
Abstract
Six intellectually disabled youth (age range, 12–21 years) underwent training to improve motor skills, endurance, muscle strength, and motor balance. Progress was measured every four months for five years. Fifteen types of training machines were developed and used. Outcomes were measured using various methods, including observation of participants' movements, fitness testing, questionnaires, and video monitoring. Participants' guardians were required to be present during each training session, and details such as workload and number of repetitions were recorded for each exercise. Significant effects of training tended to appear after roughly one year and gradually increased. Physical training for these intellectually disabled individuals not only improved mental and physical health, but also yielded effects on social skills such as the capacity for self-control over their own behaviors, as well as acceptance of instructions from others and the ability to interact cooperatively.
Mental retardation has historically been defined as an intelligence quotient (IQ) under 70. According to the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) published by the American Psychiatric Association (2007), three criteria must be met for a diagnosis of intellectual disability: IQ < 70; significant limitations in two or more areas of adaptive behavior as measured by an adaptive behavior rating scale, i.e., delays in oral language development, deficits in memory skills, difficulty learning social rules, difficulty with problem-solving skills, and delays in the development of adaptive skills such as self-care skills; and lack of social inhibitors. The following ranges also reflect the categories of intellectual disability: profound (IQ < 20); severe (IQ 20–34); moderate (IQ 35–49); mild (IQ 50–69); and borderline intellectual functioning (IQ 70–84).
In school or classes for children with intellectual disability, walking, running, ball games, swimming, skiing and other activities are carried out in the physical education curriculum (for instance: Ministry of Education, Sport, Science and Culture in Japan, 1999). In general, the ability to play sport and exercise is lower among children with intellectual disability than among ordinary children (Kihara & Hashimoto, 2000), with deficiencies in coordination and balance of movement rather than muscular strength compared with ordinary children (Sloan, 1951; Ravin, 1957; Howe, 1959; Hatano, 1973).
Experience with exercise is often lacking in these children. Health problems accompanying obesity are more prominent in children with intellectual disability than in children without such disabilities (Balakrishnan & Wolf, 1976; Chaney, Eyman, & Miller 1985; Eyman, 1988). Promoting exercise without interest and willingness to engage in physical exercise itself is a difficulty for children with intellectual disability classified as profound, severe, or moderate. The intention in this study was to introduce a new method of training that contained some amusing body movements and actions exercising the core muscles of the body (e.g., psoas major, iliac, and erector spinae muscles) with special training machines that were developed by the second author.
The training method was originally developed for elderly individuals with low fitness or dementia who have a few opportunities for physical exercise. This training was found to be readily accepted by the elderly, was effective for improving walking and movement abilities in daily living, and had positive effects on lifestyle (Shizuoka Prefecture General Health Center, 2006).
The present study attempted to adapt the new method of training for use by young individuals with intellectual disability and examined whether this machine training would be acceptable for long-term training over several years. Continuation of training was also expected to improve coordination during exercise and to be associated with progress in behaviors of daily life related to the adaptive behaviors rating scale.
Method
Participants comprised four boys (M1–4) and two girls (F1,F2) who commenced training at between 12 and 15 years old and continued for 5 years. Although a total of 11 intellectually disabled individuals have undertaken the training, performing 90-min. training sessions once a week at the same time each week, the present study only reports results for the 6 participants who continued for an extended period, because the others started training 1–3 years after the initial 6 participants. Both male and female participants used the same training machines. The ages of the participants during the study were as follows: M1, 14–19 years; M2, 13–17 years; M3, 14–18 years; M4, 16–19 years; F1, 15–20 years; and F2, 15–21 years. Intellectual disabilities were as follows: profound disability (IQ ≤ 20), one participant (M4); severe disability (IQ, 20–34), four participants (M1–3, F2); and mild disability (IQ, 50–69), one participant (F1). Two of the participants (M2 and F2) had Down syndrome.
At the commencement of training, all participants exhibited pronounced autistic tendencies, difficulty expressing themselves in greeting, and relatively severe impairment in going about activities of daily life, such as inability to walk safely down the street without a guardian holding their hand. Training was provided to these intellectually disabled youths at the request of their guardians. Consent to the participation of children was obtained after the guardians had received an adequate explanation that the training would be carried out in their presence and that the results of the associated research would be published.
The guardians were introduced to this training program by a volunteer who provides support to intellectually disabled children. The guardians were eager to educate their children, accompanied their child on every training day, and provided encouragement during exercise.
The training began in May 2006, and results were compiled for the subsequent 5-year period up to April 2011.
Training Machines
The training machines used in the present study can be classified based on the training movements involved, as follows.
