
Abstract
Keywords
In 2006, the Institute of Medicine (IOM) issued its landmark report, From Cancer Patient to Cancer Survivor: Lost in Transition [1]. The IOM called for an orderly progression from cancer treatment to cancer survivorship. In the ensuing 8 years, many gains have been realized for breast cancer survivors including survivorship care planning, attention to late treatment effects, changes toward healthy behaviors after treatment and changes in our understanding of cancer survivors' psychosocial needs and economic burden.
These gains, however, have not been realized in minority breast cancer survivors, particularly Latinas. Reasons for the disparity are multifactorial and include systemic factors, cultural factors or a combination of both [2–5]. Systemic barriers include limited access to care, lack of insurance and poverty [2]. Cultural barriers include low education, poor communication because of language or translation problems and lack of ethnically and culturally sensitive healthcare systems [6].
Breast cancer is the most prevalent cancer among Latinas with an estimated 17,100 new cases diagnosed annually in the USA [7]. Despite lower breast cancer risk, Latinas are diagnosed at younger age, with advanced disease, and have poor survival compared with Caucasian women [7,8]. Latinos are the largest ethnic minority group in the USA, and the fastest growing minority population [9]. Currently, there are more than 120,000 Latina survivors in the USA [7], with the number of Latina survivors expected to increase [2].
Cultural and ethnic disparities exist between Latina breast cancer survivors (LBCS) and Caucasians [10,11]. Latina survivors report poor overall quality of life compared with other ethnic minority survivors [11,12]. Latinas also report heavy economic burden, social distress and poor mental health [13,14].
Despite the growing number of LBCS, combined with the psychosocial distress and poor quality of life reported by LBCS, there are comparatively few effective breast cancer survivorship interventions available. The authors located only four Latina intervention studies. The first, Latina a LatinaSM, is a breast cancer decision support intervention geared toward decision support for adjuvant therapy, not survivorship [4]. The second study reported by Napoles-Springer et al. [3] described culturally competent peer support intervention for recently diagnosed Latina breast cancer patients, not survivors.
The third paper reported by Molina et al., in an extensive review of the literature on interventions across the cancer continuum for US-based Latinas, found only one pilot study of a physical activity intervention for Latinas [2]. The pilot study was conducted by Hughes et al. and included 25 Hispanic breast cancer survivors [15]. And the fourth study by Juarez et al., reported the findings of Nueva Luz, a pilot educational intervention with 52 Latina breast cancer survivors [16]. In both papers, the authors briefly described the translation of the intervention materials. Hughes used forward and backward translation; Juarez explored cultural core values and linguistic factors in the design and delivery of Nueva Luz. It is not known whether either study was initially developed for non-Hispanic White populations.
Nevertheless, the two Latina intervention studies represent a beginning attempt to reduce survivorship disparities in this population. Multipronged approaches can also address cancer survivorship disparities among Latinas, whether the approach is the development of programs specifically for Latinas or the adaptation of existing or evidence-based interventions for non-Hispanic White survivors. Here, the authors describe an example of the latter approach in which an evidence-based survivorship intervention developed for non-Hispanic Whites, the Breast Cancer Education Intervention (BCEi), was translated to Spanish and culturally assessed through cognitive interview; subsequent changes were pilot tested with LBCS.
Background of the BCEi
The BCEi is a randomized trial demonstrating that a psychoeducational support intervention improved quality of life outcomes in early stage breast cancer survivors. The specific details of the study are reported elsewhere [17]. Briefly, early-stage breast cancer survivors near end of primary treatment were recruited from a regional cancer center in Central Florida. After informed consent and baseline measures, 261 BCS were randomly assigned to either an Experimental or Wait Control group. The Experimental group received three face-to-face education and support interventions delivered by a trained oncology nurse with each session lasting an hour. An extensive education binder and tip sheets supplemented the face-to-face education.
