
Abstract
Since the deinstitutionalization movement, many researchers have suggested that psychiatric patients have moved from one type of institution to another-a process known as transinstitutionalization. This study sought to assess evidence that suggests the mentally ill from Pennsylvania psychiatric hospitals have been transinstitutionalized to penal institutions over the years 1978 to 2010. We gathered data from a number of state agencies and found a significant negative correlation between the incarceration rate and number of psychiatric hospital beds, even after taking into account via partial correlation the changes in population and economic indices such as unemployment and poverty rates in the state. Regression analysis indicated that 6.8% of the year-to-year variation in incarceration rate could be accounted for by the decrease in statewide psychiatric hospital beds after controlling for population and unemployment rate. These transinstitutionalization effects were estimated to cost the state $82.3 million annually. These findings underscore the necessity of providing funding and research towards additional community mental health services for the severely mentally ill so as to avoid adverse outcomes such as incarceration, acute hospitalization, or inefficient state spending. Limitations of the present findings are discussed.
The deinstitutionalization movement as known in the United States began in the late 1940's after the publication of The Shame of the States and a variety of other investigative writings documenting the deplorable conditions of mental institutions (Burnham, 2006). However, the effects of deinstitutionalization, both positive and negative, are still very much relevant and obvious to those who have contact with the mentally ill or find themselves involved in the system that treats the mentally ill.
In order to best discuss the positive and negative outcomes of deinstitutionalization, one has to understand the basic philosophical concepts that were the foundation of the movement. Bachrach (1978) stated that deinstitutionalization asserts a variety of underlying suppositions about mental health care. The first supposition was that community-based mental health services are preferable to traditional institutional treatment settings for the majority, if not all, consumers of mental health services. The second supposition was that communities were able to, and were accepting of, the responsibility to provide for the mentally ill in their communities. The third supposition was that deinstitutionalization is the process of “humanizing” mental health services, the antithesis of institutional care in which a part of the apparent problem was dehumanization.
Deinstitutionalization, in theory, appeared to be a logical and sound concept towards improving the condition and care of mental health patients. However, when one or more of the individual suppositions that supported deinstitutionalization turned out not to be true for either a patient or a community, problems begin to arise. In his research on the Topeka State Hospital Model of care, which became the first model for deinstitutionalization in the United States, Burnham (2006) noted that the complete elimination of the psychiatric hospital was not part of that model. The model was meant only for the deinstitutionalization of patients who could live outside of the hospital with help from community resources; however, the Topeka State Hospital took pride in providing comprehensive innovative services to the severely mentally ill within the hospital setting.
Mowbray, Grazier, and Holter (2002) noted that one of the unforeseen negative consequences of deinstitutionalization was transinstitutionalization. Transinstitutionalization is defined as the moving of mental health clients from one institution, such as a mental hospital, to being dependent on another type of institution, such as a shelter, community hospital, jail, or nursing home facility. McGrew and colleagues (1999) documented transinstitutionalization in their study of the outcome of patients discharged from long-term psychiatric care. They found that after two years, 193 of the 303 (64%) original patients had been transinstitutionalized, ending up in facilities that provided intense monitoring or 24-hour care as well as extensive additional services. After discharge, 20.5% were moved to other state psychiatric hospitals, 1.3% were in penal institutions, 6.3% were in a nursing home facilities, 31.7% were living in supervised group homes, and 4% were in room-and-board facilities.
When a community is unable or is unwilling to support the mentally ill, the ideals and purpose of deinstitutionalization collapse. Rather than enjoying a new life full of freedoms, previously institutionalized patients are unable to handle their own mental health treatment in the community and are faced with the harsh realities of the world viewed through the skewed lenses of their mental illness. Evidence suggests these patients often fall through the cracks of the system, cycling sporadic interludes with a variety of public institutions, such as hospitals and nursing homes. For example, Lamb and Shaner (1993) found that when severely mentally ill patients did not have access to long-term care, they often end up in acute care hospital beds when they decompensate and their condition warrants inpatient psychiatric care. According to Lamb and Shaner (1993) this “revolving-door syndrome” has lead emergency departments to revise their psychiatric admission criteria, which turns away the acutely psychotic who would otherwise be admitted or refers them to overwhelmed community clinics and treatment centers that may not be able to adequately address their psychiatric needs. Lamb and associates (Lamb & Grant, 1982; and Lamb & Lamb, 1990; Lamb, 2003) also have noted the vulnerability of the severely mentally ill to homeless and incarceration related to the vulnerability of these individuals. As deinstitutionalized chronically mentally ill patients became older, many find their way back to the state hospital in their later years and are diverted to nursing home facilities instead (Mowbray, Grazier, & Holter, 2002). Along these lines, chronically mentally ill elderly patients are sent frequently to nursing home facilities straight from a state hospital. Often these nursing homes are not equipped to handle the psychiatric issues these patients bring with them.
