
Abstract
Endometriosis is a disease that affects millions of women worldwide and its diagnosis is still challenging. Medical history, symptoms together with imaging data may address the correct diagnosis, but the gold standard remains laparoscopic assessment with histological confirmation. The development of serum markers as diagnostic tools for endometriosis may allow a prompt and noninvasive diagnosis. Several serum biomarkers have been investigated over the years, but none of these have shown a clinical utility and nowadays the more realistic diagnostic biomarker consists in a panel of biomarkers. The recent introduction of new technologies such as genomics and proteomics may represent the future perspective of endometriosis diagnosis.
Keywords
Endometriosis is a disease that affects millions of women worldwide, predominantly in reproductive age [1]. Endometriosis is often disabling, leading a chronic condition that profoundly destabilizes the quality of life of the patient with a negative impact on social/personal life and with high healthcare costs.
The diagnosis of endometriosis can be suspected in women with pelvic pain and/or subfertility, although endometriosis may be completely asymptomatic. The combination of medical history, symptoms, pelvic examination and ultrasonographic findings may be useful for a presumptive diagnosis. The growing impact of ultrasonographic data shows that although the ultrasonographic diagnosis of endometrioma is relatively certain, with 88% accuracy and 90% specificity [2], deep infiltrating endometriosis remains a heterogeneous disease and its diagnosis remains a major challenge. Currently, the ultrasonographic diagnosis of deep infiltrating endometriosis is persistently improving and shows a comparable accuracy and specificity of MRI [3]. Nevertheless, the gold standard for the diagnosis of endometriosis is still the laparoscopic assessment, ideally confirmed by histological examination [4].
On these basis, although the several improvement in scientific and diagnostic knowledge on endometriosis, its diagnosis still remains tricky with a delayed time for a correct diagnosis, with an average time around 6.7 years [5]. It is considered that the development of noninvasive diagnostic test for endometriosis would have a pronounced impact on the patients' quality of life, anticipating endometriosis diagnosis and avoiding unnecessary treatment as well as endometriosis progression and complications from repeated surgery. During the last few years the scientific literature widely investigated the possible use of specific markers for the early diagnosis of endometriosis, but while peritoneal markers are too much variable under hormonal influence and related to the peritoneal fluid amount, the investigation of serum markers revealed many interesting molecules. The ideal properties of a serum biomarker are represented by its specificity and sensitivity, but also by its ability to relate to the disease activity allowing disease follow-up.
Investigated serum markers
Pathogenesis of endometriosis may be considered as a multifactorial process that involves predominantly hormonal alterations, in terms of estrogen dependence and progesterone resistance. Moreover, several and recent studies demonstrated a fundamental role of the inflammatory response with evasion of the immune clearance, of modification in endometrial cell proliferation, attachment and invasion ability and of the angiogenetic process. Considering all these possible pathogenetic steps, numerous reports tried to recruit a reliable serum marker that may be used in the daily clinical practice (Table 1).
Tumor antigens: CA-125 & other glycoproteins
Commonly used for the evaluation and diagnosis of malignant disease, glycoproteins have largely been evaluated as potential diagnostic tools for endometriosis diagnosis.
