
Abstract
Among the most common of major complications of hysterectomy are urinary tract injuries, with reported frequencies of bladder injury and ureteral injury of 2.8 and 1.8%, respectively. Failure to identify these urinary tract injuries at the time of hysterectomy may delay treatment, increasing the risks of morbidity, the need for additional surgeries and the loss of renal function. Seventy-five percent of such injuries are unsuspected intra-operatively during the hysterectomy [1]. Cystoscopy at the conclusion of hysterectomy may detect if there is a ureteral or bladder injury. There is currently controversy whether universal (always) or selective (increased risk of injury) cystoscopy should be performed at the conclusion of hysterectomies.
ACOG has not opined upon whether cystoscopy should be performed at the time of hysterectomy on a universal or selective basis. Additionally, the different types of hysterectomy, and whether adnexa are concurrently also removed, may have differing risks of urinary tract injury. There is recent conflicting published literature that advocates both for universal and for selective cystoscopy at the time of hysterectomy [1,2].
The argument for universal cystoscopy is that the procedure is quick, easy to perform and carries little risk. If an injury is detected, there will be an opportunity to repair it immediately, potentially decreasing future complications.
Those favoring selective cystoscopy believe that it adds expense and time to the surgical procedure with a low yield. Additionally, many bladder and ureter injuries may not be immediately detectable. A common reason that cystoscopy is not performed at the time of hysterectomy has been shown to be the lack of cystoscopy training by the attending OB/GYN [3]. Recently trained OB/GYNs, however, should all have the experience and skill to perform basic cystoscopy to look for bladder or ureteral injuries. The Accreditation Council for Graduate Medical Education (ACGME) currently requires the performance of ten cystoscopies during OB/GYN residency.
Our study was designed to survey current upper level (PGY-3 and PGY-4) OB/GYN residents in ACGME accredited training programs regarding their residency experiences with the performance of cystoscopy at hysterectomy. The study was limited to third and fourth year residents because first and second year OB/GYN residents have limited experience in performing hysterectomies at many training programs. Additionally, whether these OB/GYN residents planned post-graduation to perform universal or selective cystoscopy during hysterectomy was assessed.
Study design
The study was approved by the Einstein Medical Center Philadelphia Institutional Review Board (IRB). A survey was created on Survey Monkey [4], a third party website that allows for users to create and send surveys anonymously and at no cost. Cystoscopy at hysterectomy survey questions are listed in Table 1.
Cystoscopy at hysterectomy survey questions.
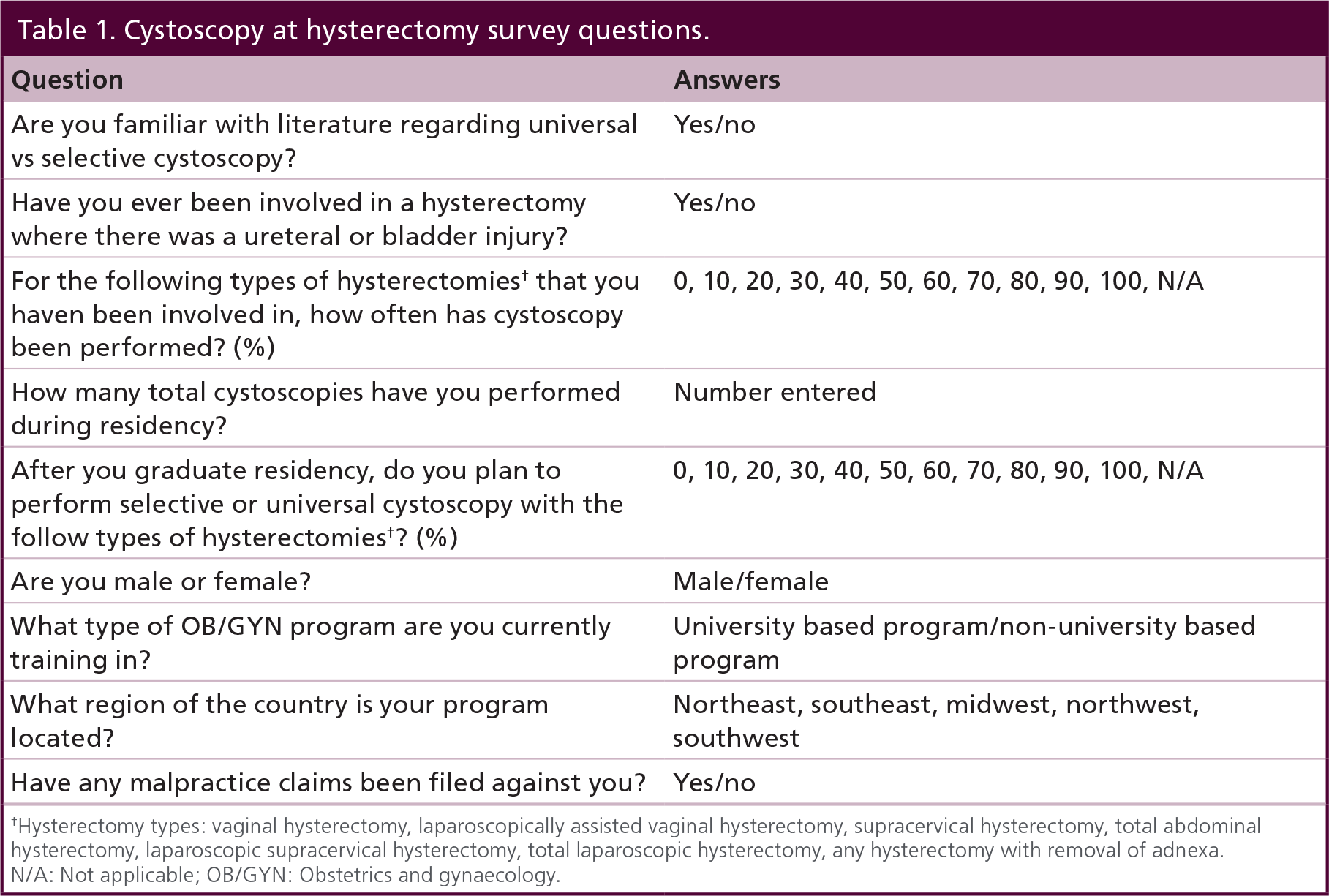