Evidence also suggests that deinstitutionalized patients may also end up in penal institutions. This phenomenon, the focus of the present investigation, is explored below.
Criminalization of the Mentally III
White and Whiteford (2006) argued that correctional facilities are quickly becoming the psychiatric institutions of the 21st century. According to the U.S. Department of Justice, 64% of those incarcerated in jails, 56% of state inmates, and 45% of federal prisoners exhibit symptoms of severe psychopathology such as bipolar disorder, major depression, or schizophrenia (Federal Surveys, 2006; Peternelj-Taylor, 2008). Mowbray, et al. (2002) reported that the criminalization of the deinstitutionalized mentally ill happens when individuals who have not been able to receive help through psychiatric hospitalization begin to disturb their communities either because they engage in survivalist behaviors (e.g., loitering, stealing, or trespassing) or through their unusual behaviors. Without structure and adequate community mental health care, some severely mentally ill patients are arrested for committing minor crimes, which are often reflective of symptoms of their psychiatric illness (Lamb, Sorkin, & Zusman, 1981). Then again, minor crimes might be committed purposefully by the mentally ill as a means of seeking shelter. Lamb and Shaner (1993) indicated that breaking the law may be a means of seeking help for many chronically mentally ill people who are not receiving adequate services. One study conducted by Lamb and Grant (1982) found that 50% of the psychiatric population in a jail for committing minor crimes had been homeless prior to their arrest. On the other hand, it is possible that crimes committed by mentally ill individuals could be viewed as medical problems reflecting on behavior, thus reducing one's responsibility for actions.
In order to better address the needs of the mentally ill who commit crimes in the community, some police jurisdictions have set up specialized teams to deal specifically with psychiatric emergencies. One such law enforcement-mental health team was studied by Lamb, Shaner, Elliott, Decuir, and Foltz (1995) in order to determine outcomes for mentally ill offenders when the team responded to psychiatric emergencies. The study found that of the 101 emergencies handled by the team, 72.2% of the mentally ill offenders were taken to the hospital for treatment, 25.7% were given appropriate outpatient referrals, and only 1.9% were sent to jail. On a six-month follow-up of 85 of the original participants, 24% had reoffended and were arrested. Lamb and colleagues speculated that this may be because the mentally ill offender was encountered in the community by a police officer without a mental health professional on second contact. However, a positive outcome was that 66% of the sample was reported to be still receiving mental health services either in the community or in appropriate facilities at the six-month follow-up. Homelessness, reported at the six- month follow-up, had decreased from 33% of the sample to 11%. Lamb, et al. concluded that the majority of the mentally ill offenders were finally receiving services that they needed to address their psychiatric issues.
Since 1995, other areas have recognized the value of diverting the mentally ill from the criminal justice system, but in Miami-Dade County, Florida, diversionary programs have become a necessary part of the judicial process due to the sheer number of mentally ill people who commit crimes. Miami Dade County has the highest urban concentration of mentally ill people in the United States (Perez, Leifman, & Estrada, 2003). Since less than 13% of this population actually receive psychiatric treatment, the mentally ill were twice as likely to be in the county jail as at the state hospital that serves Miami-Dade County. Miami-Dade County not only has a pre-arrest diversionary program similar to the one noted in the study conducted by Lamb, et al. (1995), but it also has a post-arrest diversionary program. In this program, mentally ill offenders are quickly evaluated by psychiatric professionals to determine if they should be sent to mental health crisis units for care or if they should be expedited to mental health court. At mental health court, offenders are put on probation with probation officers trained to handle mental health cases. They are also referred to Assertive Community Treatment teams that provide for psychiatric care, substance abuse rehabilitation, and case management services as well as social and vocational rehabilitation (Perez, et al., 2003). The objective of these diversionary programs is to reduce recidivism among the severely mentally ill by meeting their unmet needs through community health resources without criminalizing them.