Group 1. Six kinds of machines were used for muscle strength and stretching motions, namely: lumbar extension; leg extension/flexion; hip abduction (opening legs); hip adduction (closing legs); shoulder stretching; and trunk twisting with motions of the ipsilateral arm/leg.
Group 2. Two kinds of rowing machines were used: one power-assisted rehabilitation rowing machine (sitting position); and one rowing machine without power assistance (standing).
Group 3. Two kinds of stationary bicycles were used: one power-assisted rehabilitation ergometer cycle with an elliptical pedal orbit for cycling exercises (Photo 1); and one bicycle ergometer for maximum effort sprint-style cycling.
Group 4. One sprint training machine with rotating pedals, backward-moving axis and applied force (Photo 2) and one power bike machine with an elliptical orbit (induced by moving wheel axis) were used for whole-body dynamic motor balance, basic motor training for walking and running, and inner muscle training (Photo 3).
Group 5. A one-leg swing machine was used for synchronized hip motions and a trunk rotation machine was used for trunk training (trunk rotation, leg and hip swinging).
Group 6. One kind of treadmill was used for improving walking and running motion and building endurance.
All machines except for the treadmill (Group 6: Otake-Root, Iwate, Japan) and bicycle ergometer for maximum effort (Group 2: Power Max-V; Combi, Tokyo, Japan) were originally developed with the concept of improving motor skill of walking and running using core body muscles and improving flexibility and range of motion mostly by the various motions for stretching muscles.
Training participants performed Group 1 and 2 exercises for 30 min., Group 3, 4 and 5 exercises for 25 min., and Group 6 exercises for 5 min., comprising a total of 15 exercises. Training time was 90 min., including rest and preparation for the next exercise. At first, participants could only manage Group 1 and 2 exercises in the allotted 90 min., but after 1 year they could complete all exercises and also exhibited improvements in quality of movements.
Measurement of Body Characteristics and Physical Fitness
Height, body weight (BW), and body fat percentage (%BF) (Body Composition Analyzer; Tanita, Tokyo, Japan) were measured in addition to the sit-and-reach test, 10-m obstacle walk, grip strength, 50-m run, and back muscle strength using the “New Physical Fitness Test” of the Ministry of Education, Culture, Sports, Science and Technology (MEXT). Measurements were performed every 4 mo. for the duration of the 5-year study period.
Guardians were requested to complete a questionnaire on changes in the daily activities of participants.
Many adaptive behavior scales have been developed, and accurate assessment of the quality of adaptive behaviors also requires clinical judgment. In the present study, questionnaire items were selected from the behavior scales shown in the guide of Diagnostic of Statistical Manual of Mental Disorder: (1) daily living skills, such as getting dressed, using the bathroom, and feeding oneself; (2) communication skills, such as understanding what is said and being able to answer; and (3) social skills with peers, family members, adults and others.
Questionnaire items comprised items such as health condition, mind of challenging to trying new tasks, willingness to exercise, daily living skills, social skills with peers, relationship with family members, and frequency of smiling. Guardians checked items using a 5-grade evaluation scale, after receiving explanations on how to fill in the questionnaire sheet.
Observation of Participant Movements
In the present study, physical movements that could not be numerically quantified, relating to facets such as skill development, behavior expression, and motivational level, were observed and recorded by the first author.
Results
Results of measurements taken over the 5-year study period were as follows.
Body Height
The height of female participants F1 (135 cm) and F2 (137 cm) did not increase from 12 years of age onwards. These heights were low compared to the average of 158 cm for 18-year-old Japanese females. Among the male participants, height remained unchanged for M1 at 160 cm, M2 grew 11 cm from 163 cm to 174 cm, M3 grew 13 cm from 166 cm to 179 cm, and M4 grew 2 cm from 175 cm to 177 cm.
Body Weight and Percent Body Fat
Among female participants, F1's weight ranged between 51 kg and 47 kg and percent body fat (%BF) fluctuated from 38% to 35%, while F2's weight increased from 43 to 52 kg and %BF increased from 32% to 40%. Among the male participants, M1, whose height had remained unchanged, showed a weight range of 48–50 kg. M2, whose height had increased, decreased in weight from 83 kg to 76 kg, and %BF decreased from 48% to 39% after 1 year and to 30% after 2 years, with a dramatic overall decrease to 23% by the 5-year mark. M3, who grew the most in height (+13 cm), gained weight from 62 kg to 78 kg and %BF changed slightly within the range of 23% and 18%. M4's weight fluctuated between 55 kg and 57 kg, while %BF fluctuated within the range from 10% to 7%. Marked differences in physical development were seen for each participant.
