
Abstract
Women with an inherited BRCA1 or BRCA2 mutation face high lifetime risks of both breast and ovarian cancer [1,2]. Given the large impact of a bilateral salpingo-oophorectomy on reducing cancer incidence and all-cause mortality, women with BRCA mutations are routinely advised to undergo an oophorectomy to lessen their cancer risks [3]. Oophorectomy is typically recommended to women at age 35 years or after childbearing is complete [4]. There are various physiologic and psychological consequences of surgically induced menopause, including adverse effects on bone and cardiovascular health, as well as a decline in sexual functioning and an increase in vasomotor symptoms (i.e., hot flashes, night sweats) [5–9]. One potentially undesirable side effect is weight gain. Among women at average risk, weight gain after surgical or natural menopause has been documented and is associated with an increased risk of various diseases including coronary heart disease and diabetes [10–13].
A few studies suggest that hysterectomy with oophorectomy may be associated with increased weight gain [14,15], although these studies are of middle-aged women at average risk of cancer. To our knowledge, no studies have evaluated the impact of oophorectomy on changes in adiposity specifically among BRCA mutation carriers. We undertook this study to evaluate the impact of a preventive bilateral oophorectomy on weight gain, using prospective data from a large international study of BRCA mutation carriers.
Patients & methods
Study population
Eligible study subjects were identified at one of 72 participating centers in 13 countries. Women were participants in ongoing research protocols at the host institutions. These women sought testing for BRCA1 and BRCA2 mutations because of a personal or family history of breast and/or ovarian cancer. Mutation detection was performed using a range of techniques, but all nucleotide sequences were confirmed by direct sequencing of genomic DNA. A woman was eligible for the current study when the molecular analysis established that she was a carrier of a deleterious mutation in the BRCA1 or BRCA2 gene. There were 14,818 female BRCA mutation carriers enrolled in the parent study. All participants provided informed consent. The ethics committees of all participating centers approved the study. Details regarding mutation testing and data collection have been previously published [3,16].
Data collection
All study subjects completed a baseline questionnaire at the individual center at the time of a clinic appointment or at their home at a later date. The questionnaire requested information on family and personal history of cancer, reproductive and medical histories, including preventive oophorectomy. The questionnaire asked whether the woman had one or both of their ovaries removed (oophorectomy) for reasons other than ovarian cancer (for example, preventative measures, fibroids, cyst, scar tissue or pain), the year of the surgery, the reason for the surgery and the number of ovaries removed but did not distinguish between oophorectomy and salpingo-oophorectomy. The questionnaire also asked about body weight (pounds) at ages 18, 30 and 40 years, as well as current weight. Exposures, preventive procedures and disease incidence were updated every 2 years using a follow-up questionnaire that was either mailed to each study participant or administered over the telephone by a genetic counselor or research assistant.
Statistical analysis Case–control analysis
First, we performed a matched case–control analysis to compare the body weight of unaffected women who did and who did not have a bilateral oophorectomy in the past. We excluded women who: had a cancer diagnosis at the time of the baseline questionnaire (n = 8174), were missing information on body weight at baseline (n = 1004), had missing information on oophorectomy status or date of oophorectomy (n = 191). After these exclusions, 5500 women were eligible for analysis. Cases were women who had a bilateral oophorectomy (n = 1046) and controls were women with two ovaries intact (n = 4454). After n:1 matching on date of birth (within 1 year), BRCA mutation status (i.e., BRCA1 or BRCA2), country of residence, age at completion of baseline questionnaire (within 1 year) and prophylactic mastectomy status (yes/no), there were 405 matched sets available for analysis (405 cases and 741 controls). The distributions of continuous and categorical variables between cases and controls were compared using the Student's t-test and chi-square test, respectively.
Prospective follow-up study
Next, we evaluated whether a bilateral oophorectomy was associated with a change in bodyweight. For this analysis, we only included women who had a bilateral oophorectomy at some time (n = 1454). For each woman, we extracted all pertinent data that were available from the baseline and follow-up questionnaires, including age (years), weight (pounds), bilateral oophorectomy status (yes/no) and prophylactic mastectomy status (yes/no) at the time of completion of each questionnaire. For those women who reported a prophylactic mastectomy, we only included data obtained from the questionnaires preceding the date of the surgery.