While the aforementioned studies highlight the importance of diverting psychiatric patients to appropriate mental health services, the ability to divert mental health patients from the criminal justice system to community health systems also reduces the cost to society as a whole. According to Lamberg (2005), inmates with mental illness are incarcerated five times longer than the average inmate and cost almost twice as much as average inmates per day to keep incarcerated. Lamberg also pointed out that according to the Pennsylvania Department of Corrections, the annual cost per each mentally ill inmate is $51,000 compared to the annual cost of $10,000-$20,000 to provide services, a job, shelter and food in the community for a mentally ill adult. The aforementioned Miami-Dade County program estimates a substantial savings since the start-up of their post-arrest psychiatric diversionary program accomplished simply through redirecting psychiatric patients to mental health services rather than sending them to local jails and the traditional court system (Perez et al., 2003).
Incarcerating the severely mentally ill is not only a costly endeavor, but it also often fails to provide any correctional benefits to the mentally ill person. It also can be seen as a way of “disowning responsibility” (Sheth, 2009). Peternelj-Taylor (2008) identified several factors that make penal institutions markedly disadvantageous to the mental health population. First, correctional staff usually has limited knowledge of mental health issues and appropriate interventions. Second, often the mentally ill do not understand the rules of the prison or lack the ability to follow orders. Third, mentally ill inmates often become easily identifiable targets for other inmates to victimize and are often subjected to harassment, physical assaults, and sexual assaults. Forth, many policies and procedures used by prisons in an attempt to keep those with psychiatric disorders safe (e.g., restraint, seclusion, segregation) are often detrimental to the mentally ill inmate's physical and mental health (Peternelj-Taylor, 2008).
Criminalization of the mentally ill can lead to a variety of adverse outcomes for both the mentally ill offender and society as a whole. While some areas of the United States have recognized that criminal or disruptive behavior may be a signal that the mentally ill offender needs proper or more intensive mental health care, other places have no diversionary programs to keep the mentally ill from becoming incarcerated. Regrettably, people with severe psychiatric disorders receive no therapeutic or social benefit from having been incarcerated and may end up suffering from more physical and psychological damage from the experience. Keeping people with chronic mental illness in penal institutions is also costly to society. For these reasons and many others, it is necessary to establish whether transinstitutionalization of the mentally is occurring so as to reduce undesirable effects for the mentally ill, correctional facility administrators, staff, and society as a whole.
Previous Studies on Transinstitutionalization from State Hospitals to Penal Institutions
Previous studies have sought to determine if there is a statistical relationship between the closure of state hospitals and the increased use of correctional facilities. Palermo, Smith, and Liska (1991) examined the relationship between the number of people in jails and prisons and the number of psychiatric patients in mental hospitals around the United States. The researchers used 41 discontinuous years of data and found a correlation of −.45 between the number of people in hospitals for psychiatric reasons and people in jails and prisons. They also found a correlation of −.51 between the number of mental health patients in psychiatric institutions and the number of inmates entering jails and prisons. Although correlational data cannot be interpreted as causal, these documented associations do suggest that transinstitutionalization is occurring. Palermo and colleagues (1991) also underscored that penal institutions provided no therapeutic value to the mental health population and that appropriate interventions within the penal institution to keep these individuals from committing additional crimes was highly unlikely.
However, another study by Banks, Stone, Pandiani, Cox, and Morschauser (2000) did not find a significant relationship between the closure of state hospitals and increased incarceration rate. They examined data from 17 counties in New York State over a two-year period after the closing of a state hospital that served the mentally ill of those counties. The authors' posited that if patients released from state hospital care utilized general hospitals and correctional facilities more in their second year in the community than the year in which they were released, transinstitutionalization effects would be occurring. They found in the two years after the closing of the state hospital that both men and women were more prone to being incarcerated during their first year after their release from the state hospital (16–27% and 6–18.2%, respectively) than in their second year in the community (11.4%-17.2% and 3.7%-13.5%, respectively). General hospital usage by previously institutionalized men and women also had a similar pattern, with between 30–41% of men and 40–46% of women being treated in the general hospital for psychiatric care in their first year out of the state hospital; in comparison with 10.6%-25.1% of men and 24.8%-35.8% of women in their second year out of the state hospital (Banks, et al., 2000). Thus, the results were contrary to the hypothesis of transinstitutionalization.
