
Abstract
Ultrasonography is today the method of choice for distinguishing between benign and malignant adnexal pathologies. Using pattern recognition several types of tumors can be recognized according to their characteristic appearance on gray-scale imaging. Color Doppler imaging should be used only to perform a semiquantitative color score or evaluate the flow location. International Ovarian Tumor Analysis group had standardized definitions characterizing adnexal masses and suggested the use of ‘simple rules’ in premenopausal women. Recently, the use of 3D vascular indices has been proposed but its potential use in clinical practice is debated. Also computerized aided diagnosis algorithms showed encouraging results to be confirmed in the future.
Several researches have demonstrated that a common indication for gynecological surgeries are adnexal masses and [1] up to 10% of all women in the USA underwent surgery at least once in their lifetime for this reason [1].
Ultrasonography (US) is an easily executable procedure as well as repeatable, and with a relatively low cost and it remains the method of choice for distinguishing between benign and malignant adnexal pathologies [2,3].
An adequate characterization of adnexal masses is a fundamental step to plan the correct therapeutical approach [2–5]. In this paper, we will present the application of US in the detection and characterization of adnexal masses with particular emphasis to the new techniques and approaches.
The past
Thirty years ago the US studies were performed with the transabdominal approach but the relatively poor resolution associated with the use of lower frequency ultrasound usually determined suboptimal results [6]. With the introduction of the transvaginal probe, about 20 years ago, a significant increase in the accuracy was found and this method became the reference standard in the assessment of the adnexal masses.
Currently the transabdominal US has no indication with the only exception of virgo patients, when transrectal approach is difficult, or in the case of adnexal mass bigger than 10 cm, assessment of presence of ascites and metastases. Moreover, thanks to the use of higher frequencies it is possible to use of TV ultrasonography to investigate the structural morphology of the mass with an exquisite level of detail.
The first study that correlated the US finding and histology was performed by Granberg et al. in 1989; they understood that different morphologies were associated with an increased risk of malignant condition; in fact they found that unilocular cyst with smooth walls is a typical marker of benignity whereas solid projections into the cyst cavity increases the risk of malignancy [7]. Later, several morphological characteristics were described, including the internal structure of the cyst's walls and their thickness as well as the extension of septa and echogenicity of the content; by considering these parameters a sensitivity of 100% and a specificity of 83% were obtained [4].
The use of score systems
The diagnosis of ovarian cancer has been challenging and some authors suggested to use US ‘scoring systems’ based on the use of different sonographic parameters. During the years, several scoring systems and mathematical models helping to calculate the risk of malignancy have been suggested. One of the first score system was proposed by Sassone et al. [4] in 1991 [8–10]. One of the most important score system is the risk of malignancy index (RMI) and it was demonstrated that using an RMI cut-off level of 200, this score is effective in discrimination between benign and malignant ovarian masses with a sensitivity of 85% and a specificity of 97%. When an RMI score of greater than 200 is detected, patients have 42-times the background risk of cancer [8]. A recent published paper by Klangsin et al. [11] assessed the accuracy of the five sonographic morphology scoring systems (Sassone, DePriest, Lerner, Vera and Kawai and Valentin) for prediction of ovarian cancer and the sensitivities of the sonographic morphology scoring by Sassone, DePriest, Lerner, Vera and Kawai and Valentin were 75, 89.1, 82.8, 79.7 and 82.8% whereas the specificities were 79.3, 73.2, 68.3, 82.9 and 85.4%, respectively.
Pattern recognition
In 1999 a new method called ‘patter recognition’ [11,12] was introduced that demonstrated to have better performance in term of accuracy, sensitivity and specificity compared with all other ultrasound methods such as scoring systems and mathematical models for calculating the risk of malignancy. According to this method, some types of tumors can be recognized according to their characteristic appearance on gray-scale imaging (Figure 1). Pattern recognition considers specific ultrasonographic characteristics such as volume, localization, associated features as ascites, carcinomatosis, internal structure (wall, inner contour/papillary projections, septa, solid areas), echogenicity and the presence of shadow and/or Crescent sign. According to pattern recognition it is possible to classify the presence of the different types of ovarian neoplasms, in particular:

Example of specific structural ultrasonographic characteristics.