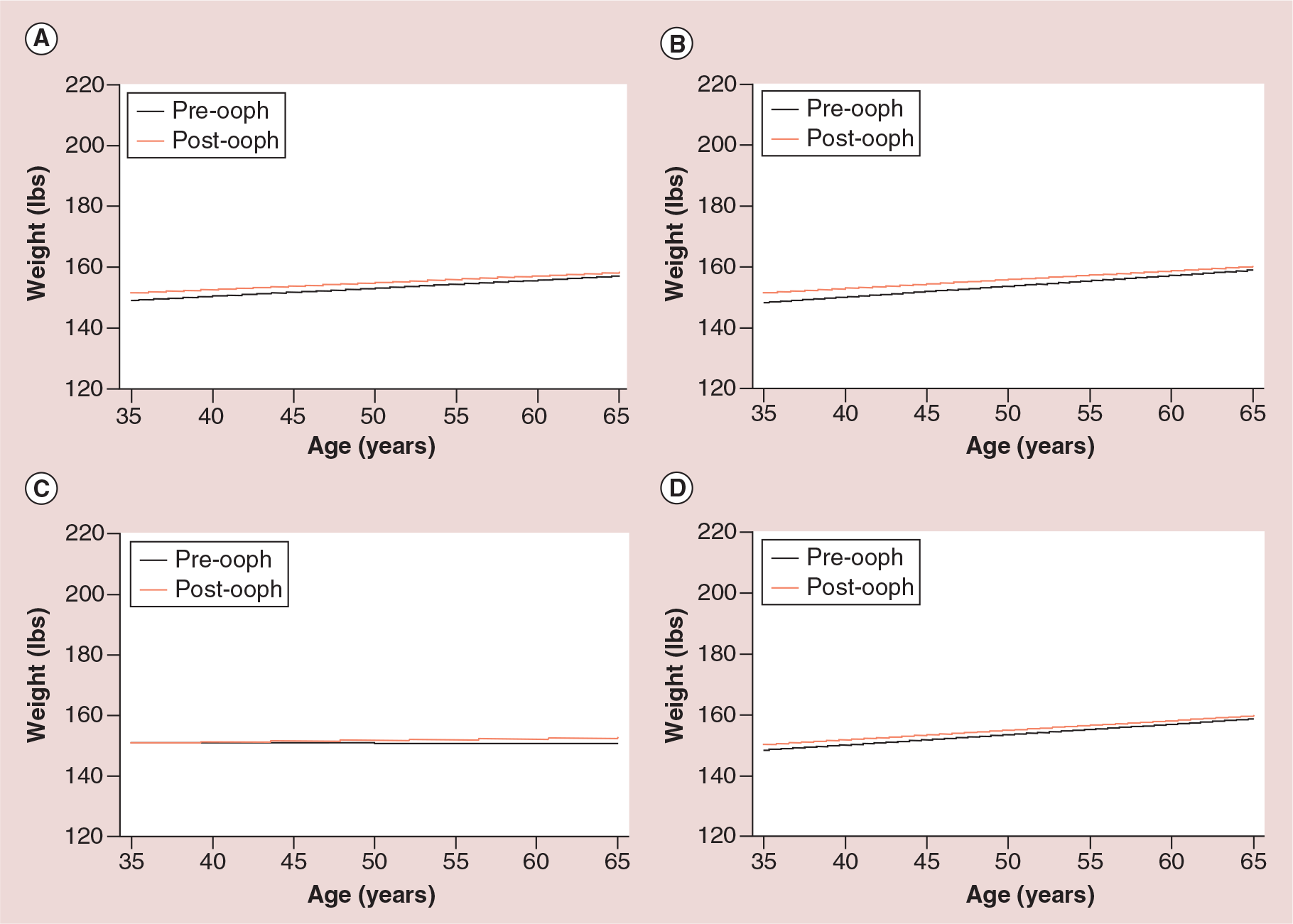
Linear regression was used to evaluate the rate of weight change with increasing age prior to and following a bilateral oophorectomy among all the eligible women who had an oophorectomy at some point, stratified by BRCA mutation status and by age at oophorectomy (i.e., <50 vs >50 years old). The F-test was used to compare the parameters of the regression equations (i.e., intercept and slope) prior to and following surgery.
All analyses were performed using the SAS statistical package, version 9.1.3 (SAS Institute, NC, USA). All p-values were based on two-sided tests and were considered statistically significant if p < 0.05.