The first session focused on physical side effects and late side effects including: pain, lymphedema, fatigue, sexual and menopausal problems; with a focus on improving health behaviors such as nutrition and physical activity. This session included a discussion of the guidelines or recommendations for follow up and cancer surveillance. The second session delved into psychosocial, work, family, financial and economic changes occurring after treatment. The third session explored the potential for personal growth and advocacy after treatment. The Wait Control group received the same intervention after a 3-month waiting period. Both groups received monthly face-to-face followup with an assigned oncology nurse with study participation lasting 6 months.
Results showed significant differences in quality of life outcomes between Experimental and Wait Control group that were sustained over time. While effective, the study sample comprised less than 5% of Latinas who identified the major barrier to participation being language.
Subsequently, the BCEi was cited in a recent Cochrane review as an effective intervention for breast cancer survivors [18]. The BCEi was also evaluated by the Research Tested Interventions in Practice (RTIP) program at the National Cancer Institute and recommended for widespread public distribution [19]. Subsequently, the BCEi was adapted for older, rural and African-American breast cancer survivors [20,21]. In an effort to extend survivorship interventions to LBCS and to reduce language, linguistic and cultural barriers, the following reports the process of adapting the BCEI for LBCS through translation, cognitive interview and pilot testing.
Materials & methods
The authors received appropriate Institutional Review Board approval from the Department of Health in the State of Florida and the University of Alabama at Birmingham. This present study used a descriptive design using cognitive interview and survey. First, the BCEi education print materials were professionally translated. Second, an evaluation of the cultural relevance and readability of the Spanish translation was established. And third, a pilot evaluation of the satisfaction and usefulness of the education materials was conducted. Figure 1 is a schematic of the adaptation process.

Process of adapting an evidence-based survivorship intervention for Latina breast cancer survivors.
Certified translation of the BCEi print materials The BCEi print materials were contained in a 133 page binder that was divided into six modules. Thirty-seven Tip Sheets of short bulleted suggestions accompanied the modules. The BCEi print materials were used by trained oncology nurses for three, one-on-one teaching and support sessions. Teaching materials were organized within a quality of life conceptual model recognizing the interaction of physical, psychological, social and spiritual well-being, and emphasized patient self-management in survivorship care.
Modules 1 & 2 reviewed common physical late effects such as cancer-related fatigue, lymphedema, pain, menopausal symptoms, sleep problems, sexual function and fertility and self-management techniques. Modules 3 & 4 examined strategies to promote healthy lifestyle behaviors such as physical activity, nutrition and diet and cancer surveillance. Modules 5 & 6 explored psychological late effects and personal growth after breast cancer. All the English version print materials of the BCEi are available for public use at the Research Tested Interventions into Practice (RTIP) website [19].
The BCEi print materials were translated from English to Spanish based on the US Census Bureau Translation Guidelines [22] and the Consumer Assessment of Healthcare Providers and Systems, also known as CAHPS® [23,24] which are consistent with cross-cultural and Hispanic research [25,26]. Both guidelines recommend a two-step process of certified translation followed by assessment of cultural relevance using cognitive interview instead of backward translation.
The BCEi education materials were translated by a certified translator. The Fry Readability Index was used to keep the materials at a sixth grade reading level consistent with the original English version [27]. A basic Spanish vocabulary called ‘broadcast Spanish’ [25] was used for translation. Because broadcast Spanish is not based on a specific Latin American country or region, it can be understood by the majority of native Spanish speakers. The rationale for using broadcast Spanish was to recognize the diversity in idiomatic language used among Florida Spanish speakers whose origins are primarily from Cuba (28.7%) and Puerto Rico (20.1%) along with many other Latin American countries [28].
Cognitive interview
Instead of traditional backward translation, cognitive interviews with a small group of Latinas were conducted to assess cultural relevance and readability. A convenience sample of bilingual Latinas from the community was asked to participate in an individual cognitive interview lasting up to 2 h. Four Latinas agreed to participate and were mailed a copy of the certified translation. They were asked to note any words or phrases that were or were not understandable, comment on the usefulness of the cancer survivorship content and jot down suggestions for change in any aspect of cultural relevance, comprehension and/or wording. They were asked to bring their written comments to the interview. Using both Census Bureau and CAHPS guidelines, cognitive interview was used instead of backward translation because translation alone cannot address cultural relevance. While n = 4 is not a reasonable sample size for qualitative research, it is an acceptable number to assess cultural relevance through cognitive interview. Moreover, cognitive interview samples are not the same as those required for a qualitative study.
