
Abstract
The purposes were to assess the bivariate and multivariate relationships among the subdomains of physical self-concept, self-esteem, and objective measures of physical fitness in young healthy female graduate students. Nineteen participants were recruited from a local university and completed the Physical Self-Description Questionnaire-Short Form (PSDQ-S) to assess each individual's perceptions of her global physical self-concept, self-esteem, and physical fitness. Subsequently, a maximal aerobic capacity and muscular strength tests were completed, and moderate and significant correlations were found between these measures and the corresponding subdomains of the PSDQ-S. Multivariate analyses revealed that age and height but not the physical fitness tests were significant predictors of physical self-concept, while none of the variables predicted self-esteem.
Physical fitness is defined as “a set of outcomes or traits that relate to the ability to perform physical activity (Welk, 2002). Musculoskeletal strength, flexibility, aerobic capacity, body composition, balance, and agility are the main components of physical fitness. Since physical fitness is an outcome of regular physical activity participation, understanding of the factors that promote physical activity participation are paramount. Psychological factors such as physical self-concept and self-esteem have demonstrated relationships with physical activity (Lemoyne, Valois, & Guay, 2015). Physical self-concept is defined as individual perceptions of competency regarding one's physical abilities and appearance within the various environments that he or she must function in (Buckworth & Dishman, 2002). This construct relates to perceptions of an individual's ability to execute tasks that require one or more of the components of physical fitness.
The literature suggests a bi-directional relationship between psychological moderators such as physical self-concept on physical activity participation, meaning that as physical self-concept increases, so does physical activity participation and vice-versa (Bouchard, 2000). Physical self-concept comprises several subdomains that include muscular strength, endurance, body-fat, and general health (Marsh, Martin, & Jackson, 2010). Enhanced physical self-concept have been shown to relate to increased exercise adoption and adherence for Hispanic adolescents (d = 0.30) (Velez, Golem, & Arent, 2010), obese adult males (d = 0.91) (Short, DiCarlo, Steffee, & Pavlou, 1984), sedentary middle-aged women (d = 0.55) (Annesi & Westcott, 2005). Physical self-concept tends to decrease with increasing age (r = 0.23) (Cumming, Standage, Loney, Gammon, Neville, Sherar, et al., 2011) and BMI (d = 1.16) (Agarwal, Bhalla, Kaur, & Babbar, 2013) and is lower in girls and women as compared to their male counterparts (d = 1.17) (Caglar, 2009). From the period of late childhood to early adolescence, girls tend to have lower physical self-concept than boys (Hayes, Crocker, & Kowalski, 1999; Asci, 2002). No established relationship has been reported between physical self-concept and physical fitness for young women. Physical self-concept and physical activity has been shown to be lower in girls than boys and this pattern of reduced physical self-concept and physical activity persists into young adulthood, as many women tend to pursue higher education, enter the workforce, and or have increased family obligations.
Physical self-concept is part of a multidimensional hierarchical model of self which positions this construct as a psychological domain at the same level as emotional, social, and academic self-concepts. Overall self-concept, described as how an individual organizes these various perceptions, is positioned at the apex of this model (Buckworth & Dishman, 2002). Overall self-concept is necessary for an individual to determine how they feel about these self-perceptions, and determines overall self-esteem: self-concept relates to perceptions of self, whereas self-esteem refers to the feelings one has based on individual evaluations of these perceptions (Sonstroem & Morgan, 1989). Various types of physical activities have been shown to have moderating relationships on self-esteem. A systematic review conducted by Spence, McGannon, and Poon (2005) reviewed 113 studies to examine the weighted effect sizes of various moderators of exercise and self-esteem. They found small effect sizes for aerobic (d = 0.25) and resistance training (d = 0.26) exercise participation on self-esteem. They found small to medium effect sizes for measures of aerobic capacity (d = 0.32), body composition (d = 0.38), and muscular strength (d = 0.37) on self-esteem.