Simple cyst: it is a unilocular anecoic cyst without septa or without solid parts or papillary structures. With the pattern recognition it was demonstrated a good predictive capacity to distinguish between simple cyst/cystoadenomas and other ovarian masses (specificity of 96% and sensitivity of 79%) [13];
Endometrioma: it is a unilocular cyst with homogeneously hypoechoic content with fine internal echoes (‘ground glass’). In the 1995, the author showed that TV ultrasonography is a reliable diagnostic method both in screening that in the differential diagnosis of endometriomas and other types of neoplasms [14,15];
Dermoid: the most frequent echographic sign is the presence of localized or diffuse echogenicity frequently associated with a posterior acoustic shadow [16]. The presence of dermoid cyst can be suspected if there is one or more of this echo patterns: a dense echo pattern, thin echogenic band-like echos and a densely echogenic tubercle (Rokitansky protuberance). The use of these findings demonstrated a good predictive ability with sensitivity of 84.6% and a specificity of 98.2% [17];
Cystadenofibroma and ovarian fibroma: the presence of ipoecogenic mass with posterior acustic shadow suggests the presence of myomas or ovarian fibrothecoma [18]. It is complex to distinguish a pedunculated myomas from a cystadenofibroma;
Ovarian mucinous tumors: serous cyst(aden)oma, adenofibroma, mucinous cyst(aden)oma manifest overlapping characteristics. A serous cyst(aden)oma can show different patter: unilocular or bilocular with homogeneous echogenicity. Usually a thin and regular wall and regular, thin septum can be found. A mucinous cystadenomas to be ‘a multilocular cyst containing fluid of different echogenicities, with regular wall and septa, and no vegetations.’ The sensitivity of US grayscale is 75 and the specificity ranges from 75 to 96%, respectively. The sensitivity and specificity of gray-scale imaging for diagnosing mucinous cystadenomas were reported by Fleischer et al. to be 95 and 99%, respectively [19,20];
Paraovarian cysts: in some cases it may be challenging to distinguish an ovarian cyst from a paraovarian cyst [21] in particular when the ovary is not visible as a separate structure. Also the echogenicity of the cyst fluid may be variable from anechoic or echogenic [21]. Papillary projections and septa may be present. [22]. It is important to remember that in some cases in paraovarian cysts measuring >5 cm and with papillary projections a malignancy may develop;
Hydro-salpinx: the most frequent ultrasound features are: cystic structure with fluid-filled, sausage-shaped, presence of ‘incomplete septa’ and on a transverse section of a fluid-filled tube, mucosal folds are seen to protrude into the lumen, resulting in a ‘cog-wheel’ appearance if the tube is swollen and in a ‘beads-on-a-string’ appearance if it is not [23,24];
Peritoneal pseudocysts: this condition is characterized by the presence of irregular cyst with thin walls and internal septa. The irregular shape is due to the presence of adhesions fluid filled that mass following the contours of the pelvis (even though pseudocysts may also be oval or round) [25,26]. The cyst fluid may be anechoic or echoic. Ying et al. [27] find other sign that is the change of its shape when subjected to external pressure at the level of the abdominal wall by the left hand in conjunction with the transvaginal ultrasound examination. The pattern remains until today a fundamental and well-recognized approach in the diagnosis of adnexal masses.
Color Doppler flow
Studies in other anatomical districts showed that color and pulsed Doppler US are features that can improve the diagnostic accuracy of gray-scale morphologic sonography; for this reason from the 1989 authors tried to assess these parameter also in the diagnosis of the ovarian cancer. The first approach was performed in 1989 using the pulsatility index and also the resistive index. These indexes measure the impedance to blood flow. A low value suggests decreased impedance whereas a high value increases impedance to blood flow [28,29]. Initial reports were encouraging, but today's literature has conflicting results [30–33]. Most studies nowadays suggest that malignant ovarian tumors have lower impedance but there is a considerable overlap with benign neoplasms with a low specificity of the technique [34–38]. Therefore, several authors suggested to avoid cut-off values of blood flow indices for the detection of ovarian cancer [34,36–40] and the use of this approach should be abandoned. Fleischer et al. in 1993 [41] reported that peripheral vascularity is a sign of benignity whereas central vascularization is a sign of malignancy in the ovarian masses. Buy et al. [37] have proposed that the presence of color flow in a portion of an echogenic mass is indicative of six malignancy and the absence of it is suggestive of benignity; the presence or absence of flow at the level of a regular wall or septa would be index of benignity. [37] Guerriero et al. [39,42] suggested that color Doppler imaging should be used selectively to grade masses with central vascular flow or vascular flow within excrescences that were previously identified on B-mode sonography as malignant (Figure 2).