Four native-born Latinas from South and Central America (i.e., Puerto Rico, Colombia and Venezuela) with average age of 44.5 years (range 40.6–51.4 years) volunteered to participate in the cognitive interviews. All were bilingual; two preferred to speak Spanish in the home. Participants were married, with at least high school education, and worked full or part time. Two were Latina breast cancer survivors, and two were co-survivors. Open-ended questions assessed cultural relevance of the Spanish translation. Participants were asked whether additional words could enhance their understanding of cancer or survivorship terms, the ease of readability and any suggestions for deletions or changes to the content. All interviews were tape recorded.
Analysis & themes
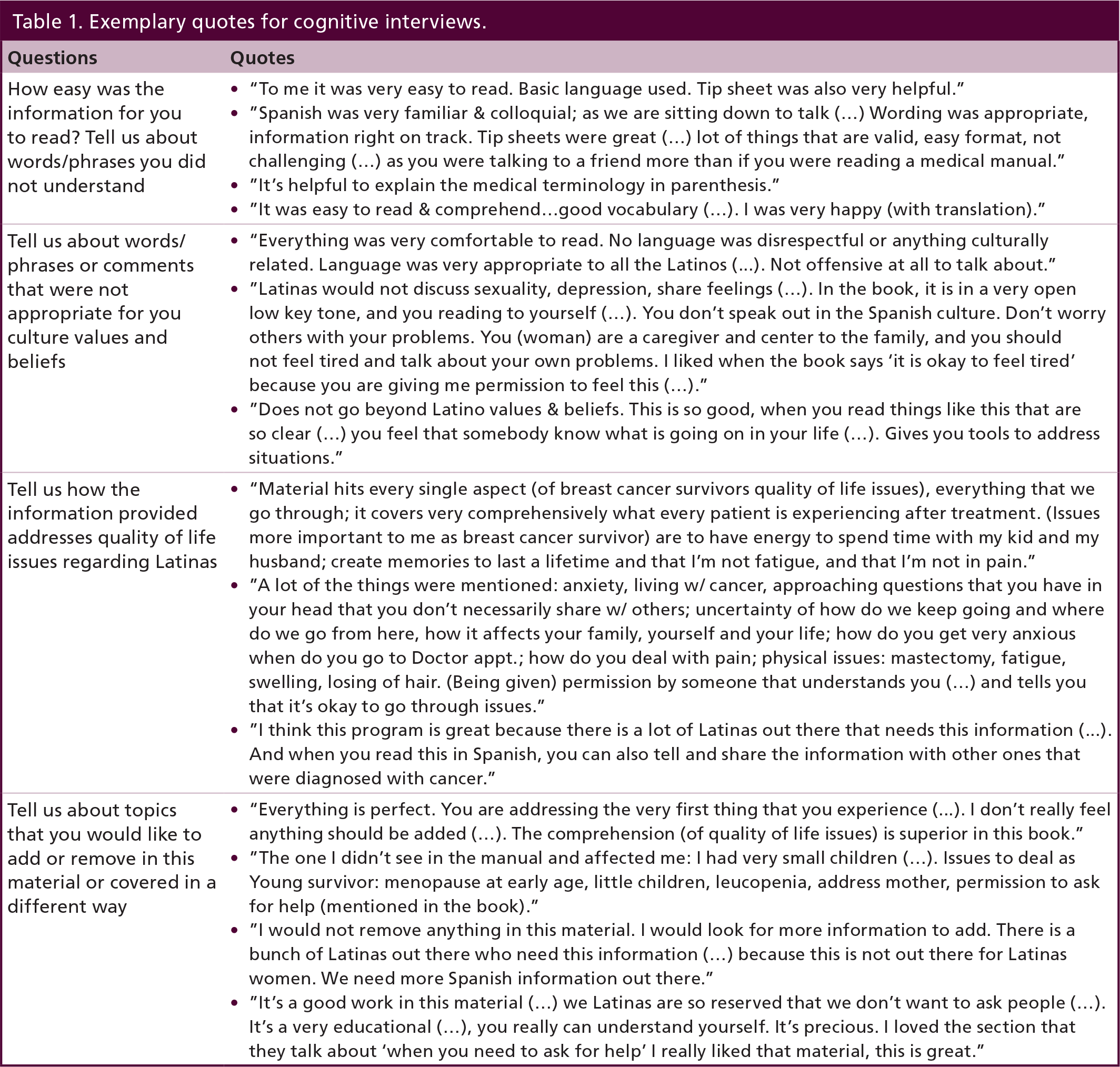
Cognitive interviews were transcribed verbatim and read line by line by one author (SG). Using thematic analysis [29], SG grouped similar phrases together. The grouped phrases were reviewed and discussed with two authors (K Menseses, P McNees). Similar content was grouped and three major themes were identified. Table 1 shows the questions, relevant quotes and the major themes.
