
Abstract
In modern conformal radiotherapy with tight margins and steep dose gradients, such as intensity-modulated radiotherapy, it is essential that the position of the clinical target volume is precisely defined prior to each treatment fraction throughout the entire course of treatment.
Technical innovations have enabled the direct integration of various image verification methods into the treatment unit. In many cases this allows for patient and tumor monitoring and position correction. Nowadays, kV and MV planar radiographic imaging and volumetric cone beam computed tomography (CT) imaging are standard image verification systems in many radiotherapy centers. Generally, these systems are implemented as image-guided radiotherapy (IGRT) for daily target alignment, and thereby improving the precision of the radiotherapy treatment. However, one of the challenges of using these ionizing systems is insufficient soft tissue visualization (e.g., of the uterus of gynecologic [GYN] cancer patients or identification of the prostate gland and surrounding organs at risk [OAR] in prostate cancer patients). In some cases these systems require invasive methods, such as implanted fiducial markers in prostate radiotherapy. Therefore, different nonionizing 3D-ultrasound (US) systems, such as the Elekta 3D Clarity® Soft Tissue Visualization system (Elekta, Montreal, Canada) and the NOMOS B-mode Acquisition and Targeting ultrasound system (NOMOS Corporation, PA, USA) have been developed and introduced into radiotherapy [1–5]. The prostate and uterus, for which internal position variations are dependent on rectal and bladder filling, are ideal sites for US scans. However, different uncertainty factors in terms of probe handling, image quality and interoperator variability are present when using the US systems. Variations in the transducer probe pressure applied have previously been documented during 3D US on prostate patients [6,7].
The aim of the present study was to quantify the magnitude of probe pressure induced uncertainty using the Clarity US system on a commercial GYN phantom. An additional aim was to compare the pressure induced uncertainty with the overall interfractional variations by utilizing the US system on a healthy volunteer.
Materials & methods
A phantom was scanned by seven operators in four sessions on different days. Each operator performed two scans per session, one without pressure (WOP) or light probe pressure and one with maximum pressure (WP). All the US experienced operators were not presented in all sessions, thus, only a total of 42 scans were acquired. A healthy volunteer was scanned by the available Clarity operators in three sessions, leading to a total of 16 scans, over a period of 3 weeks (one session per week). Each operator participated in 2 weeks of intensive training provided by the manufacturer of Clarity, as well as several practice sessions before the start of the study.
Phantom
The US training phantom (Model CIRS 404) mimics the female pelvic region and contains a uterus, bladder and rectum representing the standard female pelvic organs (Figure 1A & B). The organs are subjected to displacement due to the exerted probe pressure. The phantom does not contain any skeletal structure, such as femur head or pelvic bone. The phantom is intended for US scans, thus all organs are easily defined in the acquired US images (Figure 1C). Initially, the phantom was marked with small spherical ball bearings (laser alignment markers), used to aid reproducibility of daily setup prior to each US scan session. During an initial session the best possible US scan was selected as position reference to the following four sessions.

Volunteer
The volunteer, a healthy young woman, was instructed to have an empty rectum and full bladder prior to each session. A moderately full bladder ensures better propagation of the US waves and hence a clearer US image by enhancing the image and sharpening the interface between bladder and uterus/cervix/vaginal canal. The fixation was in supine position by means of a Vac Fix fixation system to ensure position reproducibility between sessions. The volunteer was instructed to remain still throughout each session. Consistent positioning of the volunteer was enabled by the alignment of natural skin markers to the isocenter lasers of the CT room. A US transabdominal scan of the pelvic region was performed repeatedly by each operator until adequate image quality was achieved. During the first session the best scan, in which the organs were clearly definable, was selected as a reference for the following three sessions.
Clarity US system
The Clarity Soft Tissue Visualization system (Clarity Model 310C00) consists of two US units: one located in the CT simulation room and one in the treatment room. The two units are connected through a workstation/server. In this study all US scans were performed in the CT room. Since the objective of the ongoing project at Herlev Hospital is to implement the Clarity 3D US system for both GYN and prostate patients throughout the course of their treatment, the treatment room unit will be utilized only for daily IGRT.
Each US unit is equipped with a curve probe for transabdominal 3D US scanning. Each station consists of a ceiling-mounted infrared camera that can track the US probe by monitoring the infrared reflectors/emitters mounted on it (Figure 1E & F).
To enable superimposition of the acquired 3D US images and the reference US image, the 3D US system is calibrated to the same room coordinate system as the CT and treatment room, respectively. The calibration procedure is accomplished by means of an alignment phantom. Quality assurance checks confirm the system calibration on each day of use.