It should be noted, however, that Banks, et al. (2000) followed two groups of individuals for two years after their release from a long-term state psychiatric facility. This study did not address what happened to this population five, ten, or fifteen years after state hospital care had been discontinued. It also did not assess what happens to chronically mentally ill people who previously would have met criteria for admission to state hospital treatment who now need to look to the community for care or risk adverse outcomes such as homelessness, incarceration, or lack of effective psychiatric treatment. While the study provided an example of what happens to the psychiatric population in New York in the years immediately following release from a long-term psychiatric facility, the data cannot be generalized to the next generation of mentally ill people who now have no option for long-term inpatient psychiatric care.
Similarly to the findings of Banks, et al. (2000), Severson (2000) concluded that transinstitutionalization of the mentally ill in Kansas was not occurring. Severson sought to assess if incarceration rates had increased at local jails around the state of Kansas before and after the closure of the Topeka State Hospital. Severson sent surveys to 101 sheriffs asking them to report on a variety of statistics including admission screening, staff training, relationships with community mental health services, and the number of inmates they had with a “Serious and Persistent Mental Illness (SPMI)” in their facilities in 1995, 1996, and 1997, the year the state hospital closed. A total of 54 (51%) of the surveys were returned, and 80% of the jails indicated that in 1997 they had incarcerated the same number or fewer inmates with SPMI than in 1995. However, the sheriffs also reported that 68% jails had no formal written screening for mental illness upon admission and that 71% of their staff had no mental health training. It is possible, therefore, that the data on SPMI were underreported.
The Present Study
Based on the available literature, there are two important issues regarding care of the chronically mentally ill and transinstitutionalization that have yet to be addressed. Since the majority of literature suggests that transinstitutionalization from mental health facilities to penal institutions has been occurring among people with persistent mental illness (Palermo, et al., 1991), the present study explored if transinstitutionalization effects are occurring within the state of Pennsylvania. We predicted that there would be a negative relationship between available state psychiatric hospital beds and the Pennsylvania state incarceration rate. Further, assuming transinstitutionalization is occurring, a second area of investigation was to determine whether budgeting was significantly related to the deinstitutionalization of the state's mentally ill. Specifically, Beecham and colleagues (2004) posited that transinstitutionalization of the mentally ill costs governments less than providing around-the-clock hospital quality staffing geared toward psychiatric issues for the chronically mentally ill. Therefore, we predicted that there would be a negative relationship between institutional mental health spending and the penal incarceration rate, which would provide evidence that transinstitutionalization occurs in a manner related to cost. We predicted that there would be a positive relationship between the incarceration rate and spending on incarcerating Pennsylvanians, reflecting a possible budgetary shift from mental health services to the penal system to adjust for the mentally ill who have been subjected to transinstitutionalization effects.
Variables
For each of the following variables data were collected for as many years as available from 1970 to 2010.
Number of available psychiatric hospital beds per year in Pennsylvania.—We derived data for the number of state psychiatric hospital beds available per year from the Pennsylvania Department of Health's Annual Hospital Questionnaire which is available to the public at the Pennsylvania Department of Health's website (Pennsylvania Department of Health, 1978–2009). We added specialty and federal psychiatric hospital beds to the number of psychiatric beds from local acute care hospitals as reported in the Annual Hospital Questionnaire.
Pennsylvania's population.—We obtained the Pennsylvania state population per year from The United States Census Bureau's (2010a) Population Estimates tables for 1970 through 2009, available to the public on the agency's website.
Pennsylvania's incarceration rate.-The incarceration rate for Pennsylvania was obtained from the Pennsylvania Department of Corrections Annual Statistical Reports which can be found on the agency's website (Pennsylvania Department of Corrections, 1990, 1997–2009).
Pennsylvania's poverty rate.-The poverty rate for 1980 through 2009 was obtained from the U.S. Census Bureau's (2010b) Current Population Survey, Annual Social and Economic Supplement available in their online archives.
Pennsylvania unemployment rate.-The economic climate, measured by unemployment rate for the years 1970 through 2009, was obtained from the United States Department of Labor's (2010) website.
Pennsylvania's annual spending on community mental health programs and institutional mental health programs.-For the financial data variables, all of the data were derived from the Pennsylvania State Budget documents. To best determine how the Pennsylvania State Budget's mental health appropriation was divided between spending on state hospital care for psychiatric patients and community mental health funding, the Department of Public Welfare's Department of Public Welfare Budget Request was used to find the yearly spending for state hospital care and community mental health services. These records are available to the public, by appointment only, upon request at the Department of Public Welfare's budget office in Harrisburg, Pennsylvania (Pennsylvania Department of Public Welfare, 1979 1994, 1998, 2000–2008, 2010).