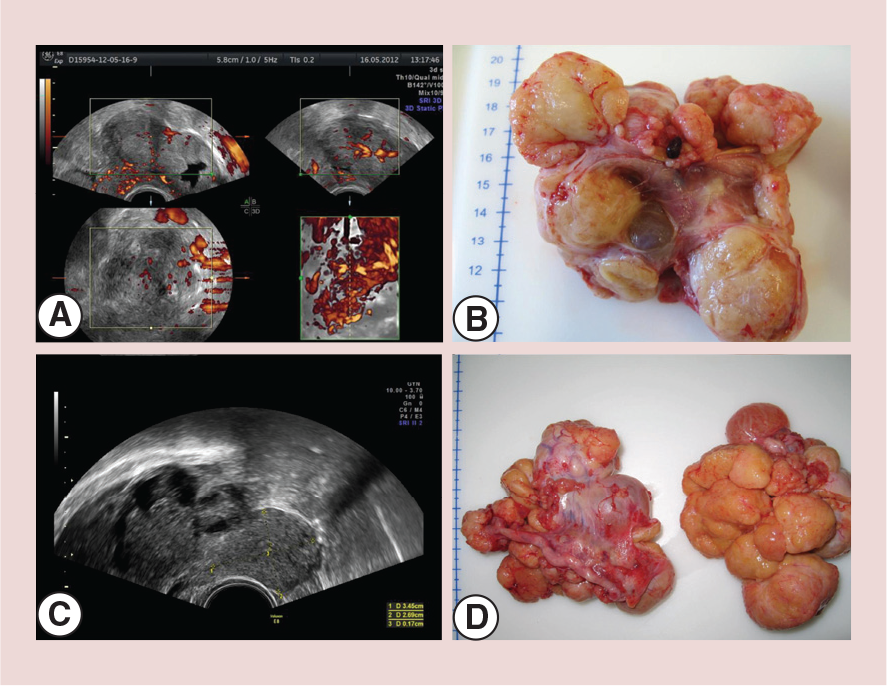
Diagnosis of adnexal malignancies by usingcolor Doppler imaging as a secondary test in persistent masses.
In 2010, a study performed through collaboration of two European university Departments of Obstetrics and Gynecology between 1997 and 2007 [43], compared the accuracy of ultrasonography with and without color Doppler imaging in the diagnosis of ovarian cancer. Each mass was graded malignant when the presence of flow at the level of vegetations or solid areas was detected whereas classified as benign if the flow was absent or peripheral. Diagnosis of adnexal tumors using gray-scale sonography is less accurate than diagnosis of adnexal masses using grayscale and color Doppler with specificity of 84 versus 94% and similar sensitivity (95 vs 98%). Guerriero et al. [44] showed that using color Doppler, in ‘high-risk’ adnexal masses (Figures 3–6) (those masses where papillary flow or solid portions is present) enables to make a validated decision regarding the best surgical approach (laparotomy vs laparoscopy). Also the use of color Doppler as second level test after gray-scale evaluation remains today a fundamental and well-recognized approach in the diagnosis of adnexal masses. A recent published paper by Saunders [43] showed that septated cystic ovarian tumors without solid areas or papillary projections have a very low risk of malignancy.



The present
The reproducibility of ultrasonography in the diagnosis of ovarian cancer
In these years, some methods have been proposed to create standardized protocols to characterize adnexal masses. The value of these methods rely to the fact that to have an homogeneous ‘modus operandi’ in the ultrasonographic assessment of the ovarian masses can significantly improve the interobserver agreement of the observers. New data are present today in the literature about the evaluation of the reproducibility of ultrasonography in the diagnosis of ovarian cancer using typical gray-scale patterns [45].
A recent study by Guerriero et al. demonstrated that using an homogenous protocol there is a good to optimal concordance among observers with different level of expertise (κ = 0.72–1). These results demonstrate that US malignant patterns could be reproducible, even in moderately experienced examiners.
The importance of IOTA studies
In the last years a consensus was presented by the International Ovarian Tumor Analysis (IOTA) group, with the purpose to create standardized terms definitions and measurements characterizing adnexal masses [46]. In IOTA, adnexal masses were classified into five categories: unilocular cyst, unilocular solid cyst (a unilocular cyst that contains at least one solid part which could be a papillary projection that protrude the cavity with height of 3 mm or more), multilocular cyst, multilocular-solid cyst (a multilocular cyst that contains at least one solid part) and solid cyst (that contains at least 80% solid tissue) (Figure 7). The cystic contents can be classified as: anechoic (black), low-level echogenicity, and ground glass appearance (as often seen in endometriotic cysts), (4) hemorrhagic and (5) mixed (often seen in teratomas) (Figure 8). The degree of vascularization within the septa, cyst walls or solid tumor area was assessed using a score between one and four. Color score one is used when no blood flow can be found in the lesion, color score two if minimal flow can be detected, color score three is given when moderate blood flow exists and color score four for marked blood flow.


