
Abstract
Herein, a case of olfactory reference syndrome is presented. The Rorschach test findings were interpreted using Exner's method (2003) and Lerner's object relations perspective, which integrate Piaget's theory of early cognitive development with Mahler's theory of separation-individuation. Based on such Rorschach interpretations and other psychological tests, the olfactory reference syndrome was found to be similar to psychotic disorders. Clinicians and researchers should be aware of this similarity when treating patients suffering from olfactory reference syndrome.
Olfactory reference syndrome is a nonorganic psychiatric disorder in which the chief complaint is the patient's awareness of his body odor that surrounding people do not detect. This condition poses diagnostic difficulty. If the patient perceives a smell, it may be an olfactory hallucination, and the condition should be categorized as psychotic disorder despite few other psychotic symptoms that might suggest a diagnosis of schizophrenia. If the awareness does not come from his own perception of the smell, but from his hypersensitivity regarding other people's behaviors that are viewed as insinuation of the smell, the condition may be categorized as social phobia. Many patients with olfactory reference syndrome are refractory to therapy and such patients are likely to stop treatment. Therefore, it is necessary to understand the pathogenic mechanism through methods other than descriptive psychology. The Rorschach test and other tests utilizing projective techniques can help the psychotherapist to recognize the inner psychological state of a patient; however, these tests have been seen as lacking validity or reliability (Wood & Lilienfeld, 1999). In the present study, a case of olfactory reference syndrome is presented, and its pathology is discussed based on the results of the Rorschach test interpreted using Exner's method (2003) and Lerner's object relation perspective (1996).
Case presentation
The patient, in his late twenties, was a trainee in a profession and was the second born of three siblings. All of his family members were also in the same profession. He was referred to my office after visiting a psychiatric clinic and reported that he had been concerned with the smell of his armpits for 10 years. As a result, he could not go to his office or use a computer system for his job and took several showers per day. Even though he had undergone a dermatological procedure on his armpits some years previously, he remained convinced that his armpits smelled bad. He said that he wanted to eliminate the bad odor by undergoing the procedure again. The patient cancelled his next session and did not contact the office to schedule a further consultation. However, some months later, he suddenly called and came for an appointment. He said that he made an unscheduled visit to a different dermatologist and asked him to perform the same procedure on his armpits. However, the dermatologist refused to perform the procedure because it might have negative physical consequences in the future, but he went to another clinic for the procedure, anyway. Consequently, he indicated a desire to resume our sessions because he wanted to change the way he thinks about his body odor. He said that his problem was based on his actual physical condition, and emphasized that he was wrong to think that his armpits smelled badly. It was unclear whether his problem was a delusion or due to anxiety. Therefore, he completed the Rorschach test, the sentence completion test, and the house-tree-person test, which comprise a common test battery used in the psychological clinical setting (Exner, 2003). The patient completed all tests after providing informed consent to participate in psychotherapy.
Method and Results
Measures
Rorschach Test. A subject's interpretations and perceptions of a series of standard inkblots are analyzed as an indication of personality traits, preoccupations, and conflicts. This test is a projective test and used to identify inner motives and personality dynamics, rather than superficial peculiarities and attitudes.
The results of the patient's Rorschach test indicated that his Perceptual-Thinking Index (PTI) score was high, which meant his cognitive mediation and thought form were distorted, despite his detailed examination of information from the world. When he was confused by his emotions, however, the quality his of information processing decreased. He tried hard to control his emotions and avoid being influenced by them. However, his emotional control was very poor. In situations where he could not use cognitive mediation or clues, his reality testing was extremely poor, indicating a distorted sense of reality. It was most difficult for him to control anger related to damage to his pride. He initially had a strong sense of identity, but his failure to assimilate to his environment during his medical internship resulted in the development of a serious identity conflict, though he was not actually aware of his lack of control over his emotions. Therefore, his emotions were an obstacle to maintaining stability in his behavior. The problem with his personality structure and the stress in his life caused him psychological pain, i.e., his Depressive Index score was high. On the surface, he seemed to be a cooperative person. However, he had strong subconscious defenses toward the outside world.