Since physical fitness is an outcome of physical activity participation and physical self-concept is related to physical activity participation, the question remains as to the relationships between objective measures of physical fitness and physical self-concept. Young women were participants in this study because they tend to have lower physical self-concept than men and report lower physical activity than men when demographic and socioeconomic factors such as race, age, and income are controlled (Centers for Disease Control and Prevention (CDC): Division of Nutrition, Physical Activity, and Obesity, National Center for Chronic Disease Prevention and Health Promotion, December 1, 2011; Centers for Disease Control and Prevention, 2013). Monroe, Thomas, Lagally, and Cox (2010) examined these relationships in college-aged students and found moderate to strong relationships between measures of physical fitness and self-perceptions of competency. An understanding of the relationships among physical self-concept, self-esteem, and physical fitness measures that utilize maximal aerobic and strength tests for this population are the purposes for this study.
Hypothesis 1. Significant, positive linear relationships will exist between objective measures of muscular strength, aerobic capacity, and BMI with the corresponding self-perceptions of these measures.
Hypothesis 2. Significant, positive linear relationships will exist between objective measures of muscular strength, aerobic capacity, BMI, resting blood pressure, and self-perceived health status.
Hypothesis 3. Significant, positive linear relationships will exist between objective measures of muscular strength, aerobic capacity, and self-perceptions of being physically active.
Hypothesis 4. Significant, positive linear relationships will exist between objective measures of muscular strength, aerobic capacity, resting blood pressure, and anthropometry with global physical self-concept and self-esteem.
Method
Participants
Twenty students enrolled in a graduate physical therapy program were recruited from a local university in Houston, Texas as a sample of convenience; nineteen complete data sets were analyzed. The inclusion criteria were: between 18–30 yr. of age, with no report of current participation in organized recreational activities or sports teams. The exclusion criterion was any self-report of a current medical condition as cited on the Physical Activity Readiness Questionnaire (Thomas, Reading, & Shephard, 1992). Informed consent was received from each participant as approved by the Texas Woman's University Institutional Review Board. The PSDQ-S and physical fitness tests were completed in one day. Each participant performed the objective health and physical fitness tests in the sequence described in the sections below. The PSDQ–S was completed prior to commencement of the physical fitness measures.
Measures
Self-reported physical activity.—The International Physical Activity Questionnaire (IPAQ) was completed by each participant for descriptive purposes to characterize the self-reported volume of physical activity performed over the previous 7 days. The IPAQ is widely used in large scale research studies to assess physical activity levels (Fogelholm, Malmberg, Suni, Santtila, Kyrolainen, Mantysaari, et al., 2006; Bauman, Ainsworth, Sallis, Hagstromer, Craig, Bull, et al., 2011; Lee, Macfarlane, Lam, & Stewart, 2011). Previous studies have documented the IPAQ's test-rest reliability (r = 0.3–0.8) and concurrent/criterion validity (r = 0.55 – 0.71) to be moderate (Tehard, Saris, Astrup, Martinez, Taylor, Barbe, et al., 2005; Fogelholm, et al., 2006; Hagstromer, Oja, & Sjostrom, 2006; Macfarlane, Lee, Ho, Chan, & Chan, 2006; Mader, Martin, Schutz, & Marti, 2006; Forsen, Loland, Vuillemin, Chinapaw, van Poppel, Mokkink, et al., 2010; Lee, et al., 2011). The IPAQ inquires about the various types of physical activities associated with household, transportation, occupational, and recreational pursuits. The intensity, frequency and durations of each type of physical activity can be quantified, summed, and expressed as the number of minutes spent performing activities at a particular intensity, e.g., metabolic equivalents (METs) per week. The physical activities documented are those that are used to enhance overall health through formal exercise programs, occupational tasks, household chores, and modes of transportation that are moderate to vigorously intense. Moderate physical is defined as physical activity with an energy expenditure of 4 METs while vigorous physical activity is defined as physical activity with an energy expenditure of 8 METs, with activity volume expressed as the number minutes spent at each intensity level per week (The IPAQ Group, November, 2005).