Pennsylvania's annual spending on incarcerating Pennsylvanians.-The amount of state funds used for Pennsylvania State correctional facilities was drawn directly from the annual Pennsylvania Governor's Executive Budget's correctional institutions appropriation figure (Pennsylvania Office of the Budget, 1974–2010). The Pennsylvania State Budget is also available to the public upon request at the Pennsylvania State Library located in Harrisburg, Pennsylvania.
Procedure
To test the predictions above, which are expected if transinstitutionalization effects had been occurring, we correlated the numbers of state hospital beds available for psychiatric patients per year with the yearly prison population for local jails and state prisons in Pennsylvania over the years between 1970 and 2010. Other variables included in the Pearson's correlation analysis were the state's population, poverty rate, and economic climate measured by the state's annual unemployment rate. To estimate the effects of budgeting on transinstitutionalization, we examined the number of psychiatric hospital beds and the incarceration rate in relation to spending on incarceration, community mental health spending and institutional mental health spending.
To further evaluate the contributions of various variables to the change in the state's incarceration rate over the years, we entered the following variables as predictors in a hierarchical regression model: yearly state population; yearly state unemployment rate; the number of available state psychiatric hospital beds yearly; and the state's yearly spending on penal institutions, community mental health, and state hospitals.
Results
A Pearson's correlation was used to characterize the relationship between Pennsylvania's incarceration rate and the number of available psychiatric hospital beds in the state, while controlling for state population, poverty rate, and state unemployment rate. First, there was a negative correlation between yearly incarceration rate and number of available psychiatric hospital beds (r23 = −.97, p< .001). Fig. 1 illustrates how the values of these variables changed over 40 years in the opposite directions. We also found correlational relationships between yearly incarceration rate and unemployment rate (r25 = −.74, p< .001) and between psychiatric hospital beds available and the state's unemployment rate (r30 =.54, p< .01). In addition, we found significant correlations between yearly state population and incarceration rate (r28 =.87, p< .001) and between yearly state population and number of available psychiatric hospital beds (r32 = −.84, p< .001). However, the correlation between yearly poverty rate and incarceration rate was not significant (r23 = −.38, p = .07), nor was the correlation between yearly poverty rate number of available psychiatric hospital beds (r30 =.33, p = .08).

Pennsylvania incarceration rate and the number of available psychiatric hospital beds in Pennsylvania per year (r23 = −.97, p< .001).
To further elucidate the relationship between incarceration rate and the number of psychiatric hospital beds available, we conducted a partial correlation to control for the changes in state unemployment rate, population, and state poverty rate. We found that even after controlling for these variables, incarceration rate and the number of psychiatric hospital beds still exhibited a strong negative correlation (r18 = −.87, p< .001).
To characterize the relationship between spending and transinstitutionalization, we conducted further correlational analyses and found significant positive correlations between incarceration rate and institutional mental health spending (r =.87, p< .001); incarceration rate and community mental health spending (r21 =.99, p< .001); and incarceration rate and spending on incarceration (r28 =.99, p< .001). In addition, we found significant negative correlations between the number of state psychiatric hospital beds available and institutional mental health spending (r26 = −.74, p< .001), community mental health spending (r26 = −.91, p< .001), and spending on incarceration (r32 = −.94, p< .001).
In order to further assess the extent to which the number of psychiatric hospital beds available and budgeting were related to the deinstitutionalization and transinstitutionalization process, we used a statistical hierarchical regression to examine the predictive values of the number of psychiatric hospital beds and the three budgeting variables with respect to the incarceration rate by controlling for population and unemployment rate. Poverty rate was dropped from this model as it appeared to be creating multicollinearity problems when it was included in the analysis with unemployment rate. The summary for this hierarchical regression can be found in Table 1. Statistics for the regression's coefficients can be found in Table 2. The regression analysis indicated that state population explained 89% of the variance in the incarceration rate (R2 =.89, F1,19 =147.33, p<.001). State unemployment rate explained 3% of the variance (R2 =.03, F1,18 =7.78, p<.02), after controlling for state population. The number of available psychiatric hospital beds accounted for approximately 7% of the variance (R2 =.07, F1,17 =97.06, p<.001), after controlling for population and unemployment rate. Spending on incarceration, community mental health spending, and institutional mental health spending combined explain only 1% of the variance (R2 =.01, F3,14 =15.43, p<.001), after controlling for state population, unemployment rate and available psychiatric hospital beds.
