
Abstract
An eight-item questionnaire was administered to 55 patients of a Canadian methadone clinic (34 men, 21 women) to self-rate their desire to relax in or around the clinic, chat with peers, enjoy the sense of community with fellow addicts, and rate the relative importance they may attribute to this part of their daily routine. Total score for loitering tendency was significantly correlated to scores on the Alcohol Use Disorders Identification Test (r=.39) and on the Drug Abuse Screening Test (r=.29) but not to results of urine tests for cocaine, opiates, and benzodiazepines, or to the psychopathology scales of the Symptom Checklist-90-Revised, or to age or sex. The loitering may express an unmet need for peer support.
Loitering of patients at the entrances of methadone clinics has caused great concern both to the surrounding communities and to the medical staff for several decades. An early study in New York by Barnes, Aloizou, Hanbury, and Stimmel (1983) examined the characteristics of 190 patients identified as “loiterers” as compared to a matched control group of other methadone patients who showed no loitering tendencies. Loiterers were significantly (p <.005) more often involved in criminal activities (φ =.20), non-opioid substance abuse (φ =.09), and less often in productive activities (φ =.13). However, these correlations are extremely weak. They reached statistical significance only due to an extremely large sample size (N = 1, 064). No significant relationship was found to concurrent alcohol abuse, arrests, or positive urine tests (all φ <.09).
Witte (1993) warns researchers that very large samples could lead to significant correlations that lack practical importance. Therefore it is important to replicate Barnes, et al.'s (1983) findings. We conducted correlations of a self-reported tendency to spend extra time at a methadone clinic to scores on measures of addiction, to scores on a questionnaire measure of psychopathology, and to urine tests for concurrent substance abuse in a clinic in a Canadian setting.
Method
Participants
The sample consisted of 34 men and 21 women (M age = 34.3 yr., SD = 9.0, range = 19–55). They were randomly selected in an urban methadone clinic in Canada. All participants were diagnosed by addiction psychiatrists as meeting DSM–4 criteria for the diagnosis of opioid dependence.
Measures
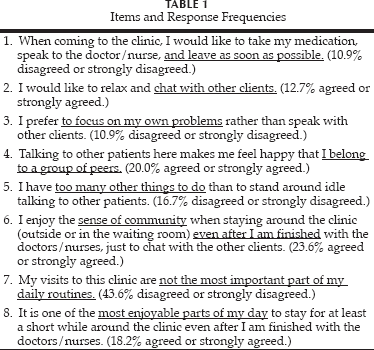
All participants completed an eight-item questionnaire (see text in Table 1) to measure their desire to spend more time in the immediate vicinity of the clinic. The items were rated on a scale with anchors 1: Strongly agree and 5: Strongly disagree. Their urine tests for cocaine, benzodiazepines, and opiates for the last 8 wk. were available. All also completed the Symptom Check List-90-Revised (SCL-90–R, see Derogatis, 1983), the Alcohol Use Disorders Identification Test (AUDIT, see Saunders, Aasland, Babor, de la Fuente, & Grant, 1993), and the Drug Abuse Screening Test (DAST–20, see Gavin, Ross, & Skinner, 1989).
Items and Response Frequencies
Results
The proportions of those endorsing any of the eight items in the direction suggestive of a potential for loitering are listed in Table 1. The total score was calculated after the items worded in a negative sense were recoded to indicate a subjective need for spending more time at the clinic. This score was significantly correlated (p <. 05, two-tailed) with the patients' scores on the AUDIT (Pearson's r =.39) and the DAST-20 (r =.29) but neither to results of urine tests for cocaine, opiates, and benzodiazepine nor to psychopathology scales of the SCL-90–R nor to age or sex.
Barnes, et al. (1983) found that loiterers at their clinic were somewhat more likely than other methadone patients to be involved in criminal activities (29 vs 11%, respectively, p <. 001). In our study, significant correlations (p <. 05, one-tailed) were found of the total score on our eight-item questionnaire to the following items of the DAST-20 that inquire about criminal or violent acting out: Item 14, “Have you gotten into fights when under the influence of drugs?” (r =.33, p =.01); Item 15, “Have you engaged in illegal activities in order to obtain drugs?” (r =.25, p =.04); and Item 16, “Have you been arrested for possession of illegal drugs?” (r =.25, p =.04).
The validity of our measure of loitering tendency has not yet been tested. With respect to other psychometric properties of the eight-item questionnaire, its Cronbach's a coefficient of internal consistency calculated on our sample was.65; i.e., within the range usually considered acceptable for research instruments.
Discussion
As did Barnes, et al. (1983), we found that the loiterers were somewhat more likely to have a criminal history. However, both our correlations and those reported in Barnes, et al. are weak.
In the present study, the tendency to loiter at the clinic was not significantly associated with concurrent substance abuse, except for a moderate correlation to alcohol use measured via AUDIT. In the study by Barnes, et al. (1983), only extremely weak correlation of loitering to non-opioid abuse was found, at the level below relevance for practical clinical predictions (φ =.09), and no significant relationship was detected to alcohol abuse. The relationship of loitering to DAST-20 measures of addiction in our sample was statistically significant but weak.
The lack of correlations to SCL-90–R measures of psychopathology in the present study suggests that the tendency to loiter could not be satisfactorily explained by psychiatric symptoms other than addiction.
The weakness of the present study lies in its extensive reliance on self-reports, except for laboratory data provided by urine tests. The contribution of this study consists in providing statistics, suggesting that factors such as concurrent substance abuse, criminal history, DAST–20 scores, or psychopathology other than addiction do not adequately account for the tendency of some patients to loiter in the proximity of the methadone clinic.
It is possible that some methadone patients have an unmet need for peer or emotional support that might perhaps be awkwardly expressed by spending more time than strictly necessary at the methadone clinic. If this hypothesis would be confirmed by further research, then more frequent encouragements for such patients to join self-help groups such as the Narcotics Anonymous or to participate in group psychotherapies may be beneficial.