Physical self-concept.—The Physical Self-Description Questionnaire–Short Form (PSDQ–S) was used to measure physical self-concept, self-esteem, and self-perceptions for each component of fitness and health. The PSDQ–S was developed by Marsh (Marsh, 1996; Peart, Marsh, & Richard, 2005; Marsh, et al., 2010) to measure the multiple dimensions of physical self-concept. The PSDQ–S comprises nine distinct subdomains and two global measures. Only the Body fat, Endurance, Strength, Activity, Health, and the two global measures of Physical self-concept and Self-esteem were evaluated. The responses that pertained to each domain were averaged (Marsh, 1996). Each question was scored on a Likert scale anchored by 1: False and 6: True. Some of the questions utilize a reverse scoring method for negatively phrased questions to prevent the respondents from answering the questions in a socially desirable manner, and the responses to questions were re-coded appropriately for data analysis. The maximum average score for each sub-domain is 6. The psychometric properties of the PSDQ–S have been reported in the literature, and it has well-established internal consistency (median α = 0.92) and test stability [r = 0.69 (14 mo.); r = 0.83 (3 mo.)] with populations from several different cultures and age groups (Marsh, et al., 2010).
Health measures.—Height and weight were measured with a stadiometer and the Tanita® BF-350 body composition scale (Arlington, IL), respectively, and BMI was calculated. Resting blood pressure and heart rate assessed via an electronic sphygmomanometer. Both the systolic and diastolic blood pressure readings will be utilized for the data analysis. The Physical Activity Readiness Questionnaire (PAR–Q) was completed to determine if the participants were able to safely conduct the objective physical fitness tests without prior consultation from a physician.
Physical fitness tests.—Muscular strength was measured by the isotonic 3 repetition maximum (3-RM) loads lifted using the seated chest press, seated row, and supine leg press (QuantumFitness®; Stafford, TX), which were divided by each participant's body weight and multiplied by 100 to provide a relative measure of strength (3-RM/BW%). Three different sets of muscles were assessed: (1) pectorals, deltoids, and triceps; (2) latissimus dorsi, deltoids, and biceps brachii; and (3) quadriceps, gluteal muscles, and hamstrings. For participants able to perform repetition maximums that exceeded three at the highest allowable weight that could be selected for the machine, their 3-RM was estimated using the Brzycki equation, which has excellent reliability (ICC: 0.95–0.98) and validity (error rate: 3.0–6.3%) with 1-repetition maximum (1-RM) tests (McNair, Colvin, & Reid, 2011; Abdul-Hameed, Rangra, Shareef, & Hussain, 2012). Maximal aerobic capacity was measured as the maximal oxygen consumption (VO2 max), which was assessed using a metabolic cart (ParvoMedics TrueOne® 2400; Sandy, UT) and the Bruce protocol multi-staged maximal treadmill test (Heyward, 2006; American College of Sports Medicine, Thompson, Gordon, & Pescatello, 2010). Blood pressure and heart rate were monitored during the treadmill test via a manual sphygmomanometer and Polar® (Lake Success, NY) heart rate monitor, respectively. Maximal oxygen consumption was reached when the respiratory exchange ratio was greater than 1.0 or if the participant requested to discontinue the test, for any reason. The test-retest reliability (r = 0.98–0.99) of the ParvoMedics TrueOne® 2400 metabolic cart and the Bruce protocol for the assessment of VO2 max have been well established in previous research reports (Crouter, Antczak, Hudak, DellaValle, & Haas, 2006; Macfarlane & Wu, 2013).
Statistical Analysis
Data were analyzed using Statistical Program for the Social Sciences (SPSS) Version 21.0 for Windows (IBM Inc., Chicago, IL). Each variable was checked for normality, linearity, and equality of variances. Means and standard deviations (SD) were calculated for the following variables: each physical fitness measure, and the Body fat, Endurance, Strength, Health, Activity, and global measures of Physical self-concept and Selfesteem from the PSDQ–S. The Pearson Product Moment Correlation (r) was utilized to determine the bivariate relationships between each subdomain of the PSDQ–S and each corresponding physical fitness measure using a one-tailed test with alpha set at 0.05. The bivariate correlations to be examined were, for Hypothesis 1, Body fat, Endurance, and Strength subdomains from the PSDQ–S and BMI, VO2max, and isotonic strength measures. For Hypothesis 2, the comparisons were between the Health subdomain from the PSDQ–S and systolic and diastolic blood pressure and each physical fitness measure. For Hypothesis 3, the comparisons were between the activity subdomain from the PSDQ–S and each physical fitness measure. For Hypothesis 4, comparisons were between the global measure of Physical self-concept and Self-esteem and each measure of physical fitness. A multivariate linear regression model was constructed to predict physical self-concept with the demographic factors of age and height entered into the first block (weight was excluded because it was used to normalize the objective measures of muscular strength and aerobic fitness). In the second block VO2max, chest press, seat row, leg press, diastolic blood pressure, and systolic blood pressure variables were entered as predictors in the model. Finally, another multivariate linear regression model was used to predict self-esteem using the same two blocks of variables to predict physical self-concept.