In the last years the IOTA group has proposed several predictive model for ovarian cancer including: logistic regression model 1 (LR1) [47,48], logistic regression model 2 (LR2) [47,48], simple rules (SR) [49] and simple descriptors (SD) (instant diagnosis) [50,51]. LR1 has 12 independent prognostic variables whereas LR 2 represents a simpler version, using only 6 selected variables (Table 1). LR1 has a sensitivity and specificity of respectively 92 and 87% with an AUC of 0.96. LR2 has obtained an AUC of 0.95 with a sensitivity of 92% and a specificity of 86% [52]. LR2 is preferred in clinical practice (Table 2) [53] because more simple compared with LR1.
Logistic regression model 1 and Logistic regression model 2.

LR1: Logistic regression model 1; LR2: Logistic regression model 2.
Data taken from [47].
Comparison of performance of International Ovarian Tumor Analysis models in two studies.
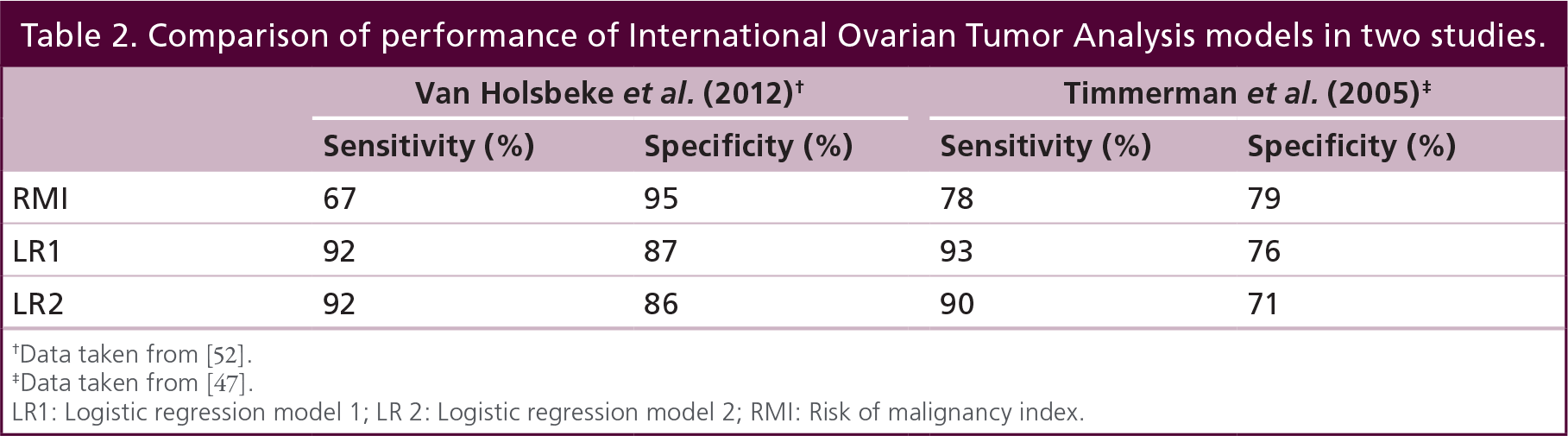
Data taken from [52].
Data taken from [47].
LR1: Logistic regression model 1; LR 2: Logistic regression model 2; RMI: Risk of malignancy index.
Simple rules
A tentative to simplify the US approach to the adnexal masses is the proposed use of SR. SR is a descriptive model that consists of five sonographic characteristics with highest positive predictive value with regard to malignancy (M-rules) and the five SR to predict a benign tumor (B-rules).
The model is quite simple: if one or more M-rules is present in the absence of a B-rules the mass is classified as malignant whereas If one or more B-rules apply in the absence of a M-rules the mass is classified as benign. When M-rules and B-rules are present at the same time or if no rules apply, the mass cannot be classified with the SR [49] (Table 3).
Simple rules.

B-rules: benign rules; M-rules: malignancy rules.
Data taken from [49].
The following three characteristics are linked with an increased risk of malignancy: a solid tumor ascites, or a high color content using color Doppler (LR+ 5.09, 14.52 and 6.17, respectively) whereas unilocular cyst, acoustic shadowing and the absence of detectable tumor blood flow decreased the risk.