Exemplary quotes for cognitive interviews.
Marianismo
Placing others before self, or the concept of marianismo, was the most salient cultural value discussed. The comment, “You don't bother others with your problems in the Spanish culture. You (woman) are a caregiver and center of the family, and you should not feel tired or talk about your own problems” was an important one, but the sentiment hinders women from openly discussing their personal experiences in survivorship. The participants commented that the objective and factual presentation of the side effects allowed them to ‘own’ the experience. For example, the quote: “I liked it when the book said ‘it's okay to feel tired’ because I am given permission to feel this way.” The experience of pain was another sensitive topic that participants indicated was not openly discussed among Latinos. Reading the information gave them the opportunity to talk about pain.
Participants were particularly pleased with the topic of sexuality prompting them to have candid discussions about sex and intimacy. For emotions such as anxiety and depression, one Latina stated that there were answers to “questions in your head, which you don't necessarily share with others.” Reading the information prompted them to accept help as a positive change. For example, as indicated in this comment, “Latinas see that if you ask for help, it is bothering people… here, everyone is offering help, but you need to change, give yourself permission to ask for help.”
Familismo
Participants stressed the primacy of family and family closeness, often called familismo. One said it was “more important for me to spend time with my kid and my husband” and the need for a “positive experience with family, time during chemo, and taking the opportunity to turn the focus into good.” They discussed concerns about children and the need to pay attention to the emotional impact of cancer on their children. They discussed concerns ranging from how to talk with little children about cancer, the impact of hair loss on children and the effect of hospitalization and separation anxiety of children. The women commented that the strategies to promote healthy personal lifestyle behaviors such as physical activity, nutrition and diet, were helpful not only for them, but their family. They gave practical suggestions to incorporate foods common to the Latino diet, for example, rice and beans, and soy as protein sources.
Personalismo
The importance of having a warm interpersonal relationship with their healthcare and oncology providers or personalismo was also valued [3,18]. However, they did not perceive that healthcare providers shared the value of personal interactions. They indicated that the information conveyed in the Spanish translation helped them “feel that somebody knows what is going on in their life.” They viewed the content as caring. For example, “You are happy that somebody tells you what is going on…somebody cares and understands.”
Overall, the participants believed the BCEi print materials provided two critical tools to address cancer survivor's needs. First, to recognize normalcy within the many changing physical and emotional issues, for example, participants agreed that they face so many physical issues including mastectomy, fatigue, swelling and hair loss. By having someone recognize their concerns as a normal process was a relief. The second tool was to develop a realistic attitude about their expectations. One summarized, “a lot of the things were mentioned regarding anxiety and living with cancer afterward. The uncertainty of how do we keep going…how it affects your family, yourself and your life… is very realistic and very on track.”