Results
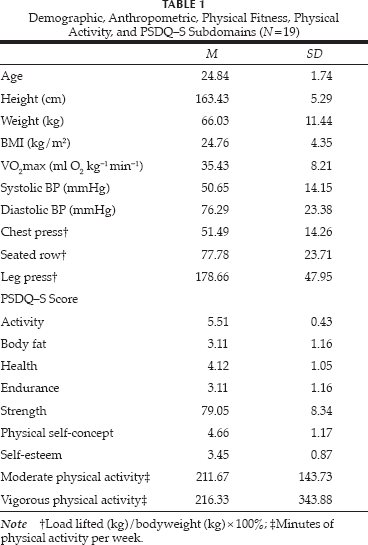
Twenty female students were recruited for this study, and nineteen completed the entire battery of physical fitness tests and the PSDQ–S questionnaire (see descriptive statistics in Table 1). Two of the 19 participants were able to perform repetitions on the isotonic strength tests that exceeded three repetitions at the highest settings on one or more of the machines used, or they were able to perform repetitions that exceeded the machine's capacity; therefore, the Brzycki equation was used for those participants to estimate the 3-RM load. All data met the assumptions of normality and equality of variances.
Demographic, Anthropometric, Physical Fitness, Physical Activity, and PSDQ–S Subdomains (N=19)
All bivariate correlations pertaining to the hypotheses are presented in Table 2. For Hypothesis 1, a strong and significant positive correlation was found between the PSDQ–S Endurance subdomain and maximal aerobic capacity (VO2max); however, the PSDQ–S Strength subdomain had moderate and significant positive corelations with isotonic chest and leg press loads lifted relative to bodyweight percentage. For Hypothesis 2, the PSDQ–S Health subdomain had no significant correlations with any of the objective measures. For Hypothesis 3, the PSDQ–S Activity subdomain demonstrated moderate but significant relationships with two of the three isotonic strength tests, the seated row and the leg press. No other significant relationships were found. For Hypothesis 4, physical self-concept had no significant correlations with any of the objective measures of physical fitness. Self-esteem had moderate and significant correlations with the seated row and leg press loads lifted per bodyweight percentages.
Bivariate Relationships Between Self Perceptions of Physical Fitness, Health, and Global Physical Self-concept and Self-esteem With Objective Measures of Physical Fitness and Health

One-tailed p < .05.
One-tailed p < .01.
The results of the hierarchical multiple linear regression to predict physical self-concept revealed that the overall model was significant (F8,10 = 3.21, p = .04, adj R2 = .495 (Table 3). However, addition of the physical fitness predictors to the model did not significantly improve model fit (ΔR2 = 0.48, F6,10 = 2.84, p = .07). Upon examination of the individual predictors, systolic blood pressure was the only variable that significantly predicted global perceived self-concept scores when controlling for the other variables in the model (β = −0.74, p = .03) (Table 4). These results suggest that as women's systolic blood pressure increases, their global perceived self-concept decreases.
Multiple Linear Regression to Predict Global Physical Self-concept

Note Model 1: Age, Height; Model 2: Model 1 + BMI, VO2 max, Systolic BP, Diastolic BP, Chest Press, Seated Row, Leg Press.
Regression Coefficients From Regression Predicting Global Physical Self-concept

The results of the second hierarchical multiple linear regression to predict global self-esteem revealed that the overall model was not significant (F8,10 = 2.55, p = .08, adj R2 = 0.41) (Table 5). In addition, adding the physical fitness predictors to the model did not significantly improve model fit (ΔR2 = 0.61, F6,10 = 3.11, p = .06). Furthermore, no predictors significantly predicted global self-esteem scores (Table 6).