The risk of malignancy was found to be high also in irregular unilocular-solid tumors and irregular multilocular-solid tumors, when they are vascularized or large (≥100 mL). It is important to underline that the rules were applicable in only 76% of the cases with a sensitivity of 95% and a specificity of 91% [49,54].
This represents a limit of this approach and that the rules worked rather well in tumors that are usually easily classifiable using pattern recognition for example endometriomas, dermoid cysts, simple cysts and malignant tumors at an advanced stage, but they work less well in tumors that tend to be more difficult to classify 10 using pattern recognition, with the exception that hydrosalpinx is relatively easy to classify using pattern recognition [12,55], while the rules did not work well for hydrosalpinx, tumors to stage I and stage I invasive cancers).
In 2013, Alcazar et al. [56] tested the diagnostic efficacy of ‘SR’ also in less expert operators with good results in terms of sensibility and specificity. Other authors found that the SR are reasonably reproducible among observers with different level of expertise when assessed in stored 3D volumes [57]. For these reasons, the use of SR has proved to be a reliable method to distinguish between benign and malignant masses and can be easily used by operators with less experience.
Instant diagnosis or ‘simple descriptors’
In the 2013, Bourne et al. proposed a multicenter prospective external trial designed to assess the diagnostic results of the IOTA. This trial was performed by examiners with different background and level of experience and a three-step model was used: in the step one, SD were used; in the step two, the ultrasound SR whereas in the step three the subjective assessment (SA) of ultrasound images by expert operator was considered [50,51]. The SD, were used to identify ‘easy to classify’ masses and if SD did not apply, the SR were used. In last phase, for those masses where neither rules nor descriptors were applicable, SA by experienced examiners was used as the final test.
The SD comprises six parameters based on US and measurements of serum CA-125: four describe the features of benign tumors, while two describe probable malignancies. The benign SD are: unilocular cyst and ground glass content in a premenopausal woman, unilocular cyst with acoustic shadows in a premenopausal woman, anechoic simple cyst with regular wall less than 10 cm and all remaining regular walled cysts. The malignant SD are: more than 50 years old and CA125>100 IU/mL and at least moderate Doppler color score and ascites in a postmenopausal woman. The SD could be applied in less than the 50% of the cases. This approach seems to work adequately also in the hands of examiners with less experience in ultrasonography (Table 4). It is important also to remember that the dimension of the lesion is an important parameter and that most of small-to-medium size neoplasms will resolve spontaneously and can be followed conservatively with serial US. Modesitt et al. demonstrated that in unilocular ovarian neoplasms less than 10 cm, the risk of malignancy is extremely low [51].
International Ovarian Tumor Analysis prediction models and risk of malignancy index.
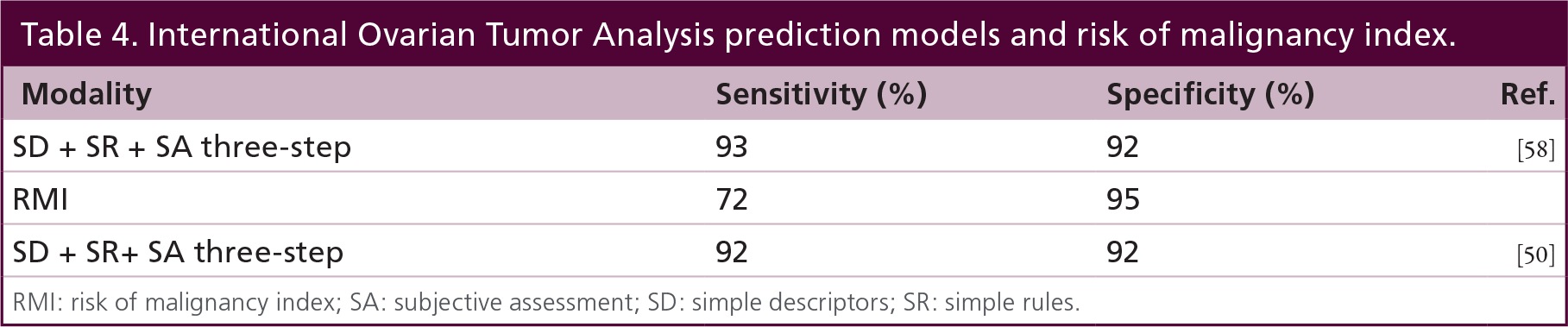
RMI: risk of malignancy index; SA: subjective assessment; SD: simple descriptors; SR: simple rules.