Image acquisition
The US image of the phantom (transabdominal US scan) was acquired by the seven experienced operators using the curve probe (Figure 1B). In each phantom scan the US probe was placed on the first occasion with minimal pressure and on the second with firm pressure in the region corresponding to the pubic symphysis and rotated, after which it was swept cranially. No firm pressure was applied on the volunteer, as the focus was on obtaining clear images, where the complex pelvic structure could be identified.
Organ delineation & data analysis
The uterus, bladder and rectum were delineated in the reconstructed 3D US image datasets using the Clarity workstation supplied by the manufacturer. In the workstation the delineation can be performed either manually or with aid of autosegmentation. In this study the assisted segmentation was utilized for all outlined organs. A single operator (MB) conducted a retrospective analysis of the acquired US image sets and delineated the organs for both the phantom and the volunteer.
Descriptive statistics and the paired sample t-test were employed to evaluate the statistical significance of the mean differences between probe pressure and no probe pressure. The p-value was calculated for a 95% CI, (i.e., the significance at α = 0.05).
Results
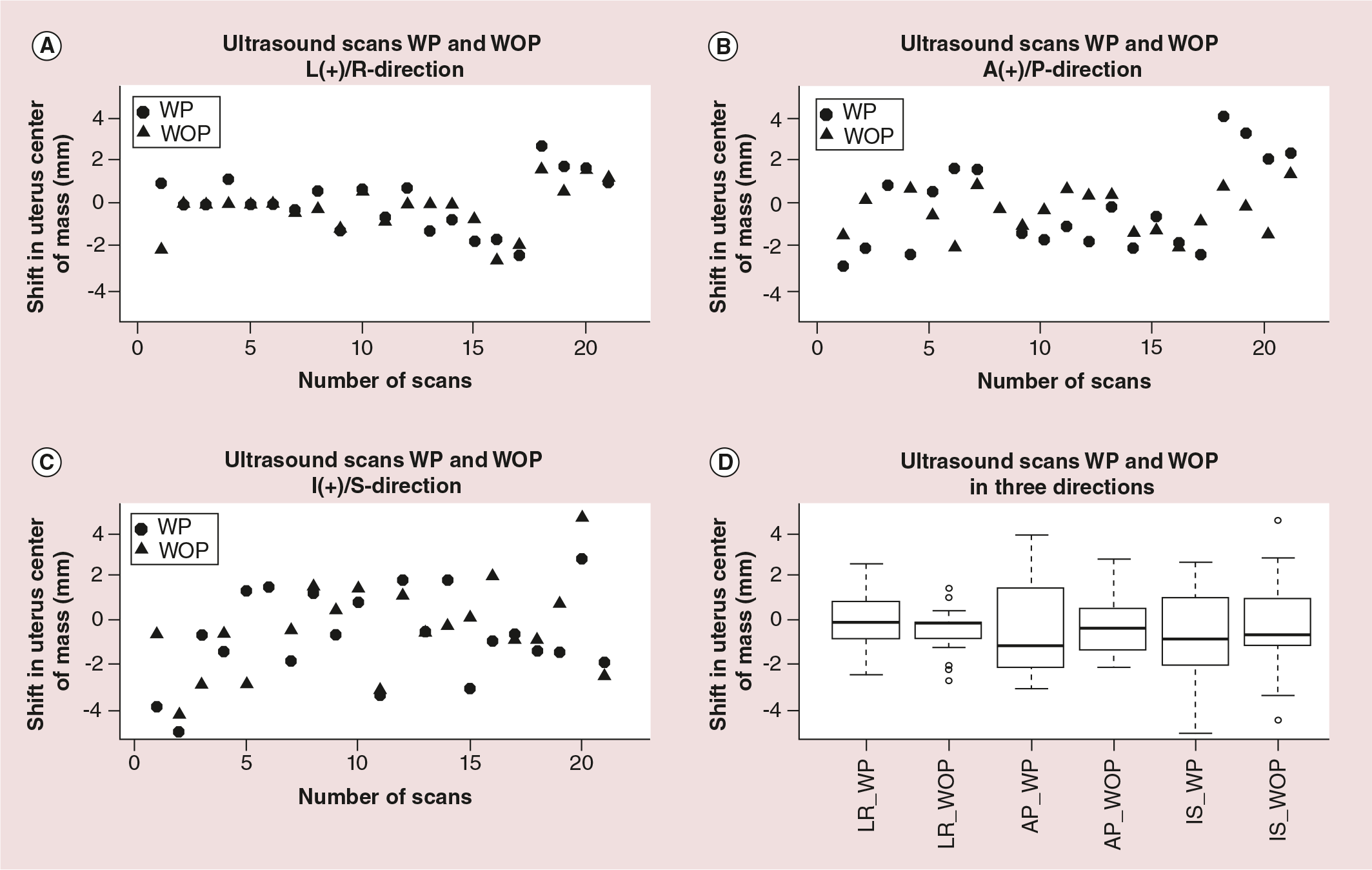
Positional shifts of the phantom uterus center of mass (COM) in the three orthogonal directions WP (depicted as circles) and WOP (triangles) are presented (Figure 2A–C). Positive shifts are left, anterior and inferior. Qualitatively, these plots demonstrate that there are no significant differences when comparing the shifts between WP and WOP.