Transinstitutionalization Model Summary Predicting Change in Incarceration Rate

Notes.
Predictors: (Constant), Pennsylvania Population
Predictors: (Constant), Pennsylvania Population, Pennsylvania Unemployment Rate
Predictors: (Constant), Pennsylvania Population, Pennsylvania Unemployment Rate, the number of Pennsylvania Psychiatric Hospital Beds
Predictors: (Constant), Pennsylvania Population, Pennsylvania Unemployment Rate, the number of Pennsylvania Psychiatric Hospital Beds, Pennsylvania state funds spent on Institutional Mental Health, Pennsylvania state funds spent on Community Mental Health, Pennsylvania state funds spent on Incarcerating Pennsylvanians
Coefficients for the Transinstitutionalization Model Predicting Change in the Incarceration Rate a
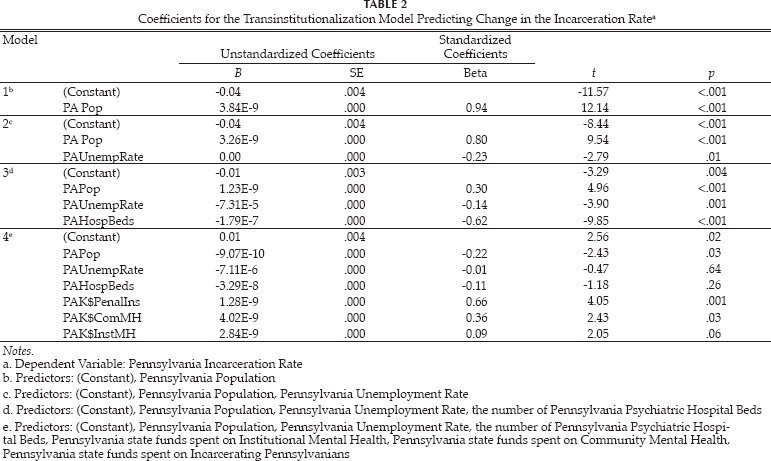
Notes.
Dependent Variable: Pennsylvania Incarceration Rate
Predictors: (Constant), Pennsylvania Population
Predictors: (Constant), Pennsylvania Population, Pennsylvania Unemployment Rate
Predictors: (Constant), Pennsylvania Population, Pennsylvania Unemployment Rate, the number of Pennsylvania Psychiatric Hospital Beds
Predictors: (Constant), Pennsylvania Population, Pennsylvania Unemployment Rate, the number of Pennsylvania Psychiatric Hospital Beds, Pennsylvania state funds spent on Institutional Mental Health, Pennsylvania state funds spent on Community Mental Health, Pennsylvania state funds spent on Incarcerating Pennsylvanians
Discussion
Implications for Behavioral Health
Similar to the work of Palermo and colleagues (1991), the current study investigated possible evidence for transinstitutionalization effects in Pennsylvania, related to shifting of mental health patients from psychiatric hospitals to penal institutions. Further, we examined the extent to which the Pennsylvania state population, the number of available psychiatric hospital beds, unemployment rate, and state budgeting were statistical predictors of the incarceration rate in Pennsylvania. It was hypothesized that a decrease in state psychiatric hospital beds would be associated with a significant increase in the Pennsylvania incarceration rate, and the data supported this prediction. The strong negative relationship between incarceration rate and hospital beds suggests that transinstitutionalization of the mentally ill has been occurring in Pennsylvania. Additional analyses provided evidence that the strong negative correlation consistent with the transinstitutionalization hypothesis was not related to population increase or changes in unemployment rate and poverty rate.
We also found positive relationships between the incarceration rate and all of the budgeting variables, suggesting that spending has increased for institutional mental health, community mental health, and incarceration. Incarceration rates have increased during this time and a positive correlation would be expected for incarceration spending, similar patterns were noted on community health and even institutional health spending. Thus, the positive correlations between incarceration, community health, and institutional mental health may reflect budgeting trends.
While the negative relationship between psychiatric hospital beds and institutional mental health spending did not support the present hypothesis, these data indicate the deinstitutionalization movement's basic principle of saving money has not actually occurred as budgeting administrators had planned that it would. The increased cost of institutional care, in spite of the extreme reduction in long-term psychiatric facilities and psychiatric hospital beds, substantially decreasing from 19,107 in 1978 to 5,238 in 2009, may be due to the rising cost of staffing and maintaining each individual psychiatric bed.