Hysterectomy types: vaginal hysterectomy, laparoscopically assisted vaginal hysterectomy, supracervical hysterectomy, total abdominal hysterectomy, laparoscopic supracervical hysterectomy, total laparoscopic hysterectomy, any hysterectomy with removal of adnexa.
N/A: Not applicable; OB/GYN: Obstetrics and gynaecology.
Demographics and regions of practice were queried. The residents’ experience with cystoscopy and their knowledge of the literature regarding selective versus universal cystoscopy were questioned. Whether the OB/GYN resident had ever participated in a hysterectomy complicated by a ureteral or bladder injury and if they had been sued in a malpractice allegation were also asked.
For each specific type of hysterectomy that they participated, the resident had to answer in what percent of cases cystoscopy had been performed. The categories of hysterectomy were vaginal hysterectomy (VH), laparoscopically assisted vaginal hysterectomy (LAVH), supracervical hysterectomy (SCH), total abdominal hysterectomy (TAH), laparoscopic supracervical hysterectomy (LaSH), total laparoscopic hysterectomy (TLH) and hysterectomy with removal of adnexa. Residents additionally were asked whether as attending OB/GYNs they anticipated if they would choose to perform cystoscopy universally or selectively for each category of hysterectomy.
A link to the nine-question [4] survey was sent via email to OB/GYN residency program coordinators from a list of program coordinators throughout the USA. The residency program coordinators were then asked to forward the survey to current third and fourth year OB/GYN residents. A reminder email was then sent two weeks later to the OB/GYN residency program coordinators.
Investigators accessed the survey responses through the [4] website. The website has the capability to tally responses, as well as create graphs and figures.
Due to residents operating with multiple OB/GYN attending physicians, we defined what would categorically be considered universal and selective cystoscopy at the time of hysterectomy. For categories in which individual resident's reported >90% usage of cystoscopy at the time of hysterectomy were considered representative of ‘Universal’ usage of cystoscopy during hysterectomy. Responses of ≤ 90% performance of cystoscopy were considered ‘Selective’ usage of cystoscopy.
Statistical analysis was performed. Frequency of universal cystoscopy during residency training compared with that planned post residency for individual categories of hysterectomy were compared. Whether gender, residency type, geographical region, frequency of universal cystoscopy during training and number of cystoscopies performed influenced future plans to perform universal cystoscopy for a given type of hysterectomy after residency were also analyzed. Continuous variables were compared using t-test. Categorical variables were compared using Chi-squared analysis. Statistical significance was determined by a p-value of less than 0.05.