Exner (2003) recommended examining the content of minus responses in detail. A minus is coded for responses that differ a great deal from the actual stimulus. Therefore, minus responses are considered to be projected contents of the subject's mind or serious distortions of cognition or emotion. The content of his minus responses were (I) a shinto priest; (III) a deer horn; (IV) fog and clouds; (V) the left side of the body of a crab, the head of a dinosaur, and a bow tie with a white shirt; (VI) erupting Mt. Fuji; (VII) a cracking pelvis and men's faces; (VIII) the face of a samurai and armor without a head; (IX) a large satanic skeleton, food in hell, and a living skull; and (X) an aged man, meteorite, and a face. Among this patient's responses, the following met Lerner's criteria (1996) for impairments in the first stage: (III) a deer horn; (IV) fog and clouds; (V) the left side of the body of a crab; (VIII) the face of a samurai and armor without a head; and (IX) a satanic skeleton, food in hell, and a living skull. Lerner (1996) applied the object relations model integrating Piaget's theory of early cognitive development and Mahler's theory of separation-individuation and defined three stages. In the first stage, the main cognitive task is to recognize the object he is holding at the sensorimotor stage. If there is any impairment, it will be connected to the lack of affective relatedness to the environment. In the second stage, the main task is to distinguish an object from other people at the mid-sensorimotor stage. If a caretaker fails to hold a baby, the impairments will result in a baby who depends on the environment too excessively and is influenced by the stimuli. As a result, the baby will lack independence, even when she grows up and becomes an adult. In the third stage, the early preoperational stage, a baby has tasks that establish internalization and representation. If the baby fails to accomplish these tasks, she will have impairment in evocative object constancy and could fail to internalize learning skills. This patient's impairments were categorized as belonging mainly to Lerner's first and second stages. Impairment in the first stage means that he could not use symbolization. There is lack of imagination, poor vocabulary, lower intellectual accomplishment, difficulty in understanding means and aims, low interest in the environment, a poverty of information, and a lack of understanding and conceptualization of the world using human vocabulary. Impairment in the second stage means the patient lacks the ability to distinguish between external and internal objects and cannot complete the representational process.
These results showed that this patient made intense efforts to control his emotions. However, these efforts tended to collapse easily when he was overwhelmed by anger related to damage to his inflated pride. Such collapses left his psychotic anger and anxiety exposed. Consequently, his olfactory reference syndrome was found to be similar to psychotic disorders.
Sentence Completion Test (SCT). This test is composed of 80 sentences. Participants are asked to complete a sentence that has been started by the examiner. The sentence completion test taps into the respondents' cognitive resources and reveals their predetermined attitudes, feelings, and emotions, all of which help the therapist gain insight into the patient's behavior.
Although the patient's Japanese grammar was good, he did not complete many of the sentences. Furthermore, the content of his responses was poor. He completed sentences for which he could write his preferences and specific contents of his life, such as “Attraction for me … was baseball,” “When I was a child, I … got up at seven o'clock every morning,” “My siblings … were three, an older sister and a younger brother,” and “I dislike … computers.” However, he did not continue to write sentences starting with “I” (e.g., “I regret …” “I secretly…” “I cannot forget…”) and “My” (e.g., “My feeling …” “My anxiety …” and “My brain …”). The sentences that revealed his symptoms were “Do you wear … my clothing?” “Talk to me seeing … my face,” and “I do not think about … my job.” His relationships with others seemed to be mostly positive for him. He wrote “Friends … were important,” “At school … I was a kind of funny,” and “I recall … having a happy high school life.” However, for one sentence, he wrote that “It was frequently said … that I was strange.” Based on the results of this test, we can understand his daily life, preference, and family structure, but not his fantasies, worries, anxieties, and his inner life. His responses only referred to extremely superficial things. He could not describe his inner life or his defensiveness with other people.