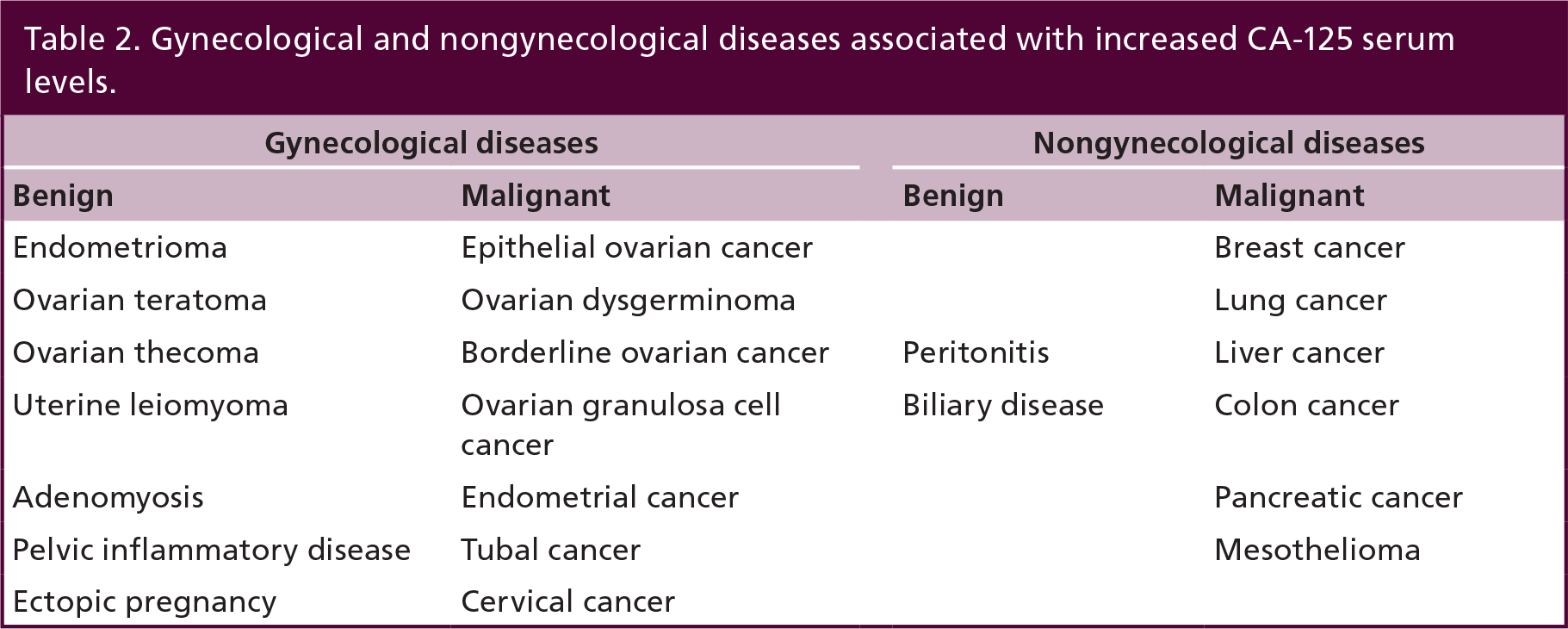
The most consistently studied glycoprotein in endometriosis has been CA-125, which, from its characterization in 1981, has been associated to several benign and malignant pathologies. CA-125 could be identified in patients with cancers of the lung, breast, endometrium and gastrointestinal tract, but elevated levels have been demonstrated also in benign diseases of the liver and gastrointestinal tract, inflammation and benign tumors of the ovary and uterus (Table 2). Actually, CA-125 evaluation represents the most reliable markers for detection of epithelial ovarian cancer, showing a significant value as marker of prognosis, disease progression and response to chemotherapy. Its accuracy has been widely studied also for endometriosis since it is produced by endometrial and mesothelial cells and may be secreted into circulation in response to inflammation. A complete meta-analysis found that serum CA-125 performance in the detection of any type of endometriosis was low, but was better for the detection of severe endometriosis [6]. Subsequent studies confirmed these previous results [7,8], but at the same time CA-125 levels have been found to be much higher in serum of women with endometrioma [9] or dense pelvic adhesions [10] compared with other forms of endometriosis.
Finally, the diagnostic accuracy of CA-125 for endometriosis is low, considering the most commonly employed cut-off values in the literature (35-0 IU/ml). Furthermore, normal physiological conditions may also modulate CA-125 serum levels causing variations in concentrations, as during late secretive phase and menstrual phases of menstrual cycle [11].