Results
Fifty-six current third and fourth year OB/GYN residents completed the entire on-line survey. A total of 59% reported having familiarity with the literature regarding selective versus universal cystoscopy. Seventy-nine percent had been involved with a hysterectomy complicated by either a bladder or ureteral injury. The average number of cystoscopies performed per resident survey responders was 44.
The frequency of residents who reported that cystoscopy was performed in > 90% of the following types of hysterectomy during their training were: vaginal hysterectomy (VH) 12%; laparoscopically assisted vaginal hysterectomy (LAVH) 14%; supracervical hysterectomy (SCH) 0%; total abdominal hysterectomy (TAH) 2%; laparoscopically assisted supracervical hysterectomy (LASH) 7%; total laparoscopic hysterectomy (TLH) 27%; and any hysterectomy including removal of adnexa 5%. For all seven categories of hysterectomy, OB/GYN residents were more likely to plan to perform universal cystoscopy post residency than had occurred during their training

Frequency of universal cystoscopy during residency training compared with planned post-residency for individual categories of hysterectomy.
Upon graduation the categories of hysterectomy which residents planned to most commonly perform universal cystoscopy were TLH (49%) followed by LAVH (34%) and VH (34%). Universal cystoscopy was least likely to have occurred during the residents’ training with SCH (0%) followed by TAH (2%), hysterectomy with removal of adnexa (5%) and LASH (9%). Similarly, upon graduation the categories of hysterectomy which residents were least likely to plan to perform universal cystoscopy were SCH (12%) followed by hysterectomy with removal of adnexa (15%), and TAH (15%).
The likelihood that an individual respondent planned to perform universal cystoscopy for the different types of hysterectomy was analyzed as a function of whether that respondent stated that they were familiar with the published literature on cystoscopy at the time of hysterectomy, whether the respondent was in training at a university affiliated or nonuniversity affiliated residency program, the gender of the resident, and whether the respondent had witnessed a urinary tract injury at the time of hysterectomy.
Respondents who stated that they were familiar with the published literature on cystoscopy at the time of hysterectomy were statistically more likely than were respondents unfamiliar with it to plan universal cystoscopy for several types of hysterectomy. The categories that did not have a statistically significant difference were likely limited by group size
Percent of residents planning to perform universal cystoscopy with hysterectomy postresidency based upon familiarity with published literature.

LASH: Laparoscopically assisted supracervical hysterectomy; LAVH: Laparoscopically assisted vaginal hysterectomy; NS: Not significant
SCH: Supracervical hysterectomy; TAH: Total abdominal hysterectomy; TLH: Total laparoscopic hysterectomy; VH: Vaginal hysterectomy.
There was no difference in planned frequency of performing universal cystoscopy between respondents trained at university-affiliated or nonuniversity-affiliated programs, between female and male residents or in different regions of the USA. Residents who had experienced a urinary tract injury at time of hysterectomy were no more likely to plan universal cystoscopy than were residents who had not. Interestingly, residents who had observed a urinary tract injury were statistically less likely to plan universal cystoscopy after vaginal hysterectomy than were their peers.
An important predictor of whether an individual respondent planned to perform universal cystoscopy for a given type of hysterectomy after residency was whether that same respondent had seen cystoscopy performed universally during residency. Residents who saw cystoscopy performed universally for a specific type of hysterectomy were statistically more likely to plan universal cystoscopy post residency for the same type of hysterectomy.
There was a direct correspondence between frequency of cystoscopy observed as a resident and frequency of cystoscopy planned as an attending, for all types of hysterectomy. For the different types of hysterectomy, the proportion of residents who planned to practice in accordance with their residency experience ranged between 68 and 89%.
Discussion
Injury to the urinary tract is one of the most commonly occurring major complications of hysterectomy. Given reported frequencies of bladder injury (2.8%) and ureteral injury (1.8%) [1], such complications will be encountered by the majority of operating gynecologists at some time or multiple times during their career. In our study, 79% of third and fourth year OB/GYN residents reported already having participated in a hysterectomy complicated by either a bladder or ureteral injury.
The goal of cystoscopy at the time of hysterectomy is the diagnosis of urinary tract injuries during the initial surgery. If such not otherwise identified injuries are found at the time of the hysterectomy via cystoscopy and appropriately addressed immediately, this may potentially decrease morbidity. Cystoscopy at the conclusion of hysterectomy, however, will not detect all bladder or ureter injuries. A ureter may be only partially iatrogenically obstructed or lacerated. Thermal or devascularizing injuries to the bladder or ureter may have a normal cystoscopic findings at the time of hysterectomy. Due to the mechanisms of these injuries, perforation or fibrosis of the injured area of the bladder or ureter may be delayed for several days or weeks.