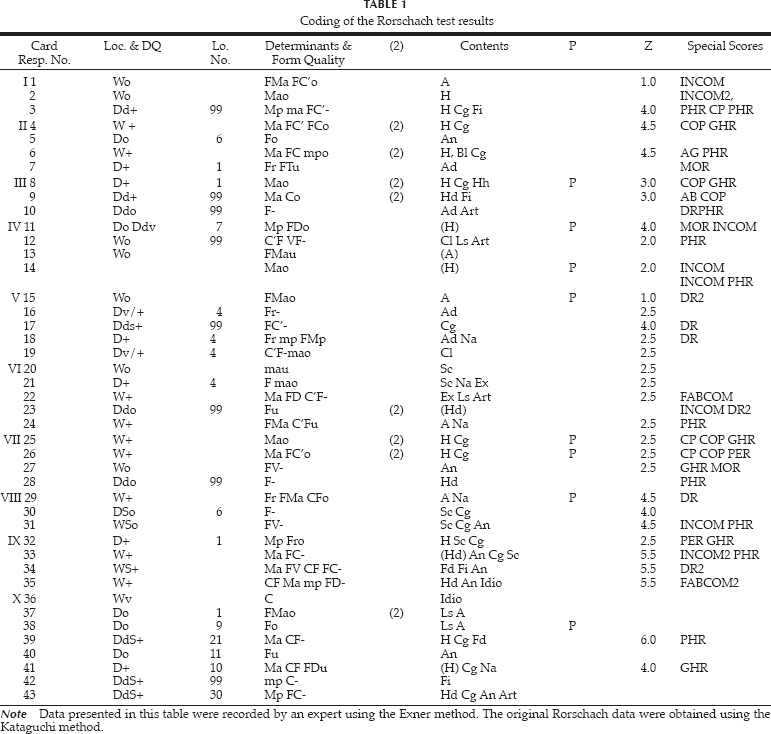
Coding of the Rorschach test results
House-Tree-Person Test (HTP) and Integrated House-Tree-Person Test (IHTP). This test was created by Buck in 1948. A subject is asked to make separate drawings of a house, a tree, and a person. Once these tasks are completed, the subject is asked to draw a house, a tree, and a person as a landscape. These drawings provide a measure of self-perceptions, attitudes, and composition ability. The picture of the house is considered to represent a person's feelings toward his or her family. The picture of the tree is considered to represent feelings of strength or weakness. The picture of the person is considered to provide information regarding the person's self-concept.
Relations, percentages, and derivations of the Rorschach results

This patient drew a tree with eight fruits and one falling leaf. The roots were drawn below a line that symbolized the ground. Normally, the roots under the ground are not seen. The tree crown was drawn roundly, and he added five semicircles under the crown of the tree. As a result, the tree crown hangs down. This drawing suggested that he was stimulated by emotion rather than reason. He hopes to childishly depend on others and might have experienced being denied emotionally. He seemed to become aware of his tendency to be stimulated by emotion, his emotional displays, and infantility in spite of his ideal self-image. The house was drawn in three dimensions. There was a chimney from which smoke was rising, two windows for which it was unclear whether they were open or shut, and one closed door. A line symbolizing the ground was also included. The roof was triangular. Lines representing the wall and chimney that should have been hidden by the roof were still visible.
The woman smiled, with an open square mouth and closed eyes with eye lashes and ears, but no eyebrows, nose, or border between the hair and neck. She wore a long sleeve shirt and mini skirt without any decorations. Her foot projected out from her skirt without shoes. Her fingers were sharp. Her shoulder-length hair was drawn using a single line. The drawing of the woman without a neck indicates that the woman in his image could not control her emotion or impulse through reason. The man's face was a circle, with large black eyes, eyebrow, ears, a smiling mouth drawn with one line, bristle up black hair, a neck, stern shoulders, and sharp fingers. He wore a long sleeve shirt, a pair of trousers, and a belt. The man's large eyes symbolized his suspicious mind toward the outside would.