Muscle Strength (Grip and Back Muscle Strength)
Grip strength and back muscle strength were measured as indicators of muscle strength. As shown in Fig. 1, during the period of a young person's development, muscle strength typically increases in association with height. In terms of mean values during development, for a typical Japanese male student, grip strength is about 32 kg at a height of 160 cm, and around 42 kg at 170 cm grip strength. Measurements of muscle strength in each participant over the course of the study period are shown in relation to height in Fig. 2. Specifically, ranges of height and grip strength were 158–160 cm and 14–20 kg for M1, 162–174 cm and 8–32 kg for M2, 166–179 cm and 12–25 kg for M3, and 175–177 cm and 12–20 kg for M4. These measurements were equivalent to 47–78% of those of a standard student. Among female subjects, F1 and F2 showed grip strengths in the ranges 15–25 kg and 12–22 kg, respectively. The height of these girls was equivalent to that of the average Japanese 10-year-old girl, and grip strength relative to height was consistent with the national average.

Relationship between height and grip strength of Japanese male students in elementary, junior high, and high school. Prepared based on data from MEXT's Physical Strength and Motor Fitness Survey.
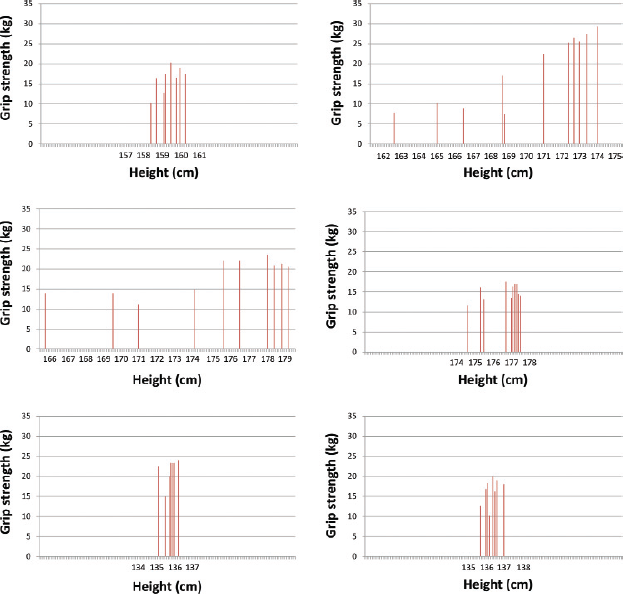
Relationship of height and grip strength over the experimental training for male (M1-M4) and female (F1-F2) participants.
In terms of other physical fitness parameters, M1 displayed improved flexibility in the seated forward stretch (flexibility test), but no other participants exhibited any marked changes in this area. Regarding the relationship between height and back muscle strength for the boys, the average Japanese male student has a mean back muscle strength of 100 kg at a height of 160 cm and 120 kg at 170 cm (Fig. 3). For participants in the present study, height and back muscle strength were in the ranges 158–160 cm and 25–50 kg for M1, 162–174 cm and 25–70 kg for M2, 166–179 cm and 42–68 kg for M3, and 175–177 cm and 25–56 kg for M4, respectively. Accordingly, back muscle strength for study participants was <58% of that of a typical student. Female participant F1 had back muscle strength of 28–60 kg and F2 had 28–59 kg, equivalent to the average for a typical 10- to 12-year-old student (Fig. 4).

Relationship between height and back muscle strength of Japanese male students in elementary, junior high, and high school. Prepared based on data from MEXT's Physical Strength and Motor Fitness Survey.
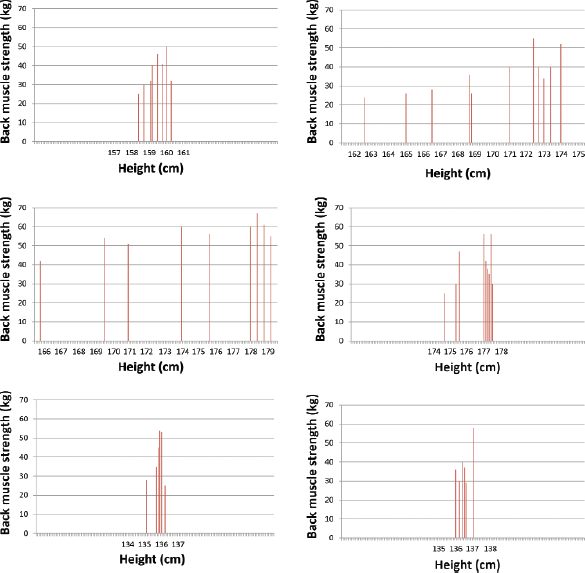
Relationship of height and back muscle strength over the experimental training for male (M1-M4) and female (F1-F2) participants.