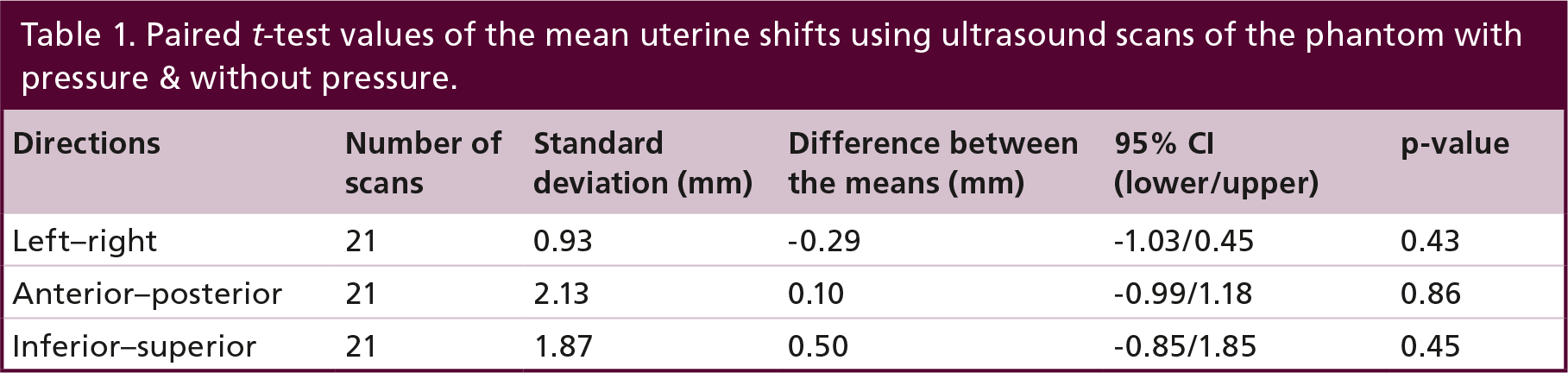
The overall mean (± 1 SD) of the phantom COM shifts are (mm); WP/WOP: LR (0.1 ± 1.2)/(−0.2 ± 1.1), AP (−0.3 ± 2.1)/(−0.2 ± 1.2) and IS (−0.8 ± 2.1)/(−0.3 ± 2.2). The largest recorded shift is observed in the I/S-direction; +5 mm (WOP) and −5 mm (WP). The mean of the COM shifts in all three directions (L/R, A/P, I/S) for WP and WOP are centered around zero (Figure 2D). The spread in the recorded shifts, (i.e., the standard deviations) for WP is larger than WOP in all directions. This is caused by larger interoperator variations while applying strong probe pressure. For each of the three directions a paired two sample t-test was utilized to test whether there are any statistical significant differences in the means of the shifts between WP and WOP. No statistical significant differences in any direction are observed (i.e., none of the p-values are below 0.05). The largest lower/upper 95% CI range was found in the I/S-direction (−0.85/–1.85) (Table 1).
Paired t-test values of the mean uterine shifts using ultrasound scans of the phantom with pressure & without pressure.