For the Integrated HTP, he drew three houses, five trees with fruit, a person walking a dog, a person washing his car, a road, and a car. On this drawing, a line representing a road was drawn behind a person and trees. The results of these tests indicate that he tended to ignore reality and was not concerned about this. He was careless and vague in differentiating between internal and external stimuli.
Discussion
Three kinds of psychological tests indicated that the patient had a weak ego structure. Normally, an infant psychologically and physically develops from simple or naïve to complex or intricate mechanisms. Lerner's theory is arranged according to psychological and cognitive developmental stages. First, an infant recognizes her mother. Next, she can distinguish her mother from other people, such as her father. An infant memorizes her mother after she distinguishes the mother. Although the present patient could not accomplish Lerner's first or second stages, we could not find impairments in the third stage. However, this did not indicate that he had accomplished the tasks of the third stage. His accomplishment was superficial. He had two quite different psychological layers: an adaptive surface layer and a psychotic deep layer. Psychologically normal people also have two layers, but they are able to control the psychotic one as they develop. However, this patient did not develop this ability during the process of growth because his adaptive and social layer was superficial and he could not access his subconscious through his adaptive layer. Therefore, his psychotic layer was easily exposed.
Tustin (1990) reported that patients with this kind of psychological structure show symptoms of obsessive compulsive disorder, manic-depressive disorder, and phobia. Baba (1983/1987) reported the detailed results and a theoretical discussion of the Rorschach tests and psychotherapy process of a patient suffering from delusion and hallucination. The patient suddenly cried and clung to her parents saying, “I am being killed, help.” The patient complained that a creature similar to a wolfman grabbed her shoulders one month before she came to the hospital. Although she had delusions and hallucinations, she could attend school and exercise. The results of her Rorschach test included normal signs and those indicating pathology. Her clinical state and the results of her psychological tests were quite different from those of patients suffering from schizophrenia. Baba (1983/1987) stated that there was a break between the normal and pathological psychological layers.
There may be patients for whom a single category is not suitable. Patients suffering from obsessive-compulsive disorder, manic-depressive disorder, phobia, and even hallucinations and delusions might represent heterogeneous categories.
Inness-Smith (1987) stated that there were some patients who were difficult for clinicians to categorize and treat. His patient suffered from anxiety and was afraid of a recurrence of a coronary attack. The patient was not psychotic and did not suffer from olfactory reference syndrome; however, the patient stated that he smelled his feet and showed his anxiety during the session. He always had relationships with two women, but he did not enjoy the relationships. Sometimes, he showed irrational outbursts. This patient had a mother suffering from schizophrenia. Inness-Smith speculated that certain of the mother's psychotic confusions were transmitted to his patient in very early infancy. He also stated that these patients had many similarities and their symptoms tended to be attributable to their early infancy.
Tustin also reported that patients with this kind of psychological structure often tend to have had traumatic experiences in early infancy (Tustin, 1990). Baarkman, Kortmann, and van den Brik (2009) reported the relationship between psychotic symptoms and traumatic experiences. Although it could not be determined whether or not the present patient had traumatic experiences, many studies have reported that patients with traumatic experiences tend to forget memories related to the trauma (Terr, 1988). In particular, when traumatic experiences happen before the age of two, the individual cannot verbally recall the memories. Such memories appear through behaviors (Terr, 1988). Researchers and clinicians must consider this in future studies.
Patients with problems similar to the present patient tend to be difficult to diagnose. Consequently, appropriate treatment might not be possible. Clinicians and researchers should be careful when treating patients suffering from olfactory reference syndrome.