Nevertheless, nowadays CA-125 remains the only serum marker widely used in clinical practice in terms of endometriosis diagnosis. To date, CA-125 may be proposed more a prognostic marker rather than a diagnostic marker, since postoperative CA-125 values have been demonstrated to be significantly lower in women who achieved a pregnancy and apparently had a complete disease removal [12]. CA-125 levels may also be useful in patients' follow-up after surgical or medical treatment or to evaluated disease recurrences [13].
Considering other glycoproteins, CA-19.9 was initially detected in patients affected by colorectal carcinoma, but the evidence that endometriotic tissue also expresses CA-19.9 opens several researches on its evaluation as serum markers for endometriosis diagnosis. However, the results are still contradictory, since some studies failed to find any association with endometriosis and CA-19.9 serum levels [7], while others study reported raised levels of CA-19.9 in patients with endometriosis and an association with severe stages [14]. Moreover, comparing CA-19.9 and CA-125 accuracy Harada et al. [14] found that CA-19.9 had similar specificity but reduced sensitivity compared with CA-125. In a more recent study, CA-125 and CA-19.9 serum levels reached similar sensitivities and specificities (86–89% and 61–52%, respectively) [15].
Investigated serum markers.

AFP: Alpha-fetoprotein; CEA: Carcinoembryonic antigen; NLR: Neutrophils/lymphocytes ratio; sFasL: Soluble Fas ligand.
Gynecological and nongynecological diseases associated with increased CA-125 serum levels.
Finally, other glycoproteins have been tested during the years looking for a significant association with the endometriotic disease, such as CA-15.3, CA-72, alpha-fetoprotein, carcinoembryonic antigen and β-2 microglobulin. Recently, new progresses are directed to the analysis of serum haptoglobin that has been identified as a secretory product of endometriotic lesions. Serum levels of haptoglobin-E chain isoforms levels have been demonstrated to be significantly higher in women with endometriosis than in controls [16].
Growth factors & peptides: activin, follistatin & urocortin
Activin A is a member of the TGF-β superfamily and it is produced by the healthy endometrium, but also by eutopic and ectopic endometrium in endometriosis [17]. In physiologic conditions, activin A promotes the process of decidualization of endometrium in preparation for embryo implantation, allowing uterine receptivity [18]. An aberrant expression of activin A has been observed in the endometrium of women with endometriosis and, as consequence, Reis et al. [19] showed only a modest increase in serum activin A in women with ovarian endometrioma between women with deep infiltrating endometriosis and women with the other forms of endometriosis.
Follistatin is a glycoprotein involved in the inhibition of activin A. Its production occurs in a coordinated way with activin A and it is the major regulator of activin bioactivity. Follistatin is abundantly expressed in human endometrium and endometriotic tissue at all phases of menstrual cycle [20] and by antagonizing activin A, it has been shown to inhibit stromal cell decidualization. Recently, Florio et al. [21] showed a significant increases in serum follistatin levels in women with endometriosis and endometriomas compared with controls. The possible role of follistatin in the pathogenesis of endometriosis is still unclear, but some crucial events implicated in the development of the disease, such as endometrial differentiation, mesothelial invasion, immune system modulation and angiogenesis, are modulated by the activin/follistatin system. Serum follistatin was increased in women with ovarian endometrioma compared with controls, other benign ovarian cysts or nonovarian endometriosis. Follistatin showed a sensitivity of 92% corresponding to 92% specificity at 1433 pg/ml cut-off. Comparing follistatin and CA-125 accuracy, CA-125 detected only 44% of endometriomas with 90% specificity, showing that follistatin may be considered a potential marker of endometrioma, with much higher sensitivity than the current marker CA-125. Recently, the same group demonstrated that serum follistatin concentrations are different in women with endometriosis with higher follistatin levels in peritoneal and ovarian endometriosis compared with deep infiltrating endometriosis [19].