The future
3D ultrasound
3D ultrasound (3D-US) allows the acquisition of 3D volumes [59,60] that can be digitally stored and further evaluated using dedicated software. The 3D volume can be ‘virtually navigated’ and manipulated in multiplanar display, which simultaneously shows three orthogonal planes (axial, longitudinal and coronal) allowing navigation through these planes (Figure 9). This approach can be considered a paradigm shift in the US field because allows two new important features: the potentiality of assess the US information multiple times and in different places and time and to assess the US data according to multiple planes, selected by the observers, similarly to the volumetric computed tomography data.

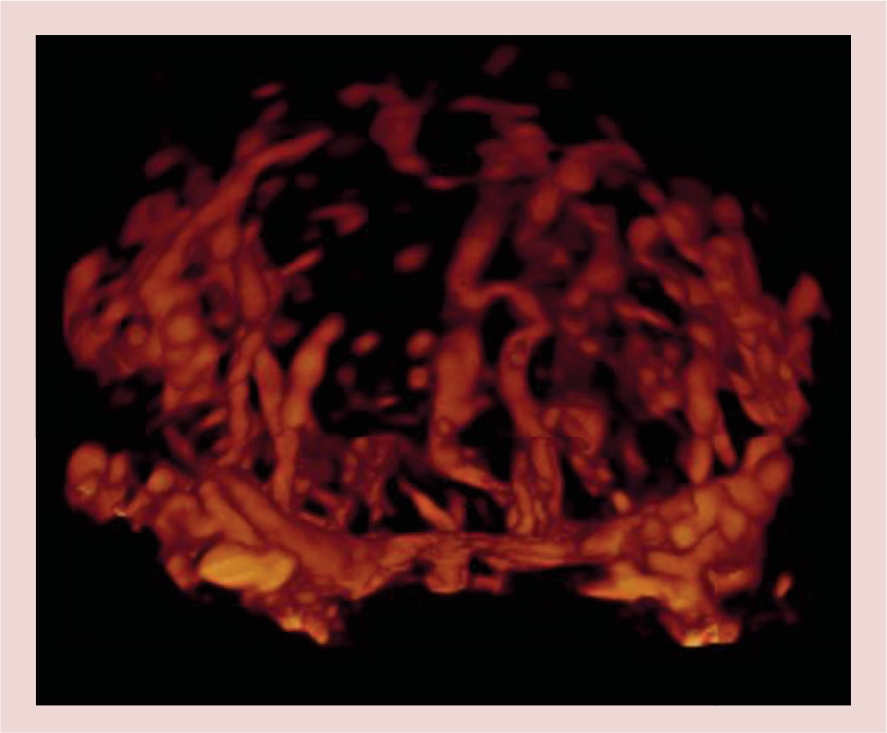
3D reconstruction of the vascular tree from an ovarian tumor depicted by power Doppler ultrasound.
Using the 3D-US it is possible to use three main modalities: the ‘inversion’ mode that shows as ‘white’ what is a fluid-filled structure giving a more precise idea of the shape the cystic cavity (Figure 10); surface rendering that shows surfaces or allows a 3D reconstruction of vessels (Figure 11) and tomographic ultrasound imaging that presents images like CT does (Figure 12).


Tomographic ultrasound imaging of an ovarian malignant tumor.
Another important ability of 3D-US is volume calculation even in irregularly shaped structures and with the 3D power Doppler angiography is possible evaluate ‘real’ vascularity of each organ and tissue with the reconstruction of the vascular tree (Figure 9, Figure 10 & Figure 12) that can be subjectively analyzed [61] but also, using dedicated software, evaluated by power Doppler-derived indices [62]. The most used indices are the vascularization index (VI), flow index (FI), and the vascularization-flow index (VFI). The VI reflects the amount of vessels and it measures the ratio between the number of color voxels and total number of voxels. The FI is the average color value of all color voxels and it shows the intensity of flow within those vessels. VFI represents both blood flow and vascularization and it is a derived parameter from VI and FI.
Gray-scale 3D ultrasound
Several studies about the role of gray-scale 3D-US in the diagnosis of ovarian cancer have been published but the results are still debated. As a matter of fact although the reproducibility of the technique, in term of intraobserver and interobserver, is good [63], 3D-US seems to have a good diagnostic performance for predicting malignancy in adnexal masses with specificities ranging from 78 to 100% and sensitivities ranging from 90 to 100%. Further studies are needed for the definitive introduction in the clinical practice. In several cases, 3D ultrasonography reinforced examiner's diagnostic impression. Additionally some authors investigated the use of 3D-US for diagnosing some specific types of lesions. [64–67]. In particular, Alcázar et al. showed that the objective analysis of cyst content by calculating the so-called mean gray value could improve the performance of 2D-US for the diagnosis of ovarian endometrioma [65]. The results of this study have been confirmed also by Guerriero [67].