There is no current consensus regarding whether cystoscopy should be performed universally or selectively at the time of hysterectomy. Advocates of the differing philosophies cite conflicting literature that they believe supports their opinions. Conflicting literature and its interpretation is a barrier to standardized practice in this area.
The Ibaneau article advocated for universal cystoscopy, reporting rates of bladder injury (2.8%) and ureteral injury (1.8%) at hysterectomy, with 75% of injuries unsuspected [1]. In the Sandberg article, however, the rate of ureteral injury was less than 1% (9.6 per 1,000) overall at the time of hysterectomy. This article supported selective cystoscopy based upon the low rate of injury, increased costs and lack of sensitivity for detecting urinary tract injury [2]. Gilmore reported that less than 50% of ureteral injuries and less than 25% of bladder injuries were detected when a cystoscopy was not performed. When cystoscopy was performed, 100% of ureteral injuries and 80% of bladder injuries were detected during a laparoscopic hysterectomy [5]. Another cost analysis study by Visco has shown that universal cystoscopy would be cost-effective only if urinary tract injury rates exceed 1.5–2% [6].
Our study did not factor in the surgical indications for the hysterectomies performed. The frequency of pelvic organ prolapse and the occurrence of concurrent reconstructive surgery was not evaluated. Cystoscopy is often recommended to be performed universally with urologic procedures performed by many gynecologists. Cystoscopy is currently recommended after sling procedures to treat urinary incontinence by the American Urological Association [7]. Additionally, the Urinary Incontinence Treatment Network recommended that cystoscopy be performed at the time of any surgery for stress urinary incontinence [8].
Barriers to performing cystoscopy at hysterectomy may include the lack of training in cystoscopy by the attending OB/GYN and a lack of hospital privileges to perform it. A 2005 survey, reported that the lack of cystoscopy privileges in 14% of cases was the reason for not performing cystoscopy. In the same survey, the most common reason for not performing a cystoscopy was lack of training [3]. OB/GYNs may be reluctant to consult a urologist to perform a cystoscopy, especially if no injury is suspected. Given the current requirement for cystoscopy performance during OB/GYN residency, all graduating OB/GYNs should have the surgical skills for basic cystoscopy. The residents who responded to our survey averaged having each already performed 44 cystoscopies. Given their training, hospital cystoscopy privileges will likely be granted to an increasing number of OB/GYNs.
Rather than combining all hysterectomies together as a single procedure, we individually assessed the performance of cystoscopy for seven different categories. Each procedure may have different risks of bladder and ureteral injury. Patient positioning during vaginal and laparoscopic procedures facilitates cystoscopy. Additionally, other factors such as surgical skill, adhesive disease, uterine size and concurrent procedures at the time of hysterectomy, such as an anterior repair, may increase the risk of a urinary tract injury.
The category of hysterectomy with removal of adnexa had one of the lowest rates of cystoscopy being performed or planned on being performed after residency. As queried in the survey, this category encompasses all types of hysterectomy. Patients undergoing removal of the adnexa at the time of hysterectomy are more likely to have conditions such as endometriosis, adhesive disease, pelvic inflammatory disease, adnexal neoplasm and pelvic malignancy. Additionally, operating lateral to the adnexa at the time of hysterectomy places the surgical area closer to the ureter, increasing the risk of injury. Given the increased risk of ureteral injury with concurrent adnexal removal, it is both interesting and counter-intuitive that cystoscopy rates were lower for these hysterectomies.
It is disappointing that 41% of current third and fourth year OB/GYN residents were unfamiliar with the published literature regarding selective versus universal cystoscopy at the time of hysterectomy. Hysterectomy is one of the most common procedures performed by OB/GYNs, with urinary tract injury one of the most common of major complications [9–15]. The lack of standardized guidelines regarding the performance of cystoscopy with hysterectomy may contribute to this knowledge deficit.
The key determinants of whether an individual respondent planned to perform universal cystoscopy for a particular type of hysterectomy after residency were whether the respondent was familiar with published literature on cystoscopy at the time of hysterectomy, and whether the resident had been trained using universal cystoscopy for specific types of hysterectomy during residency. There are examples in the literature on how exposure in surgical training influences practice post residency, which are consistent with our findings. In the obstetrical field, it has been reported that OB/GYN residents who performed greater than the threshold of 13 forceps deliveries during their training were more likely to use them in independent clinical practice [16]. Similarly, general surgeons were more likely to perform a procedure based upon their case volume during residency training. Additionally, physician comfort with a surgical procedure was also associated with the number of cases performed during their residency training [17].