Urocortin is a neuropeptide belonging to the corticotrophin-releasing hormone family, known to be expressed in the endometrium [22]. On this basis, serum urocortin has been investigated as possible markers for endometriosis. Serum levels of urocortin were found to be significantly higher in women with endometriomas than in women with other benign ovarian cysts, giving a sensitivity of 88% and specificity of 90%, while CA-125 detected only 65% of the cases with the same specificity [23].
Glycodelin A is an endometrium-derived protein with known angiogenic and immunosuppressive effects which could contribute to the development of endometriosis and endometriosis-related infertility. Glycodelin A has been demonstrated to be elevated in the sera and in peritoneal fluid of women affected by endometriosis, with a sensitivity and specificity as a biomarker for ovarian endometriosis of 82.1% and 78.4% in serum, respectively [24]. Moreover, the combined analysis of IL-6, TNF-α and glycodelin A serum concentrations provided a good method of discrimination between the subjects with endometriosis and the controls [25].
Immunological markers: cell populations & cytokines
The role of immune system in the pathogenetic process of endometriosis is a growing evidence. Consequently, various populations of immune cells and their secretions, in term of antibodies and cytokines, have been studied to test their utility as biomarkers.
The possible role of T lymphocytes as well as B-cell populations have been investigated, although some differences have been shown in eutopic endometrium and peritoneal fluid, no significant differences have been shown in the proportion of serum T and B cells in women with and without endometriosis [26,27].
However, the analysis of the autoantibodies has produced quite a lot of remarkable outcomes. Autoantibodies pattern in women with endometriosis revealed significantly increased serum concentrations of B-cell levels in women who were positive for antinuclear antibodies (ANA) [28]. Moreover, great attention has been focused on the role of serum antiendometrial antibodies as possible cause of infertility in endometriosis; the sensitivity and the specificity of serum antiendometrial antibody screening have a wide range and their role as serum markers is still unconvinced [29]. The increasing evidence that oxidative stress is a key steps in the pathogenesis of endometriosis led to analyze oxidatively modified lipoproteins and their antibodies and this demonstrated that the latter were significantly increased in women with endometriosis without any correlation with the stage, symptoms or morphologic type of the disease [30]. Subsequently, many reports focused on the serum evaluation of other autoantibodies, such as antiprogestogen-associated endometrial protein antibodies and endometrial glycoproteins, antibodies directed against carbonic anhydrase, antibodies to collagen, albumin and IgG, transferrin, but all failed to identify a correlation between serum levels and endometriosis. Considering total immunoglobulins, they have been assessed in sera of women with endometriosis showing no differences with controls, even if the medical treatment with danazol exerted a significant reduction in all immunoglobulin subtypes studied (IgG, IgM and IgA) [31].
Other immunological products have been tested with contradictory results. In particular, elevated serum levels of C3c and C4 were found in women affected by endometriosis [32]. Serum levels of soluble HLA class I and II have been demonstrated to be significantly lower in women with endometriosis than control women [33].
Natural killer (NK) cells have been successfully studied in peritoneal fluid and eutopic endometrium, showing an altered NK cytotoxicity to endometrial tissue and cell cytotoxicity inversely correlated with the stage of the disease. However, some studies have failed to identify different levels of NK cells in peripheral blood, while other studies identify modification of NK subset in sera of women with endometriosis comparing controls [34].
Several promising results came from the analysis of neutrophils cells population. An interesting recent report focused on the concentrations of neutrophils in relation to lymphocytes, showing an increase in total white blood cell levels, and a particular increase in neutrophil levels in endometriosis. Furthermore, the analysis of neutrophils/lymphocytes ratio has been proposed as a diagnostic test since it demonstrated sensitivity and specificity of 60%. Furthermore, combining neutrophils/lymphocytes ratio and CA-125 levels, sensitivity improved over either test alone, but with slightly reduced specificity compared with CA-125 alone. The combined marker had a sensitivity of 69.3% and specificity of 83.9%, showing 13.5% increase in sensitivity but 8.9% decrease in specificity when compared with serum CA-125 [35].