Readability
The sixth grade reading level of the Spanish version was consistent with the original English version. Overall, the women found the wording was basic, colloquial and understandable. They commented that the conversational style of the Spanish translation felt “more like talking to a friend [rather] than reading a medical manual.” They also made several valuable suggestions. The first was to add short explanations or phrases to enhance understanding about cancer survivorship because some words and terms had different meanings. Some specific cancer treatment or cancer survivorship terms were not well understood, so they suggested that synonyms and short explanations be added to enhance comprehension. For example, the common side effect word lymphedema (i.e., arm swelling) was translated as ‘linfedema’. However, this word was not readily understood by the participants. Thus, a short explanation or phrase ‘hinchazón de los brazos y manos’ was added in parenthesis after the word linfedema. These synonyms and short phrase suggestions were incorporated into the final Spanish print translation comprising 168 print pages.
Pilot evaluation
The Spanish translation print materials were evaluated with a pilot sample of LBCS who participated in a large parent survivorship intervention study conducted in the State of Florida. The parent study recruited Latina breast cancer survivors through the state's population-based cancer registry. Eligibility criteria for the parent study were women at least 21 years of age, diagnosed stage 0 to III breast cancer within the past 1–3 years. Recruitment was conducted via mail and those who were interested either contacted the study office via telephone or return postcard. Women with Spanish surnames who were identified through the cancer registry were sent recruitment information in both Spanish and English. Survivors who were interested contacted the study office for further information.
Sample & procedures
Forty LBCS enrolled in the pilot study with 30 completing the 12-month intervention. Thirty nine of the 40 participants were born in Latin and South America including Cuba (n = 10), Puerto Rico (n = 5), Colombia (n = 3), Costa Rica (n = 3), Honduras (n = 3), Venezuela (n = 2), Mexico (n = 2) and one participant each from Guatemala, Argentina, Panama, Peru and the Dominican Republic. One Latina was US born. 70% (n = 28) were between 46 and 64 years, 65% (n = 26) were married or living with a partner. 37% (n = 15) had at least high school education. 40% (n = 16) had family income of $20,000 or less. Spanish was the preferred language spoken at home for 82.5% (n = 33). About 37% (n = 15) were recent immigrants living 10 years or less in the USA.
The intervention comprised three telephone education sessions based on the Modules 1 & 2, Modules 3 & 4 and Module 5 & 6, as previously described in BCEi, followed by six telephone support sessions for a total of 12-month study participation. The intervention was delivered by trained bilingual nurse or physician interventionists via telephone. Each intervention took about an hour for delivery and each followup telephone call took about 30 min. All interventionists received training and education in breast cancer survivorship, principles of intervention research and core Latina values. For example, marianismo and familismo values were discussed during the telephone education sessions. Interventionists discussed that caring for oneself as a survivor helped support the ability to care for their family. All interventionists participated in mock interviews prior to the start of the study and learned that additional time may be needed to establish warmth and personal contact with LBCS, paying attention to personalismo.
After the end of 12-month study participation, LBCS were mailed a follow-up evaluation survey concerning the usefulness of the Spanish translation print materials and satisfaction with their interactions with the interventionists, along with a return self-address stamped envelope. The evaluation survey comprised an 8-item Likert questionnaire and a 12-item open-ended questionnaire developed by the authors and translated into Spanish. Because this component was an evaluation, no identifiers were included in the survey so the returned responses were anonymous. The Likert questionnaire assessed satisfaction with the educational materials. The open-ended questionnaire assessed cultural relevance of the print materials, and satisfaction with the telephone interaction with the interventionist.
Evaluation survey analysis & results
Fourteen LBCS returned the evaluation surveys via mail for a 47% response. Survey data were analyzed using IBM® SPSS® version 20 [30]. Descriptive analyses were completed for the 8-item questionnaire. The open-ended questionnaire data were analyzed by content analysis by an experienced coder (Y-M Schoenberger) [29]. Initially, Y-M Schoenberger read the questionnaire responses, identified and grouped similar content, and identified themes that emerged within each question. Y-M Schoenberger discussed the initial themes with two members of the research team (K Meneses and S Gisiger-Camata). Themes that were considered relevant had to be identified by a minimum of two participants. Interpretations were made, and relevant themes were finalized.