We further evaluated the effect of budgeting during the deinstitutionalization process and found that financial variables account for less than 1% of the incarceration rate in the model. This suggested that budgeting had limited contribution to the process of transinstitutionalization in Pennsylvania. Most of the variation of incarceration rate can be explained by population changes, but we also found that slightly less than 7% of Pennsylvania's incarceration rate changes could be attributed to by the decrease in hospital beds. This model suggested that transinstitutionalization of the mentally ill has been occurring in Pennsylvania. As expected, the significant relationship between the incarceration rate and incarceration spending indicated that an increase in spending on incarceration has occurred as more citizens have become incarcerated. The marginal relationship between institutional mental health spending and incarceration rate was contrary to prediction, but supported the concept that spending variables have little influence on the current incarceration rate.
The findings of this study corresponded with those of Palermo, et al. (1991) who hypothesized a negative relationship between psychiatric hospital population in United States and the national prison population, indicating evidence for transinstitutionalization of the mentally ill from hospitals to penal institutions. Palermo, et al. (1991) found a negative correlation between hospital population and prison population, similar to the present study's negative correlation between Pennsylvania's incarceration rate and the number of psychiatric hospital beds available to Pennsylvanians. Some prior studies have not found evidence for the deinstitutionalized mentally ill being transinstitutionalized to penal institutions (Banks, et al., 2000; Severson, 2000). However, the limited window of examination of these previous studies may have played a role in these findings. Palermo, et al. (1991) analyzed 41 discontinuous years of data to test their hypothesis and found evidence for transinstitutionalization, while Banks, et al. (2000) and Severson (2000) studied transinstitutionalization within only two years and one year, respectively, of their samples being deinstitutionalized. Similar to Palermo, et al.'s work, the current study gathered all of the data available for each study variable during 40 contiguous years between 1970 and 2010, and 20 years within this time frame had values available for all of the research variables. This indicates that transinstitutionalization effects might best be observed over longer periods of time as opposed to immediately after the deinstitutionalization of the mentally ill.
The current study included data from the crucial time period during which deinstitutionalization occurred in Pennsylvania, starting in 1979 and continuing through the present with the closing of Allentown State Hospital in December, 2010, as well as data prior to and following deinstitutionalization of the mentally ill. Since deinstitutionalization has occurred at different times for different states, it is important that one state such as Pennsylvania was used for this research so the years vital to deinstitutionalization as well as those preceding and following could be identified and used in research. The study also assessed how much of the current incarceration rate might be accounted for by deinstitutionalization effects.
For many governments and administrative personnel, deinstitutionalization has been as important a financial issue as it has been one of humanitarian concern. The current study has many implications for the state of Pennsylvania. We found that nearly 7% of all incarcerations in Pennsylvania could be accounted for by the decrease in psychiatric hospital beds available within the state. The economic climate of the state accounted 5% of the incarceration rate in Pennsylvania. Lamberg (2005) noted that it costs twice as much to incarcerate the mentally ill of Pennsylvania and the incarceration length for mentally ill individuals was found to be nearly five times longer than that of the average inmate. This study's results, and the data of most other researchers, suggest there is increased incarceration in the criminal justice system of individuals with severe mental illness. The criminal justice system, as a result, often becomes the treatment agency of last resort for severe mental illness. However, one wonders if the more direct provision of psychiatric treatment could bring greater benefit to the patient, and indirectly to society at large.
Between 1990 and 2010 there has been a six-fold budget increase for penal incarceration in Pennsylvania; the cost of penal incarceration in Pennsylvanians in 1990 was $333.3 million in contrast to the $1.7 billion budgeted in 2010. In comparison, community mental health spending has doubled in the same amount of time, rising from $167.3 million dollars in 1990 to $376.2 million in 2010. Within this same 20-year period, institutional mental health spending has only decreased by 10%, with $367.3 million being spent on mental institutions in 1990 compared to $334.0 million budgeted for 2010. This leads one to question whether or not deinstitutionalization has provided the financial benefits that were intended, considering that a 10% savings in institutional mental health has occurred in a time frame of a 6-fold increase in prison spending. Even when one considers the combined cost of both community and institutional mental health in Pennsylvania, $710.3 million dollars in 2010, it still pales in comparison to the $1.7 billion budgeted to imprison Pennsylvanians; for every dollar spent on mental health, $2.46 are being spent on penal institutions in Pennsylvania. In other words, for a “savings” of $33.3 million dollars in institutional mental health per year, incarcerating mentally ill Pennsylvanians costs the state $115.6 million per year. Thus, the estimated effect of transinstitutionalization of the mentally ill costs the state of Pennsylvania $82.3 million dollars per year. These findings suggest that significant savings could be obtained by merely having provided appropriate mental health services to the incarcerated Pennsylvanians who have suffered the effects of transinstitutionalization. Tests are available to researchers to detect when an individual has the potential to engage in criminal behavior (Zagar, Busch, Grove, & Hughes, 2009), and thus it is puzzling why these formal, actuarial assessments are not frequently employed, as the financial costs of such would be minimal compared to the costs to society in terms of victimization and burden on the justice system (Zagar, Zagar, Bartikowski, Busch, & Stark, 2009).