Considering cytokines, IL-6 and TNF-α represented the most investigated types of cytokines. IL-6 is a proinflammatory cytokine involved in T-cell activation, B-cell differentiation and secretion of other cytokines and its response has shown to be dysregulated in macrophages in patients with endometriosis. Some studies have indicated a link between raised serum levels of IL-6 in endometriosis, but other studies have shown no link, using different cut-off values. In particular, Martinez et al. [36] found higher serum levels of IL-6 in women with Minimal-Mild endometriosis than other groups, including Moderate-Severe cases of endometriosis. Using the cut-off level of 25.75 pg/ml, the authors described a significant accuracy of IL-6 in detecting endometriosis (sensitivity 75.0%, specificity 83.3%), proposing IL-6 as a reliable, noninvasive marker of minimal and mild endometriosis.
The serum evaluation of other cytokines (IL-2, −4, −10, −12, −18, −13, −15, −16) did not produce any addition in finding correlation with endometriosis.
TNF-α plays a proinflammatory and proangiogenic role in the human endometrium, where it is related to physiological endometrial proliferation and shedding. In patients with endometriosis TNF-α raised in peritoneal fluid and some studies also showed that higher concentrations correlate with the disease stage. Considering TNF-α as serum marker, the results are still uncertain since some reports demonstrated an increase in TNF-α levels in women with endometriosis [37], while other authors showed no such difference [38]. On the contrary, increased levels of serum TGF-β have been reported in women with endometriosis and their concentrations appeared to correlate with stage of disease [39].
Lastly, recent studies evaluated other immunological factors, such as MPC-1, macrophage migration inhibitory factor and IFNg-inducible protein-10 (CXCL10). One study found a significant higher level of MCP-1 in early disease stages of endometriosis [39] and another demonstrated higher values in more severe stages [40]. Serum concentrations of migration inhibitory factor have also been studied as single marker or as member of a panel, and serum levels were significantly higher in women with endometriosis, especially in women with more advanced disease stages [41]. In 2009, our group focused on the study of CXCL10, which is involved in TH1-type immune responses. Evaluating serum levels, reduced concentrations were found in women with endometriosis compared with healthy controls with absence of statistically significant differences between women with early endometriosis and those with advanced endometriosis was found [42].
Other markers: apoptotic, cell adhesion & angiogenetic molecules
Accumulating evidence suggests that the endometrial cells from women with and without endometriosis have fundamental differences and endometrial cells from women with endometriosis have enhanced proliferation and increased ability to implant and survive in ectopic locations with an impaired sensitivity of endometrial tissue to spontaneous apoptosis. In endometriosis, it seems reasonable that an imbalance in peritoneal cleaning and excessive receptive mesothelium and cells have the ability to adhere to mesothelial cells of peritoneum, to proliferate and to produce neoangiogenesis resulting in the development of active endometriotic foci.
The percentage of apoptosis in sloughed endometrial cells was greatly reduced among women with endometriosis, implying that the number of surviving cells that enter the peritoneal cavity is greater in women who develop endometriosis. The Fas/FasL system plays a crucial role in normal tissue homeostasis and pathological conditions since their interaction is essential in inducing apoptosis. Cells expressing Fas undergo apoptosis on interaction with other cells expressing Fas ligand (sFasL). However, it also exists in a soluble form, and women with stages I–II of endometriosis had equivalent serum levels of soluble sFasL to controls, but levels were significantly increased in women with stages III–IV disease [43].