3D power Doppler ultrasound
3D power Doppler ultrasound (3D-PD-US) can be used to evaluate the morphology of the vessels by identifying all those changes suspicious for malignancy but also to quantitative analyze tumor vascularization. The 3D-PD-US using a morphological approach showed specificities ranging from 50 to 100% and sensitivities ranging from 75 to 100% [68–74]. The accuracy in the diagnosis of ovarian cancer is good but according by Alcázar et al. can be achieved also by using a simpler technique such as 2D power Doppler [75]. The criteria of presence of malignancy using 3D power Doppler were: irregular branching (>3 branches and close to 90° angulation branching), vessel caliber narrowing, microaneurysms and vascular lakes. Good results were also found in the subjective evaluation of the morphology of the vessel tree, in term of specificity and sensitivity and they can be used to discriminate between benign and malignant ovarian tumors. Further studies should be addressed to evaluate only masses difficult to classify even for experienced observers as stated by Sladkevicius and Valentin represent approximately 10% of adnexal masses. These difficult tumors are often borderline tumors or papillary cystadenofibromas.
In addition, a further option that can be used is the remote off-line assessment that shows a good agreement with real-time ultrasound [76]. 3D volumes have been also used in the training of less expert operators. In a study of Alcazar et al. [77] 3D ultrasonographic volumes has been used in specific training program for ultrasound diagnosis of adnexal masses. The authors found that after 170–185 examination the observers reach a sensitivity of >95% and a specificity of >90%.
Alcazar et al. [78] recently published a study where they proposed the off-line assessment of 3D-PD-US vascular indices (FI – VI – FVI), within the most suspicious vascularized area of the tumor and Geomini et al. using a similar approach, demonstrated that FI, but not VI and VFI, was significantly higher in ovarian cancer. Jokubkiene et al. proposed a different approach based on a 5 cc spheric volume of interest from the most vascularized area from the tumor [79] and found that these indices from the spherical sample were higher in ovarian cancers as compared with benign tumors. Similar results were obtained by Kudla et al. [80]. All these methods seem reproducible [79,81–82]. Some studies reported [83–89] have shown that the use of 3D power Doppler angiographyvascular indices could be useful to improve the specificity of conventional gray-scale and 2D power Doppler ultrasound in selected cystic-solid or solid adnexal masses with specificities ranging from 33 to 77% and sensitivities ranging from 91 to 95%. However, it should be borne in mind that the actual significance of these indices is not fully understood, there are some important technical limitations for this technique and standardization is lacking [90–93]. Thus, its potential use in clinical practice is debated [94,95].
Computer aided diagnosis technique
Due the algorithms evolution and the increase in the hardware performance of the computer today it is possible to design artificial intelligence systems that automatically process the images and that can detect and characterize several kind of human lesions. These algorithms are known as computer aided detection/diagnosis (CAD).
CAD technique that uses ultrasound images of the ovary has been proposed to accurately classify benign and malignant ovarian tumor images. The mathematical model beyond these techniques is complex but can be summarized in these five steps: preprocessing, feature extraction, feature selection, classifier development and classifier validation.
Until now there are very few studies in the application of CAD for ovarian cancer detection. CAD algorithms show encouraging results and Acharya et al. [96] were able to achieve a sensitivity of 99.2 and specificity of 99.6% in the diagnosis of ovarian cancer. This approach is automated fast and accurate and in the future could be adjunct tools in helping physicians make a more confident diagnosis. These results need to be confirmed in larger populations before to introduce it in the routine clinical practice [96–99].
Contrast-enhanced ultrasound
Real-time contrast-enhanced ultrasound technology, using a second generation contrast agent containing sulfur hexafluoride microbubbles, has been proposed to depict vascularity in tumors. Unfortunately, although promising studies [100,101] have published some years ago, in a international multicenter study [102] performed on 134 patients ultrasound contrast examination seems not superior to conventional ultrasound techniques.
In addition the same study that there is a significant overlap between peak contrast signal intensity in borderline tumors and benign tumors, whereas a statistically significant difference is detectable between malignant tumors and borderline tumors/benign tumors.
Further studies should be performed, also using other molecules, to establish the potential role of this method in the detection and characterization of ovarian neoplasms.
