and Haggard (2010) recently suggested an additional map incorporating the body's metric properties. Although the map is distorted and crudely resembles the maps drawn by Penfield and Boldrey (1937), participants consciously perceived only the undistorted map. It is expected that the different body forms and the distortions will be examined experimentally in the future.
In conclusion, perception of the body seems to consist of information from multiple sensory modalities and the perception forms a body image. Our series of studies indicated that the body image is constantly being updated according to proprioceptive and tactile information. The studies further indicate that visual information overrides the proprioceptive and tactile information in formation of body image.