A variety of factors involved in cell adhesion have been studied in endometriosis and both soluble E-cadherin and vascular cell adhesion molecule-1 VCAM-1 serum levels have been found to be elevated in women with endometriosis [44]. The most relevant results come from the evaluation of intercellular-adhesion molecule-1 (ICAM-1) which has been hypothesized to be useful in the diagnosis of endometriosis, since ICAM-1 is demonstrated to be involved in the implantation and development of endometriotic lesions. Many investigators have reported a significant increase in serum concentration of ICAM-1 in patients with endometriosis and Somigliana et al. [45] found that women with deep peritoneal endometriosis had significantly higher concentrations than women without the disease and in those with superficial endometriosis. The sensitivity and specificity of soluble ICAM-1 (sICAM-1) in detecting deep peritoneal endometriosis were 19 and 97%, respectively, concluding that the measurement of sICAM-1 may be helpful in specifically identifying women with deep infiltrating endometriosis.
Considering neoangiogenesis, VEGF physiologically induces angiogenesis in endometrial tissue, allowing endometrium to repair after menstruation, but modulates also the characteristics of the newly formed vessels. The concentration of VEGF is increased in the peritoneal fluid of endometriosis patients and its levels raised also in sera of patients with endometriomas and other types of endometriosis [37]. Moreover, a prospective randomized case–control study demonstrated that there was a statistically significant difference in serum VEGF levels in patients with advanced endometriosis before conservative laparoscopic surgery and those without endometriosis and after conservative laparoscopic surgery, proposing VEGF as biomarkers for advanced endometriosis diagnosis [46].
Combined tests
The reported data indicated that a single specific serum markers for endometriosis has not been found yet and during last year many investigators proposed the use of combined test. Somigliana et al. [7] reported the results of the concomitant assessment CA-125, CA-19.9 and IL-6 failing in demonstrating that it could add significant data in respect to the CA-125 test alone. On the contrary, the association of serum and peritoneal fluid markers led to significant outcomes, showing that the concomitant dosage of serum IL-6 and peritoneal TNF-α provided to diagnose women with and without endometriosis accurately [47].
On these bases, recently many investigators focused their researches on a panel of markers. In 2010, D'Hooghe et al. [48] evaluated a panel of six possible serum markers (IL-6, IL-8, TNF-α, high-sensitivity C-reactive protein, CA-125 and CA-19.9) for the diagnosis of endometriosis and reaching a sensitivity and specificity of 100 and 84%, respectively, for moderate-severe endometriosis and a sensitivity and specificity of 87 and 71%, respectively, for minimal–mild endometriosis. The same authors continued their research analyzing a panel of 28 potential serum markers: the analysis of four biomarkers (annexin V, VEGF, CA-125 and sICAM-1/or glycodelin) enabled the diagnosis of endometriosis undetectable by ultrasound with a sensitivity of 81–90% and a specificity of 63–81% [49].
Proteomic & genomic: the new perspectives
Proteomic represents the new perspective in the field of serum markers and several authors have recently attempted to identify specific peptide and protein patterns to diagnose endometriosis. Proteomic technologies provide innovative ways to identify protein ‘fingerprints’ in blood and from these patterns of expression the identification of peptides or proteins that are up- or downregulated may allow to assess them as possible biomarkers of the disease.
The results are promising for determining high accuracy for the diagnosis of endometriosis, in terms of sensitivity and specificity, which is confirmed by many reports during the last years. In 2008, two different groups detected proteomic patterns in the sera of women with endometriosis: Wang et al. [50] identified five potential with a sensitivity of 91.7% and a specificity of 90.0%, while Jing et al. [51] based their diagnostic algorithm on two protein peaks reporting a sensitivity of 87% and specificity of 97%. The same investigators also found that one of these two peaks was significantly altered 1-month after surgery, suggesting that it may be a possible marker of disease stage or activity. More recently, the analysis of 24 different protein peaks has been reported, generating a sensitivity and specificity of 92 and 75%, respectively [52].
Sensitivity and specificity of new reliable serum markers.