Results
We studied 1146 BRCA mutation carriers who had no history of cancer at the time of completion of the baseline questionnaire; 405 reported an oophorectomy and 741 did not report an oophorectomy at the time of the baseline questionnaire (
Characteristics of BRCA mutation carriers with and without a bilateral oophorectomy at the study entry.

Women who had two ovaries intact at the time of the baseline questionnaire.
Women who had undergone a bilateral oophorectomy at the time of the baseline questionnaire.
Mean values for controls represent the means of the sets.
Refers to use in the women after bilateral oophorectomy.
In order to evaluate the relationship between parity, weight and weight gain in our study population (irrespective of oophorectomy status), we analyzed all the data points for parity, age and weight and constructed a regression curve (not shown). At age 50 years, the mean weight of nulliparous women was 147.04 pounds compared with 151.32 pounds for women with one child, 152.14 pounds for women with two live births and 154.99 pounds for women with three or more live births. There was no significant difference between the intercept or slope parameters after comparing any two regression lines of the four parity categories (p > 0.05).
Discussion & conclusion
The goal of the current study was to evaluate the effect of undergoing a bilateral oophorectomy on weight gain among women with an inherited BRCA1 or BRCA2 mutation. We restricted the analysis to unaffected women because of the known impact of a cancer diagnosis and subsequent treatment of the disease on body-weight [17,18]. First, we utilized information obtained from the baseline questionnaire and compared the bodyweight of women who reported having undergone an oophorectomy at study oasis:entry compared with those who did not. After matching for age, country of residence, BRCA mutation and prophylactic mastectomy status, women with a prior oophorectomy weighed, on average, 2.4 pounds more than women who had both ovaries intact. This difference was not statistically significant. Next, we studied 1454 women who reported an oophorectomy at some time during the follow-up period and compared their bodyweight trajectories prior to and following surgery. We found a significant positive relationship between bodyweight and age, irrespective of oophorectomy status. Those women who had a prior bilateral oophorectomy weighed 2–3 pounds more at any given age; however, at no age was this difference statistically significant. The effect of oophorectomy on bodyweight was similar among carriers of mutations in either BRCA1 or BRCA2 and for women who underwent surgery at or prior to age 50 years. These findings suggest that preventive removal of the ovaries may be associated with a small change in bodyweight.
Prior evaluations of preventive surgery and adiposity have been limited to women in midlife at average risk of cancer and included relatively few women undergoing bilateral oophorectomy [14–15,19]. No evaluations, to our knowledge, have been conducted among women with a hereditary cancer predisposition. In the largest prospective study to date (n = 1962 women aged 42–52 years), Gibson et al., evaluated the mean change in BMI before and after natural menopause, hysterectomy with ovarian conservation and hysterectomy with bilateral oophorectomy [19]. They found that BMI increases over the course of the menopausal transition and that this effect was steeper among women who had a hysterectomy with bilateral oophorectomy (n = 106) compared with those with natural menopause (n = 1780) or a hysterectomy alone (n = 76). Similarly, Sutton-Tyrell and colleagues reported that in their study of 3260 USA women, surgical menopause (hysterectomy with or without oophorectomy) predicted severe obesity compared with premenopausal or naturally postmenopausal women [14]. It should be noted that 60% of the 162 surgically postmenopausal women also had an oophorectomy. In contrast, an analysis of two large British birth cohorts found that hysterectomy with or without oophorectomy during midlife was not associated with weight gain compared with women with no hysterectomy or oophorectomy [15].
Among women in the general population, as well as in animal studies, aging, including the transition from premenopause to postmenopause, is associated with weight gain and an increase in central body fat deposition [11,20–23]. Changes in the source and quantity of sex hormones is reported to underlie many of these changes in fat distribution and weight gain [10]. A few studies have illustrated that oophorectomy is associated with metabolic syndrome, which is described as the clustering of abdominal obesity, dyslipidemia, hypertension and hyperglycemia, compared with women with intact ovaries [24–26]. Of relevance is a large study using NHANES III data from women aged 40 years or older (n = 4040), no significant increase in all-cause mortality with oophorectomy prior to age 40 years; however, they found that women who were obese at the time of oophorectomy had a twofold increased risk of cardiovascular disease mortality [27]. These findings suggest that overweight women undergoing early oophorectomy should be monitored for cardiovascular disease risk factors as well as for body weight.