Questionnaire results
The results showed a high level of satisfaction with the Spanish print materials. All participants (n = 14, 100%) strongly agreed or agreed that the materials were easy to understand, addressed their quality of life issues and concerns and was helpful for making decisions. Nearly all participants (n = 13, 93%) strongly agreed or agreed that the materials helped them communicate concerns to their family or oncology team. A total of seven (59%) strongly agreed that the information was relevant to the Latina culture; eight participants (67%) strongly agreed that the information reflected their experiences as a Latina breast cancer survivor.
Open-ended questionnaire results The major themes identified in the open-ended questionnaire and exemplary quotes are summarized on Table 2. Overall, participants were satisfied with the intervention. Participants stated the intervention was informative and helpful, as in this quote: it was “interesting and very important to learn about the different symptoms, side effects and treatments for breast cancer; as well as side effects of some medications, and how our life is affected by being diagnosed and treated for breast cancer.” One participant stated “I believe that the information I received was very important because it helped me see that many of my feelings and symptoms are not imaginary.” Another participant stated “It was an excellent program with very good professional people that made me feel the support that I needed during this very difficult time because of my illness.”
Themes and exemplary quotes from Latina breast cancer survivor evaluation surveys.

The participants agreed that the program met expectations as in this quote: the program “completely met [expectations] since I believe it covers all the ranges of emotions and situations that survivors have to face.” Another stated, “Yes, it guided me and as I shared my experiences I learned more. I received advice/tips that I started following.” “Yes it met my expectations since I learned new things and all the telephone calls with [names of interventionists] were usually friendly and educational.” They also indicated that the number of educational appointments were sufficient to meet their needs for survivorship information. “All the information has been very helpful, since, after you complete the treatment you feel like you have been abandoned, and this program makes you feel useful.”
In response to how the participants were helped in a particular way by the program, the single most frequently mentioned response was that the one-on-one personal interaction with their interventionist who was supportive, compassionate and personal. One participant stated: “I received help with a lot of caring from Mrs. [interventionist]. If I didn't know the explanations, she was very good when she explained things to me. She gave me her friendship and made me feel like part of the family every time that she called me.” Another participant said, “Just the simple act of talking to someone about the subject is of great help. Also, the tips and the caring quality of the people that I spoke with were just exceptional. I felt in a way valued and appreciated and helpful to others, that my experiences could help others.” In addition, participants mentioned that the program helped them better understand their health after breast cancer treatment. For example: “For me in particular, I liked participating in the study because I got to speak and learn about a topic that affected me and I learned and received tips that I didn't know before.”
Overall, the survivors expressed satisfaction with support received from the interventionists. For example: “I feel very happy about participating in the program and satisfied with my nurse, she helped me during the hard times that I experienced until my husband passed away. At this time, I am at peace.” When asked whether they would recommend the program to a friend or relative who was a survivor, all participants indicated yes.
Discussion
This paper described a process by which an evidence-based cancer survivorship intervention originally developed for non-Hispanic White survivors was adapted and implemented in an effort to reach LBCS who experience survivorship disparities. There are several lessons learned. First, given the tremendous lack of Latina intervention studies, particularly in survivorship, adapting a known intervention can be used to improve reach to this underserved population. Since language and cultural values are well known barriers to effectively reaching Latinas, English to Spanish certified translation was a necessary first step to address cultural barriers.
Second, cognitive interviews with a small Latina sample provided valuable information to enhance or modify print materials prior to use in the intervention. Based on our experience, cognitive interview was preferred over backward translation. Cultural meanings were conveyed during the interviews which may likely have been ‘lost in translation’ if backward translation had been used. The impact of culturally embedded and valued concepts of marianismo and familismo was vital to transform the print materials into a culturally appropriate Latina intervention. Participant suggestions to improve familismo or family closeness could not have been achieved by translation alone.