50-m Run (Fig. 5)

Changes in 50-m run performance over the experimental training for male (M1-M4) and female (F1-F2) participants.
M1 initially recorded a time of close to 16 sec., but subsequently improved to 10–13 sec. M2 took more than 40 sec. at 12 years old, as running was his most challenging exercise, but managed to gradually reduce this, reaching about 15 sec. by the time he progressed to high school (at 15 years old). M3 gradually reduced his time from 15 sec. to around 9 sec. from 16 years old through to 18 years old, while M4 posted wildly inconsistent times from 9 sec. to 19 sec., but later in the range of 12–13 sec. F1 achieved relatively consistent times of 12–13 sec., whereas F2 originally took 15–17 sec., but her running ability declined significantly after graduating from high school.
10-m Obstacle Walk (Fig. 6)

Changes in 10-m obstacle walk performance over the experimental training for male (M1-M4) and female (F1-F2) participants.
Originally developed to help prevent elderly individuals from tripping, this test measures the time taken to walk a 10-m course over which are arranged 5 boxes to be stepped over, each with a height of 20 cm. Overall improvements were seen in recorded times, but the greatest change was observed in the first year, after which either roughly the same times or only slight improvements were seen. However, both M4 and F1 have made continual improvements.
Results from Questionnaire
Excerpted results of the questionnaire are shown in Fig. 7. Although some individual differences were observed among respondents, tendencies toward improvement were observed in endurance time for running (running distance), making the bed, health, appearance of health condition, making the usual greetings, and letter discrimination.
General Observations
Participants showed satisfaction with training, positive facial expressions, and improved sense of stability during exercise (see supplemental videos). A state of unease was observed at the start of training, but training machines were soon being used with a sense of curiosity and happiness. In addition, improvement of movement was observed in all members with repeated training. Regular attendance without absence for months became the norm for participants, and sessions seemed to become an important part of the weekly schedule.
Discussion
We have previously reported on the effects of training intellectually disabled youths with the aim of improving their motion abilities (Hayakawa and Kobayashi, 2008; 2011). The present study, on the other hand, is characterized by the recording of continuous results from long-term training of intellectually disabled youths using various types of original training machines developed by Dr. Kobayashi. The Totsubo Gym Project in Kashiwa City, Chiba Prefecture, Japan is a training program being conducted under the guidance of the University of Tokyo that uses these Cognitive Motor Development Training Machines to provide training to more than 1,500 local participants, mostly within the age range of 60–90 years.
The word “Cognitive” was used in the name of this series of new training machines, because cognitive abilities relating to control of body movements are a key requirement for performing machine exercises adequately, especially for machines in Group 4 such as the sprint training machine and power bike machine with an elliptical orbit.
In this training, the ipsilateral foot, knee, hip and shoulder are required to move in the same direction in a forward movement, to achieve effective use of the core muscles of the torso. Nerve control differing from typical motor behaviors is used in ipsilateral movement of the lower and upper extremities of the body. Movement with different nerve control is initially difficult for most individuals, but becomes easier with focused attention.
The data used to compare muscle strength measurements of study participants with typical students were taken from the “Physical Strength and Motor Fitness Survey” published annually by MEXT. The physical fitness testing by MEXT was reorganized in 2000 as the “New Physical Fitness Test”, in which the measurement of back muscle strength is no longer included. Accordingly, the present study relied on figures published in 1998 for data from which the relationship between height and back muscle strength could be ascertained, and these figures more or less corresponded to the period during which the study participants developed (MEXT, 1998).
While the problems inherent in measuring and evaluating physical ability intellectually disabled individuals have already been highlighted in previous research (Kihara, 2000), the muscle strength measurements of participants taken in the present study with a grip dynamometer and back muscle strength meter tended to be very low. These findings suggest that intellectually disabled individuals have limited capacity for muscle exertion when required to focus strength according to a prescribed method. The muscle strength of developing youths generally tends to gradually increase roughly in proportion to height. This tendency was strongly evident in study participant M2, who was measured from 13 to 17 years old, while M3 and F1 came to exhibit significant increases in muscle strength with gains in height from 1 year after beginning training. Overall, muscle strength relative to height was low compared to the typical student, but participants displayed a propensity towards increased muscle strength as training progressed.