Ultrasonographic screening for ovarian cancer
In the last part of this paper we would like to present the results of some important multicentric trail that have assessed the diagnostic performance especially in the controversial field of screening for ovarian cancer. One of the most important is the UK Collaborative Trial of Ovarian Cancer Screening published in Lancet Oncology in 2009 [103]. This trial was designed as randomized controlled and the purpose was to assess the effect of screening on mortality. The number of enrolled patients in the 5 years of the study is extremely big (n = 202638) and about 25% of these underwent yearly US assessment. Study results showed that US has a good specificity with better performance obtained associated CA-125. Another important trial published by van Nagell et al. in 2011 [104] had the purpose to assess the effect of US screening in detecting ovarian cancer and in the 25 years of the study (1987–2011) 37,293 women underwent US screening. The authors found 62 tumors and the 5-year survival rate was 75 compared with 54% for unscreened women (p < 0.001). This is an important study that demonstrates that US screening of asymptomatic women allows identifying more early-stage ovarian cancer with a statistically significant improvement in the survival rates. Similar results were found in another prospective randomized trial performed in Japan from 1985 and 1999 and published in 2008 [105] with more than 82,000 patients; the authors found that number of stage I was higher in the group of woman that underwent US screening but at that time they did not obtain a statistically significant difference. Another important trial performed on 39,337 women in the frameshift of the Kentucky Ovarian Cancer Screening Program [106] showed that many ovarian abnormalities assessed with US resolve, even if the initial appearance is complex, solid or bilateral. This is important because demonstrated that some complex structures are transient and resolve with serial inspection therefore, following these structures can ultimately distinguish benign from malignant structures that persist. In the next few years, the conclusions of some trials as UK Collaborative Trial of Ovarian Cancer Screening could further modify our knowledge about screening for ovarian cancer.
Executive summary
Using ‘pattern recognition’ several types of tumors can be recognized according to their characteristic appearance on gray-scale imaging.
Color Doppler imaging should be used selectively to grade masses with central vascular flow or vascular flow within excrescences that were previously identified on B-mode sonography as malignant.
International Ovarian Tumor Analysis group had standardized terms definitions and measurements characterizing adnexal masses.
Simple rules (SR), a descriptive model that consists of five sonographic characteristics with highest positive predictive value with regard to malignancy (M-rules) and the five SR to predict a benign tumor (B-rules) reported a sensitivity of 95% and a specificity of 91 % but applied in the 76% of the patients with an adnexal masses.
Although the simple descriptors could be applied in less than the 50% of the cases, using a three steps approach including SR, the sensitivity obtained is 93% with a specificity of 92%.
The use of 3D power Doppler angiography vascular indices could be useful to improve the specificity of conventional gray-scale and 2D power Doppler ultrasound in selected cystic-solid or solid adnexal masses but its potential use in clinical practice is debated
Computer aided diagnosis algorithms show encouraging results with a sensitivity of 99.2% and specificity of 99.6% in the diagnosis of ovarian cancer but these results need to be confirmed in larger populations before to introduce it in the routine clinical practice.
Conclusion
In the last years, gynecologists have been experienced a significant evolution in the US potentialities in the detection and characterization of ovarian masses. Nowadays US allows to identify the morphologic, as well as structural and vascular characteristics of the adnexal neoplasm by avoiding unnecessary surgeries and. The use of US, in particular the serial approach is very helpful because some complex structures are transient and resolve with serial inspection.
Future perspective
In the next future, ultrasonography will interact further with other new technologies as mobile operating systems. Already LR1 and 2 are present as mobile APP for use in smartphone and tablet. Using this modality the operator can, during the scan, introduce the observed variables and obtain the risk of malignancy in few seconds at the end of examination. Also a recent study of IOTA group [107] develops a risk prediction model, called ADNEX to preoperatively discriminate between benign, borderline, stage I invasive, stage II–IV invasive and secondary metastatic ovarian tumors. This model, now present in internet, should be in the next future implemented as APP.
Several national and international societies are trying to improve the knowledge of the operators directly organizing several courses. In particular IOTA group will perform courses to obtain a IOTA certificate that ensures the knowledge of IOTA variables, SR and SA of ultrasound images of adnexal masses.
The use of 3D power Doppler has been criticized by a recent paper published by our group [108] but further studies are necessary to obtain final results.
In addition some ex vivo optical imaging technologies [109] but in particular molecularly targeted microbubbles and US imaging [110] has been proposed in the noninvasive assessment of the level of expression of three angiogenic markers, as integrin, endoglin, and VEGFR 2, on tumor vascular endothelial cells in vivo during tumor growth. This new frontier is at the moment very preliminar for the use in humans.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.