Multiple Linear Regression to Predict Global Self-esteem

Note Model 1: Age, Height; Model 2: Model 1 + BMI, VO2 max, Systolic BP, Diastolic BP, Chest Press, Seated Row, Leg Press.
Regression Coefficients From Regression Predicting Self-esteem

Discussion
This study examined the relationships among perceptions of physical fitness and health with actual health and fitness measures for healthy young women. For this group, the relationships between perceptions of strength and endurance with the actual measures were strong. All three isotonic measures tested large muscle groups of the upper and lower body using movements that require synergistic activation of these muscle groups. The Strength subdomain of the PSDQ–S may be reflective of physical tasks that require use of large muscles working together to accomplish a task. Other modes of strength testing should be performed such as 1-RM testing and isokinetic testing of these same muscle groups to ascertain if these modes of testing would provide a stronger relationship to the Strength subdomain. The findings showed stronger relationships among measures of muscular strength and the PSDQ–S Strength subdomain than a similar study done by Monroe, et al. (2010), which quantified the relationships between objective physical fitness measures and self-perceptions using the PSDQ with college students. The current study used measures that were more reflective of maximal muscular strength, while Monroe, et al. used a muscular fitness test more indicative of muscular endurance (maximal number of curl-ups completed in 1 min.). The use of submaximal muscular tests vs. tests that examine the maximal contractile properties of muscles may explain the lower correlations and effect sizes found in Monroe, et al. The relationships found between the PSDQ–S Strength subdomain and the objective measures were also stronger than those found Amesberger, Finkenzeller, Wurth, and Muller (2011) who examined self-perceptions of muscular strength with objective measures but in elderly individuals. They found weak to moderate correlations among lower extremity concentric muscle strength, power (jump height), and the PSDQ–S Strength subdomain. The disparity of the relationships between the objective and self-perceived measures may be reflective of the divergent ages between the current sample and Monroe, et al.'s.
The relationship between the PSDQ–S Endurance subdomain and maximal aerobic capacity (VO2max) demonstrated the strongest relationship of all the subdomains of the PSDQ–S and the corresponding objective measure. The study found a stronger relationship between these two measures than the studies conducted by Amesberger, et al. (2011) and Monroe, et al. (2010), in which they evaluated the relationships between aerobic capacity and the PSDQ–S Endurance subdomain. Aerobic capacity was assessed using a maximal treadmill test, whereas the previous two studies assessed aerobic capacity using a submaximal treadmill and maximal bicycle test protocol, respectively. Previous literature has noted potential errors in the estimation of maximal aerobic capacity using submaximal protocols and cycle ergometry, as they have been shown to underestimate maximal aerobic capacity (American College of Sports Medicine, et al., 2010). This study also found moderate relationships among the PSDQ–S Endurance subdomain and two of the isotonic strength measures, the seated row and the leg press. It is unclear what the physiological relationships are among these measures of strength and self-perceptions of endurance, other than the questions used for the PSDQ–S Endurance subdomain which make inquiries regarding self-perceptions of physical activities that require muscular endurance of the lower extremities (e.g., running, skiing) and the upper extremities (e.g., swimming, aerobic classes).
There are few published studies that examine the relationships between self-perceptions of health with objective measures of health and physical fitness for young adult women (Lamb, 1992; Van Vorst, Buckworth, & Mattern, 2002; Schneider, Dunton, & Cooper, 2008; Annesi, 2010; Monroe, et al., 2010; Lemoyne, et al., 2015). Many of the studies that examine the relationships with self-perceptions of health are done with elderly individuals using physical function, quality of life, and mortality as the correlate measures (King, Pruitt, Phillips, Oka, Rodenburg, & Haskell, 2000; Wojcicki, Szabo, White, Mailey, Kramer, & McAuley, 2013). The PSDQ–S Health subdomain demonstrated a moderate relationship with only one physical fitness measure, BMI. The lack of a correlation with any of the other physical fitness measures supports the findings of Schneider, et al. (2008), who found that improvements in objectively measured aerobic fitness did not manifest in changes in any subdomain of the PSDQ–S for sedentary adolescent girls. Other published reports refute these findings; Warr, Scofield, Spiering, & Alvar, 2013 noted that deployed soldiers who were able to perform strength and aerobic training more frequently had higher upper body strength and fat mass reduction as compared to soldiers who trained less frequently. In addition, a higher percentage of soldiers reported enhanced perceptions of optimal health as compared to the soldiers who trained less frequently. When stratified by perceptions of optimal health, the soldiers with enhanced perceptions of health during deployment had larger improvements in aerobic capacity and more weight loss compared to soldiers who reported no changes or reductions in health status. Comparable to the current study, Warr, et al. utilized direct measures of muscular strength and endurance, which may have yielded stronger relationships with perceptions of health. Similar findings were encountered in other published studies that examined the relationships between self-perceived health status and objective measures of aerobic capacity utilizing maximal tests of this fitness component (Gander, Lee, Sui, Hebert, Hooker, & Blair, 2011; Mota, Santos, Silva, Aires, Martins, & Vale, 2012).