Limitations
This research and the interpretations have limitations, the primary of which is the reliance upon correlational and regression analysis to establish evidence of transinstitutionalization. In this study's epidemiological approach it was found that available psychiatric hospital beds in Pennsylvania accounted for approximately 7% of the variance in incarceration. Along these lines, another limitation to this study's interpretation is that it is entirely possible that the individuals who have been incarcerated are not the same individuals who may have been residents of psychiatric hospitals. The present study, therefore, is a small step towards assessing if transinstitutionalization is occurring. Although a challenging task logistically, and perhaps ethically, it would be prudent to document the long-term or lifetime progress and/or placement of individuals released from psychiatric hospitals with respect to arrest rates, progress, and outcomes of community supervision programs and non-residential mental health care.
This study used the number of available psychiatric hospital beds yearly in Pennsylvania as an indicator of state hospital availability and use. Notably, this number does not specify the exact number of people hospitalized in a PA state psychiatric institution in a given year, or whether or not a single individual returned to a psychiatric institution. Nonetheless, the authors contend that the present findings serve as an impetus to study transinstitutionalization more in-depth and long-term, where and if possible.
Another limitation faced was the lack of accessibility to older data. Though the researchers gathered as much data as possible from state and federal agencies, with the exception of Pennsylvania state population and unemployment rate, data 35 years or older were not available for the remainder of variables being studied. In addition to the limited number of years being studied, 1970–2010, some Pennsylvania state agencies had limited or incomplete records, thus creating gaps within the data set for certain variables, such as incarceration rate, as well as community and mental health spending. Even so, there have been considerable earlier research (e.g., Steadman, Cocozza, & Melick, 1978; Robins, Hanin, Moore, & Wainwright, 1977) which noted very similar patterns of transinstitutionalization effects.
The results of the study on transinstitutionalization in Pennsylvania may demonstrate patterns that could be found in other U.S. states, but the generalizability of the results to other states is uncertain. Since deinstitutionalization has occurred at different times in different states, and laws vary by state, especially those pertaining to the mentally ill and deinstitutionalization, one should be cautious in assuming that transinstitutionalization effects are occurring in other states or on a nationwide basis in the United States.
A final limitation of this study was multicollinearity within the original study design that required one of the control variables, poverty rate, be dropped from the analyses.
Conclusions
This study suggests the need for future research on transinstitutionalization effects within several states or on a national level. Intensive individual follow-up of discharged individuals in a participant observer or a similar qualitative model may be useful in helping to discern the actual life course for discharged individuals from mental health care. Another possible direction for future research could be in identifying elements essential for successful community tenure of severely mentally ill people. In addition, it would be prudent to conduct research that can assist in identifying services (e.g., social, medical, financial) or types of professionals (e.g., case managers, social workers, psychiatrists, psychologists) critical to proper community care and to help avoid adverse outcomes such as acute hospitalization or incarceration. Moreover, future research could focus on aspects of mental illness more likely to lead to undesirable outcomes, such as hospitalization or incarceration, in an attempt to develop interventions or strategies to cope with this symptomology to prevent unfavorable outcomes. A final direction that future research could take is in focusing on tracking and helping the next generation of mentally ill individuals.
As Talbott (1974) stressed, institutional biases must be eliminated, and should institutional services such as state hospitals be closed or phased down, alternative community services must be provided to combat the problems caused by deinstitutionalization. Since the advent of deinstitutionalization, only a small percentage of the most severe psychiatric patients will ever be admitted into long-term institutional care. Research with a focus on interventions for children, teenagers, and young adults experiencing severe psychopathology would be beneficial to inform policy-making that will ensure adequate mental health care for this demographic and to prevent this population from becoming institutionalized in penal institutions.