Third, keeping readability at the sixth-grade reading level and eliciting participant suggestions about wording is a study strength. There is a marked absence of how other Latina investigators assess readability of their study instruments and teaching intervention materials [2]. Thus, this study adds to our knowledge of readability assessment of translated materials. Another study strength is the evaluation of satisfaction with the translation and cultural relevance among study participants. Only one prior study of Latinas by Juarez and colleagues [16] included such an assessment. Investigators in future studies of adapted interventions can consider this strategy to evaluate interventions.
Fourth, study findings affirmed three cultural values of personalismo in which Latinas placed on warmth and engagement during interactions with their interventionists. Cultural values of marianismo, and familismo were conveyed in the Spanish print materials. There are many other culturally based values of high importance to Latinas. Future investigators could identify which cultural values were either assessed or embedded in adapted interventions.
Limitations
Several limitations are noted. First, the authors recognize that implementing an intervention with a small pilot sample is considered a work in progress. In this light, this project represents a first step to develop and adapt this evidence-based intervention for other Latina groups. Second, while the evaluation summaries were entirely voluntary, about half of the participants in the pilot returned their surveys. Possibly, the 12-month long participation in the study contributed to subject fatigue. Thus, LBCS who were not as satisfied with the program may have been reluctant to document and submit their concerns. Even though half returned surveys, the quality improvement evaluation summaries were highly positive with several useful suggestions for changes in the future. Third, the authors recognize that were no Latina of Mexican heritage who participated in the cognitive interviews. However, the certified translator was of Mexican heritage, and two LBCS in the pilot study were Mexican. The Latina population of Florida is widely diverse with many Latin American countries represented throughout the state. While this population is considerably diverse, the mix and diversity is not representative of other states with larger or smaller Latina populations. Florida is also considered an ‘old settlement’ state with four or five generations of Latinas. Thus, its Latina citizens do not resemble other states, such as those in the South, that have a large new immigrant population. And finally, use of broadcast Spanish in this small study sample is a beginning reasonable attempt to address some of the idiomatic differences existing within the larger Latino population in the USA.
Conclusion
This small pilot study adds to our knowledge of adapting evidence-based interventions for LBCS. Given the scarcity of Latina interventions, this process is one that can be used to help reduce breast cancer survivorship disparities. Spanish translation and cognitive interviews attended to and embedded several important cultural and valued concepts. Pilot implementation of the Latina intervention was viewed highly positive by participants who responded to the surveys. Furthermore, the one-on-one interaction with the interventionist addressed the vital cultural need for provider support and personalismo.
Future perspective
The number of Latina breast cancer survivors will continue to increase in the USA. Latina breast cancer survivors experience disparities after end of treatment. It is critical that additional survivorship interventions be developed to address cultural acceptability of the interventions. While some interventions can be developed specifically for Latinas, evidence-based interventions can also be adapted for them. Translation and cognitive interviews are the first step to approach cultural relevance. Feasibility testing of current evidence-based interventions for cultural relevance is required to complete cultural acceptability. Patient-centered approaches to research that are inclusive of Latina breast cancer survivors are warranted.
Dislaimer
The views expressed herein are solely those of the author(s) and do not necessarily reflect those of the contractor or the Department of Health.
Financial & competing interests disclosure
This study was funded by grants from the National Cancer Institute, RO1CA-120638-07; and UAB Impact Funds. The Florida cancer incidence data used in this report were collected by the Florida Cancer Data System under contract with the Department of Health. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or anima experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Executive summary
Latina breast cancer survivors living in the USA experience survivorship disparities.
With the growing Latina cancer survivors population, there is increased need for Latina interventions.
Evidence-based interventions adapted for Latinas may be a viable option, but there are no reported descriptions of this process.
Certified translation is the first step in translation, but is insufficient to assess cultural relevance.
Cognitive interview can be used to assess cultural relevance.
Readability of study materials, satisfaction with intervention components are often overlooked in Latina intervention studies.
Follow-up evaluation to assess usefulness of interventions are needed.
Footnotes
Acknowledgements
The authors are indebted to Latina breast cancer survivors participating in this study.