No relationship was found between the PSDQ–S Body Fat subdomain and BMI. There are several plausible reasons for this unusual finding. The women in this study reported participation in moderate to vigorous physical activities that were much higher than the national average based on age and sex (Centers for Disease Control and Prevention, 2013). Although the current study did not directly assess lean body mass development, it is not reflected in BMI. Future studies should employ direct measures of body composition such as air displacement plethysmography or bioelectrical impedance. Another possible reason for this finding is the IPAQ, used to assess physical activity, inquired about participation in aerobic activities that tend to reduce fat-mass; the IPAQ does not assess participation in resistance-based activities that promote the development of lean mass. Establishing relationships between perceptions of adiposity and actual adiposity may require more information about participation in these various types of physical activities. Statements such as, “I have too much fat on my body” and “my waist is too large” appear to assess perceptions of excessive adiposity and disproportionate bodily dimensions.
The lack of relationships between the Health subdomain and all of the objective physical fitness and health measures was not expected. The perceptions of being “healthy” were unrelated to physical fitness, and thus it appears from this study that young active women may view themselves as being healthy but not necessarily “fit.” The state of being “healthy” is defined by the World Health Organization (1947) “as the state of complete physical, mental, and social well-being, and not merely the absence of disease or infirmity.” It may be that the type of questions used to assess the PSDQ–S Health domain evaluates the latter and not the former aspects of this definition. It appears that the PSDQ–S Health subdomain taps illness and not wellness. Questions such as “I have to go to the doctor because of illness more than most people my age” are questions that are reflective of being ill, as opposed to not being in a state of optimal health. The effect sizes between perceptions of health and physiological parameters such as blood pressure, BMI, and physical fitness were negligible.
The Activity subdomain demonstrated moderate relationships with two of the isotonic strength measures, the seated row and the leg press. This was an unexpected finding because the types of questions that are used, such as “I often do exercise or activities that make me breathe hard” or “I do physically active things (e.g., jog, dance, bicycle, aerobics, gym, swim) at least three times a week” appear to tap participation in aerobically-based physical activities. Maximal aerobic capacity demonstrated a moderate relationship with this domain but the lack of power limited the significance of this relationship. Lamb (1992) performed a similar study that examined the relationships among various self-reported physical activities and objective measures of physical fitness for young, college-aged adults. He found correlations that ranged from −0.03 to 0.33 between self-reported measures of participation in total, very hard, hard, and moderate levels of physical activity with objective measures of aerobic capacity and body fat; only the correlation between very hard physical activity and aerobic capacity were significant. The questionnaire used in that study (the Liverpool Questionnaire) quantifies the energy expenditures for physical activities performed over the past 14 days to derive four categories of physical activity participation. Maximal aerobic capacity demonstrated a moderate relationship with this domain but the lack of power limited the significance of this relationship. The original intent of the PSDQ–S was to assess the multi-dimensionality of physical self-concept. PSDQ–S subdomains such as Activity were not designed to quantify physical activity participation or energy expenditure as in Lamb's study, but to assess an individual's self-perceived competency in being able to engage in various physical activities that are moderately to vigorously intense several times a week. Similar to the significant correlations found between the Endurance subdomain and the two isotonic strength measures, it is possible that the strength of the muscle groups of the upper back, biceps, forearms, and the muscle groups of the quadriceps, hamstrings, and hips play a significant role in the perceptions of being able to carry out the aerobically-based physical activities described for the Activity subdomain.