Young intellectually disabled individuals seem to show a higher frequency of disliking physical activities compared with ordinary children. The correlation between development of physical fitness and age is not always as clear as that in ordinary children. In the present study, decreased physical performance as measured by physical fitness tests was observed in some years, but an overall trend toward improvement was found for the total observation period. The time of peak physical fitness (handgrip strength and back strength) for boys and girls with Down syndrome reportedly appears earlier during the course of development than in ordinary children (Hashimoto, 2008). In the present study, improvements in physical fitness were observed after 18 years old. Physical fitness may thus be able to be improved with training even after 18 years old for intellectually disabled individuals.
The training machines used in the present study were originally developed to exercise elderly individuals with low physical strength, but the exercise workload also appears suitable for intellectually disabled youths. Intellectually disabled individuals typically have difficulty with imitation compared with healthy persons (Williams, 2004), but the control systems of these training machines were found to have positive effects in conveying imitation skills to disabled youths.
Furthermore, even in the absence of prominent changes in physical fitness measurements, notable instances of emotional and social change were observed in the daily lives of participants. The results of the guardian questionnaire and observation records also revealed cases where the desire of participants to attend training ultimately led to improvements in speech and behavior, such as in greetings, when communicating before, during, and after training, as well as clear improvements in day-to-day behaviors such as better manners and increased vitality in daily activities. Kalmanson (1992) highlighted the importance of interpersonal relationships in the learning process and this training can also be assumed to have brought about substantive and profound effects in this area.
Safety issues in exercise implementation and the willingness of disabled individuals to actively participate in exercise can be a great motivator for continuation of an exercise program. With the training in the present study, participants could accept the level of safety and maintain interest, and thus were able to continue with the exercise program for a prolonged period.
In healthy individuals, motivation to exercise typically arises from the anticipated benefits. In intellectually disabled persons, however, maintaining adherence to an exercise regimen based solely on the motivation of recognized health benefits can be difficult. Rather, sensory enjoyment and emotional satisfaction from the training itself appears more important as an exercise incentive. The training machines used in this study were designed to avoid muscle soreness, by using solely electronic means to control the exercise load rather than iron weights. Their purpose is to approach physical exercise in a comprehensive manner, and improve quality of movement in daily activities such as the real-life actions of walking and running. The benefits of these training exercises are substantial in elderly individuals who have extended the distance they can walk in 6 min and reduced the time needed to complete the 10-m obstacle walk. In intellectually disabled individuals, this same trend can also be seen in the results of the 50-m run and reduced 10-m obstacle walk times.
Many intellectually disabled youths also have innate physical disabilities (Kohen-Raz, 1992) and suffer from impaired health caused by physical inactivity, often involving obesity, which in turn stems from a lack of opportunities to exercise as well as a lack of proactive efforts by schools and society at large to provide suitable opportunities.
A recent study found that many intellectually disabled youths also suffer from osteoporosis (a state of low bone density) (Srikanth, 2011). A range of social support initiatives are thus required in addition to physical exercise to improve the lives of people with intellectual disabilities (Robinson, 2012). In this context, the development of community support is becoming increasingly important (Kakiya, 2005). Given the need for training programs that encourage participation in community sports suited to the requirements of intellectually disabled youths (Morita & Nanakida, 2004), there is a growing demand for effective scientifically based training. MEXT has stipulated the goals of improved physical fitness and skill through “various sports” (MEXT, 1999), and this is similarly reflected by educational curriculum guidelines in Japan.
Oberman, et al. (2005) highlighted the importance of the relationship between brain function and movement. As pointed out by Reed and Sanderson (1983), physical actions must be broken down into appropriate stages in order for them to be smoothly achievable. Psychosomatic status is closely linked to the operation of the nervous system (Scheere, 1992; Rosenthal-Malek and Mitchell, 1997) and provision of appropriate sensory stimuli has also been suggested as necessary to maintain a healthier psychosomatic state (Dunn, 1997). In this sense, the fact that the training program using the training machines presented in this study was conducted in stages appears to have been highly beneficial. Although the training program contained a range of different exercises, this variety was presumably effective in improving the various physical motor skills.
Motor learning in intellectually disabled youths reportedly leads to a faster transfer of motor skills between exercises and tasks (Matsuoka, 2010). In social activities, familiarization with various movements corresponding to an intended action is essential to increased social adaptability. The continuation of training via the present training system gradually produced physical, emotional, and social benefits at the individual level and is considered to have helped to improve the quality of life among participants.
The present study included only a relatively small number of participants and inter-individual variability in both characteristics and results was substantial. However, the results seem to suggest that improvement of physical activities and motor control is possible with adequate training, even among individuals with profound intellectual disability. Participants were willing and able to continue physical training over the long term (5 years). Physical training also appeared helpful for improving physical health and mental condition, as in ordinary children. The present findings suggest that physical training may be desirable for individuals with intellectual disability, even at the profound level.