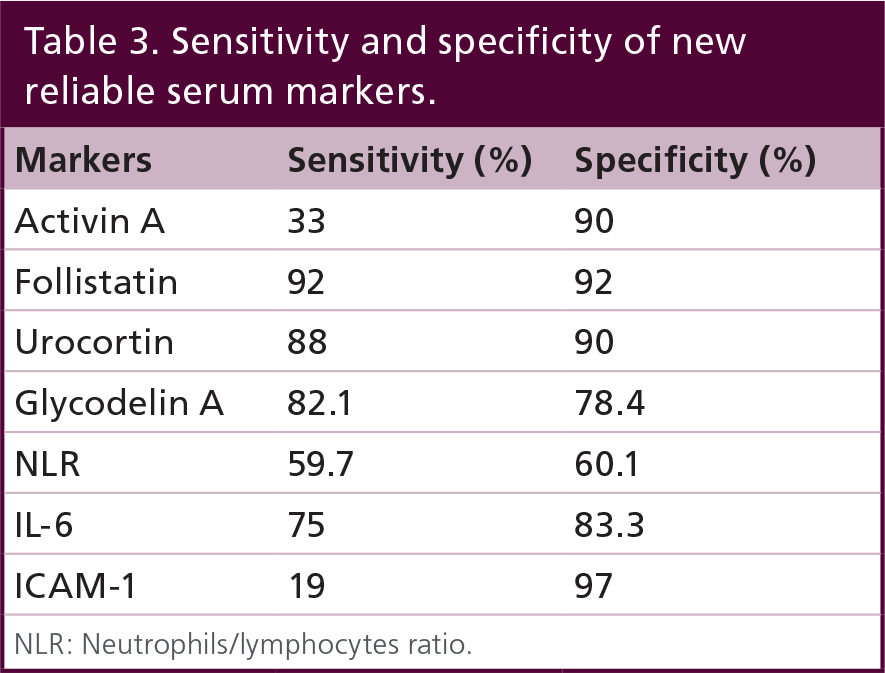
NLR: Neutrophils/lymphocytes ratio.
However, the multifactorial pathogenetic process of endometriosis also evokes the theory of a family inheritance and, as consequence, of a possible identification of genetic markers of the disease. Gene-based technologies include subtractive cDNA hybridization and cDNA microarray techniques. Moreover, circulating cell-free nucleic acids have been recently proposed as reliable markers of several diseases, and their evaluation in endometriosis showed that the concentration of circulating cell-free nDNA in plasma of the patient with endometriosis was significantly higher than in the control group [53].
Conclusion
Besides several serum biomarkers have been investigated over the years, with successful and contradictory results, none of these have been clearly shown to be of clinical utility (Table 3). Endometriosis is heterogeneous and still unknown disease and in its presentation may be determinant on the production of biomarkers; moreover the differences in studies-setups (different study and control groups, different assay) may lead to patient selection and detection bias, altering the overall results.
Future perspective
The more realistic diagnostic biomarker consists in a panel of biomarkers, even if the recent studies investigating the use of technologies such as genomics and proteomics may represent the future perspective of endometriosis diagnosis. These techniques together with other noninvasive tools, such as ultrasound and MRI, may decisively improve the diagnosis of endometriosis and patients' quality of life, as a consequence.
No writing assistance was utilized in the production of this manuscript.
Executive summary

Medical history, symptoms, pelvic examination together with imaging data may address the correct diagnosis of endometriosis, but the gold standard remains laparoscopic assessment with histological confirmation.
The development of serum markers as diagnostic tools for endometriosis may allow a prompt and noninvasive diagnosis, improving patients' quality of life.
Several serum biomarkers have been investigated over the years, but none of these have shown a clinical utility. Actually, the more realistic diagnostic biomarker consists in a panel of biomarkers.
The use of new technologies such as genomics and proteomics may represent the future perspective of endometriosis diagnosis.
Footnotes
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.