There are numerous strengths and limitations associated with the current study. First, we used self-reported surgical and body size data that was gathered from a research questionnaire. Despite this, we only included information from women without a cancer diagnosis and there is no reason to suspect differential reporting among these high-risk, unaffected women prior to or following surgery. Prior studies have found that self-report of gynecologic surgeries is valid [28,29] and that the reproducibility and validity of self-reported height and weight are generally high [30,31]. A major strength of our study was the prospective assessment of weight change and the ability to exclude women with a cancer diagnosis and take into account prophylactic mastectomy status, which may have otherwise biased our findings. Although we did not evaluate other measures of adiposity (i.e., BMI or waist circumference), adult weight gain has been suggested to be a better measure of adiposity than BMI, because lean body mass decreases with age [32] and because BMI does not distinguish between lean and fat mass; whereas changes in adult weight largely reflect changes in body fat [33–35]. We cannot rule out the possibility of residual confounding by other factors including diet and physical activity.
In summary, this represents the first prospective reports of postoperative weight gain following oophorectomy in BRCA mutation carriers. We found that prophylactic oophorectomy is not associated with significant weight gain over time among women with a BRCA1 or BRCA2 mutation. Given the existing literature suggesting that physical activity and maintaining a stable weight significantly impact long-term well-being in high-risk women undergoing PBSO [36], mutation carriers considering surgery should be counseled on the beneficial effect of maintaining a healthy body weight on postsurgery quality of life. Although weight gain does not appear to be an adverse outcome of surgical menopause in this high-risk population, prevention of menopausal weight gain through exercise and reduced caloric restriction should be advocated to prevent other health conditions associated with obesity (i.e., coronary heart disease, Type 2 diabetes, and so on) [37].
Future perspective
Data from large-scale, ongoing studies of BRCA mutation carriers undergoing bilateral salping-oophorectomy will provide important information regarding both the short- and long-term consequences of oophorectomy on body weight as well as other health outcomes is of interest.
Other members of the Hereditary Breast Cancer Clinical Study Group
Christian Singer, Charis Eng, Jeanna McCuaig, Andrea Eisen, Joanne L Blum, Dana Zakalik, Tuya Pal, Mary Daly, Carrie Snyder, Taya Fallen, Albert Chudley, John Lunn, Talia Donenberg, Raluca N Kurz, Howard Saal, Judy Garber, Kevin Sweet, Edmond Lemire, Gillian Mitchell, Charmaine Kim-Sing, Olufunmilayo I. Olopade, Sofia Merajver, Louise Bordeleau, Carey A. Cullinane, Eitan Friedman, Wendy McKinnon, Marie Wood, Daniel Rayson, Wendy Meschino, Josephine Wagner Costalas, Robert E. Reilly, Susan Vadaparampil, Pal Moller, David Euhus, Ava Kwong, Claudine Isaacs, Fergus Couch, Siranoush Manoukian, Cezary Cybulski, Christine Elser, Seema Panchal, Susan Armel, Sonia Nanda, Kelly Metcalfe, Aletta Poll, Barry Rosen, Timothy Rebbeck, Ellen Warner, Lovise Maehle, Gareth Evans, Barbara Pasini, Ophira Ginsburg, Stephanie Cohen, Anna Jakubowska and Janice Little.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Executive summary
Women with an inherited BRCA1 or BRCA2 mutation are advised to undergo a prophylactic bilateral salpingo-oophorectomy at age 35 years or thereafter.
Furthermore, it is not known whether surgical menopause in this high-risk group has an impact on bodyweight.
We evaluated the impact of oophorectomy on bodyweight among unaffected women with a BRCA1 or BRCA2 mutation.
At baseline, women who had an oophorectomy weighed 2.4 pounds more than those who had both ovaries intact.
Our findings suggest a small but insignificant change in bodyweight with a preventive oophorectomy.
Footnotes
Acknowledgements
The authors would like to acknowledge the study coordinators M Llacuachaqui and A Ragone, as well as the students and staff J Ng, A Fine, S Chin, V Walter, D Bobrowski, S Bitzos, R Ndahigwa, E Meloche, K Cooke, G Francia, J Dirube and F Shoukat who helped with the data collection and data entry.
J Kotsopoulos is the recipient of a Cancer Care Ontario Research Chair in Population Studies and a Canadian Cancer Society Career Development Award in Prevention. SL Neuhausen is partially supported by the Morris and Horowitz Endowed Professorship and her work was supported by a grant from the NIH, R01CA74415. S Narod is the recipient of a Canada Research Chair tier I. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.