Global physical self-concept had no significant relationships with any of the objective physical fitness measures, while global self-esteem had significant relationships with the isotonic measures only. Global physical self-concept had a moderately strong but non-significant relationship with the chest and leg press measures as indicated by the large confidence intervals and small effect sizes found between these two isotonic measures and global physical self-concept. Because of the multi-dimensionality of physical self-concept and the elevated position it occupies on the self-concept hierarchy, measures of fitness such as body composition and aerobic capacity would also have been expected to have significant relationships with this measure. Carraro, Scarpa, and Ventura (2010) published a study that examined the relationships between physical self-concept and objective physical fitness measures for Italian adolescents. They found moderate but significant relationships between the Global Physical Self-Concept from the PSDQ and objective measures of upper body muscle endurance, aerobic capacity and lower extremity power which were components of the EUROFIT physical fitness battery. In contrast, Annesi and Westcott (2005) found no relationships between global physical self-concept assessed via the Tennessee Physical Self-Concept scale and maximal isometric upper extremity force in sedentary older women who completed a 10-wk. resistance-training program. Monroe, et al. (2010) found moderate to weak relationships between global physical self-concept and submaximal aerobic capacity, muscular endurance of the trunk, and BMI. It appears that the relationships between global physical self-concept and muscular strength may be affected by the method of assessment, submaximal vs. maximal, which can be further delineated in studies that compare these modes of assessments with more adequately powered studies.
The current study found age and height combined in the multivariate analysis to predict physical self-concept. It is well established that advanced age is characterized by lower physical self-concept, but similar changes in height self-concept are not as well established. It is plausible to consider individuals who are taller than average are more apt to pursue certain recreational activities in which height is an advantage. When analyzed individually and via multivariate analyses, the physical fitness components did not enhance the prediction of physical concept. Peculiarly, systolic blood pressure predicted physical self-concept in this analysis, whereas it did not when assessed using bivariate correlations. The contradictory relationship between systolic blood pressure and physical self-concept when analyzed via bivariate correlations vs. the use of beta coefficients may be due to the contrasting methods of analysis. The multivariate analysis allowed for the relationship between systolic blood pressure and physical self-concept to be evident while controlling for muscular strength, aerobic capacity, and anthropometric measures, all of which have been shown to influence physical self-concept. Blood pressure is a physiological measure that is reflects the function of the aerobic, renal, endocrine, and neurological systems (Grekin & Gross, 1983; Guyenet, 2006; Wojtusik & Sulowicz, 2012).
Global self-esteem had strong relationships with two of the isotonic strength assessments, seated row and the leg press. The findings of a relationship between isotonic strength measures and self-esteem parallels the findings by Spence, McGannon, and Poon (2005), who conducted a systematic review examining the effects of exercise on self-esteem. They found the largest effect size for participation in strength training (d = 0.26) followed by aerobic training exercise (d = 0.25) as moderators of self-esteem. This systematic review reported the moderating effect of exercise on self-esteem with exercise frequencies greater than 3 times per week (d = 0.36) and participation in high-intensity exercise (d = 0.26). These are similar frequencies and intensities of exercise that were reported by the female participants in the current study. The factors of age, height, physical fitness, and health did not predict self-esteem in a multivariate analysis. Self-esteem is derived from self-concept, i.e., the process of evaluating and the development of feelings about the conscious perceptions of self. It is clear that self-esteem and physical self-concept, a subdomain of overall self-concept, are distinct constructs. Although in this study age, height, and systolic blood pressure predicted some variance in the women's perceptions of physical competency, these factors did not predict the influence that these variables have on how they felt about themselves. Future studies should examine if there is a predictive value among these variables for older, more sedentary, and less educated women.
Limitations and Further Research
A limitation of this study is that the participants were relatively homogeneous with regards to age and sex, with similar blood pressure and fitness levels. This lack of variability limits the ability of this study to establish relationships across a spectrum of blood pressures and fitness levels and probably reduced the correlations among the variables. Both elevated and low blood pressures have tenuous relationships with symptoms of well-being because often these alterations are subclinical in nature. It may not be until symptoms are present that relationships between blood pressure and perceptions of health can be established. Future studies may need to assess potential relationships between the Health subdomain and other global physiological measures such as fasting glucose for individuals of all ages or gait speed as a measure of function particularly for elderly individuals.