Limitations of our survey study include the sample size of resident responses to our survey despite requesting distribution of the survey twice. It is impossible to know exactly how many of the emailed OB/GYN residency program coordinators actually forwarded the survey request to their upper level OB/GYN residents. Thus, it is impossible to calculate a survey response rate or the geographical distribution of the respondents. There may have been a confounding bias in which respondents were either more for or against universal or selective cystoscopy. To improve and better track response rates, a future study technique might send a survey request directly to all OB/GYN residents rather than through residency program coordinators. Additionally, survey studies usually report respondents’ best estimates rather than exact numbers. As we only studied the performance of cystoscopy during hysterectomies with OB/GYN resident involvement, it is unknown if hysterectomies with no resident participation would differ.
In summary, no standard of care has been definitively established whether at the time of hysterectomy universal or selective cystoscopy should be practiced to assess for iatrogenic urinary tract injury. In our study, cystoscopy at the time of hysterectomy was performed universally in the minority of the surveyed OB/GYN residents’ current training for all categories of hysterectomy. In each of the seven surveyed hysterectomy categories, residents reported that they planned post-graduation to utilize universal cystoscopy at the time of hysterectomy more often than had occurred in their training. In no category of hysterectomy, however, did greater than 50% of residents plan to perform universal cystoscopy post residency. Knowledge of the published literature on cystoscopy at the time of hysterectomy and increased frequency of its usage during residency were predictive of increased plans to utilize universal cystoscopy during hysterectomy post training. As OB/GYNs have greater exposure to cystoscopy during their residency training, it is likely that the frequency of cystoscopy at the time of hysterectomy will increase.
Conclusion
Our study was designed to evaluate clinical practice regarding the performance of universal (always) or selective (increased risk of injury) cystoscopy to evaluate for urinary tract injury at the conclusion of hysterectomies. Urinary tract injuries are among the most common major complications of hysterectomy, with the majority unsuspected. Cystoscopy is performed in the minority of all hysterectomy types. Post residency, residents plan to perform cystoscopy at hysterectomy more frequently compared with during their training.
Executive summary
Among the most common of major complications of hysterectomy are urinary tract injuries to the bladder and ureters.
The majority of urinary tract injuries are unsuspected at the time of hysterectomy.
Cystoscopy at the time of hysterectomy may possibly detect some urinary tract injuries, allowing immediate repair.
There is currently controversy whether universal (always) or selective (increased risk of injury) cystoscopy to evaluate for urinary tract injury should be performed at the conclusion of hysterectomies.
OB/GYN resident physicians were asked to complete an internet based survey assessing demographic information, as well as their experience with and opinions toward cystoscopy at the time of hysterectomy.
Statistical analysis was performed on physician demographic information, familiarity with the literature and experience with and opinions toward cystoscopy at the time of hysterectomy.
Universal cystoscopy was performed for the following types of hysterectomy: vaginal hysterectomy 12%; laparoscopically assisted vaginal hysterectomy 14%; supracervical hysterectomy 0%; total abdominal hysterectomy 2%; laparoscopically assisted supracervical hysterectomy 7%; total laparoscopic hysterectomy 27%; and any hysterectomy including removal of adnexa 5%.
Residents paln post graduation to utilize universal cystoscopy at the time of hysterectomy more often than had occurred in their training for all types of hysterectomy.
For all categories of hysterectomy, OB/GYN residents were more likely to plan to perform universal cystoscopy post residency than had occurred during their training.
Cystoscopy at the time of hysterectomy was performed universally in the minority for all categories of hysterectomy.
Knowledge of the published literature on cystoscopy at the time of hysterectomy and increased frequency of its usage during residency were predictive of increased plans to utilize universal cystoscopy during hysterectomy post-training.
Future perspective
Over the next 5–10 years, it is likely that the performance of cystoscopy at the time of hysterectomy will increase from its current performance. Physicians will become more familiar with and skilled in performing cystoscopy as OB/GYN residency programs now require training in it. This is consistent with our findings that post-training, residents plan to perform cystoscopy more often for all categories of hysterectomy.
Acknowledgements
The study was presented orally at the ACOG District III Junior Fellow Meeting in Delaware on 3 October 2014. The study was also presented in poster form at the combined ACOG Districts I, III, and IV Meeting in Baltimore on 11 October 2014. The study has also been presented in poster form at the ACOG Annual Clinical Meeting in San Francisco in May 2015.
Footnotes
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.