The limitations of this study are related to the generalizability to women of different ages, ethnicities, educational attainment, and physical activity engagement. The participants were highly active as described by the self-reported participation in moderate and vigorous physical activities each week; however, the average aerobic fitness displayed by the participants and the small sample size, with outliers who reported extremely high physical activity participation, may leave some doubt whether these participants were as physically active as they reported. Balogun, 1987 assessed the physical fitness of 50 female undergraduate physical therapy students and found their anthropometric, aerobic, muscular strength, and flexibility levels were comparable but not superior to those of other female college students. The International Physical Activity Questionnaire was used for descriptive purposes only, since the terms “moderate” and “vigorous,” although operationally defined in this instrument, can be ambiguously interpreted along with problems associated with the recall of the various types of physical activities performed in the previous seven days. Although the issues regarding the reliability of the self-reported physical activity levels are numerous, it can be assumed that the sample had much higher levels of physical activity participation and a higher percentage of individuals who exceeded the Federal Physical Activity guidelines. Further studies should utilize more objective measures of physical activity such as accelerometry to stratify individuals based on physical activity levels or to establish relationships between these levels and subdomains of physical self-concepts.
Another limitation relates to the level and type of education the women were pursuing. All of the women in this study had bachelor's degrees or higher degrees and they were pursuing a doctoral degree in a health-related profession that utilizes exercise as a principal treatment modality. These participants perhaps were more inclined to be physically active and thus fostered an inclination to pursue a degree in a movement-related health profession such as physical therapy. Miller and Berry (2000) noted that graduate physical therapy students possessed superior knowledge of health-related physical fitness than nurses and athletic training students upon entry into their respective academic programs. It is plausible that this knowledge was a factor that translated to the physical activity behaviors reported by the participants. McWhorter, Wallmann, and Tandy (2002) noted that three successive classes of female graduate students studying physical therapy were able to maintain their aerobic capacity and increase their lower extremity strength over a two-year follow-up period despite the academic rigors of their program. It can be surmised that the increased knowledge possessed by physical therapy students may have allowed them to maintain their fitness despite challenges such as lack of time or energy created by an intense academic program.
The U.S. health care system has traditionally utilized physical therapists in a secondary prevention role to ameliorate the adverse effects of disease and injury on function and quality of life for individuals (Sullivan, Wallace, O'Neil, Musolino, Mandich, Studer, et al., 2011). Presently, there are provisions created in the Affordable Care Act which have placed physical therapists in the forefront of primary prevention efforts. Physical activity promotion is the prime modality used by physical therapists for these primary preventive efforts (Sullivan, et al., 2011). Physical therapists should be able to articulate and display the outcomes of regular physical activity participation in order to promote these ideals with the patients they serve. Future studies should compare the psychological moderators and mediators of physical activity among people in other occupations where lower physical activity participation is typical.
Conclusion
Few studies have examined the relationships between perceptions of physical fitness and actual physical measures in young adult women. The implications of these findings may allow for future studies that extend to young men and women from other regions of the United States, other age groups, and diverse educational and physical activity levels which were limitations of this study due to the homogeneity of this group. Expanding this research to the aforementioned groups will further the understanding of the relationships between the components of physical self-concept with the corresponding objective measures of physical fitness. Physical fitness components such as aerobic capacity, body composition, and muscular strength have been shown to correlate with certain disease indicators such as morbidity, mortality, incidence, and prevalence rates. If the components of physical fitness that have strong relationships with these disease indicators could be assessed using a questionnaire, then large-scale epidemiological studies to further ascertain these relationships could be performed in a more cost- and time-efficient manner. The mediating and moderating roles that physical self-concept has on physical activity participation has been demonstrated in previous literature; however, the roles between physical self-concept and physical fitness are not as clear (Cumming, et al., 2011). Physical activity participation and physical fitness are divergent constructs and thus may explain why the relationships between physical self-concept and objective measures of physical fitness require a more careful evaluation with larger sample sizes.