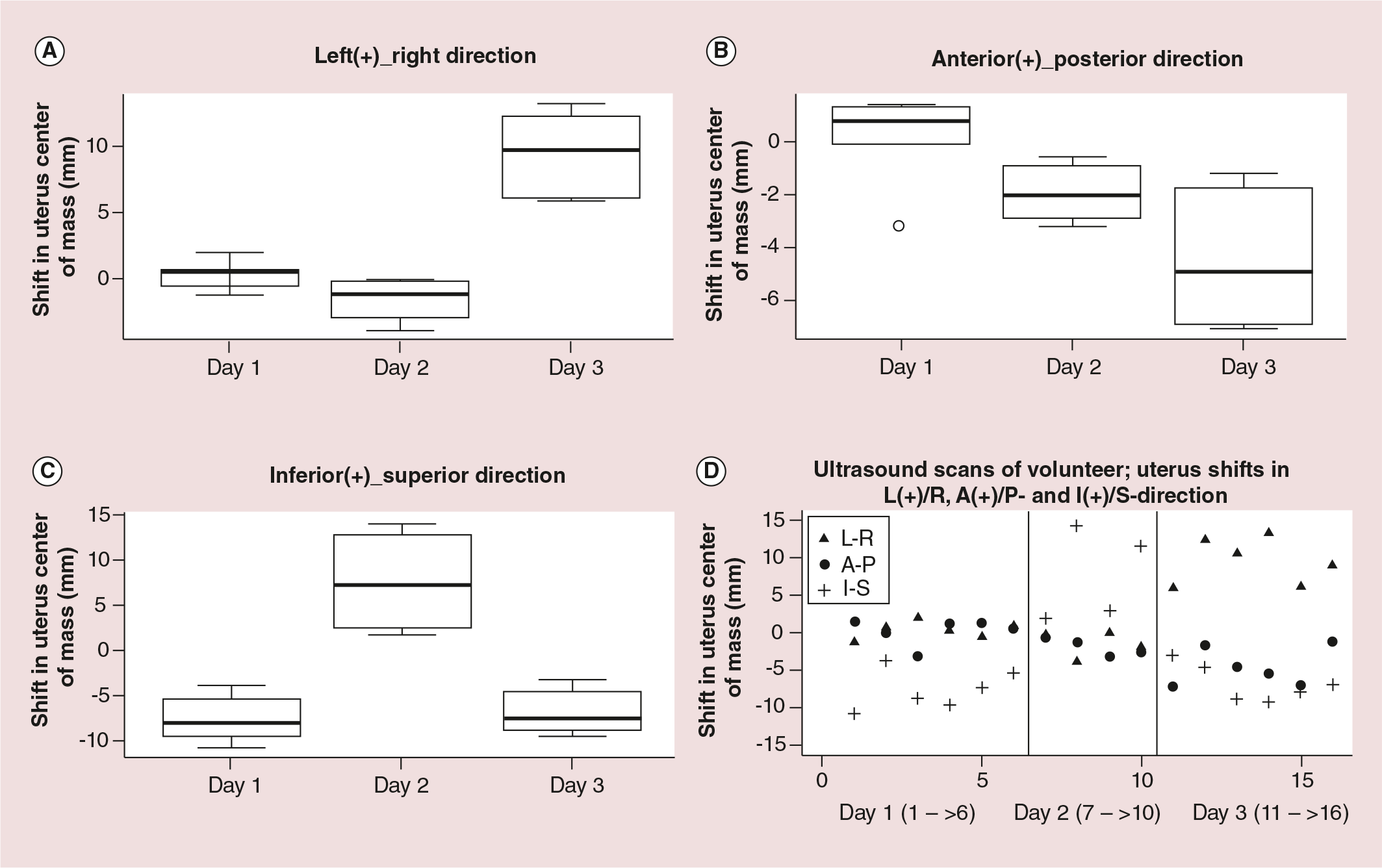
For the volunteer the recorded mean COM shift on day 3 in L/R direction is approximately 10 mm relative to the reference, while on days 1 and 2 the lateral shift is less than 2 mm (Figure 3). Furthermore, in the A/P direction the mean shifts are less than 2 mm on days 1 and 2, but more than 5 mm on day 3. The largest interfractional displacement is observed in the I/S direction, with a mean value of −7.7 mm, +7.6 mm and −6.9 mm on days 1, 2 and 3, respectively (Table 2). This clinically critical shift is visible in Figure 4. One can clearly see that the bladder is fuller on day 2 than on day 1, causing correlated uterine positional displacement. It is worth mentioning that on day 2 only four US scans (four operators) took place compared with six on days 1 and 3.
Mean values with standard deviations of the uterine shifts in the volunteer scanned by seven operators.


Discussion
Interfractional positional uncertainty of the uterus, rectum and bladder in GYN patients is a challenge in radiotherapy as it leads to the application of large planning target volume (PTV) margins. Previous reports have confirmed that uterine positional changes are strongly correlated with daily variation in bladder–rectum filling [8–10]. Thus, there is a need to incorporate IGRT methods into radiotherapy to identify and correct possible uterine and OAR positional changes. At present the 3D US IGRT method has mainly been used for prostate alignment prior to treatment [11–17]. Only a few published papers have reported the application of 3D US in GYN patients [18–20], and with the focus on quantifying interfractional bladder motion and variation in bladder volume rather than uterine positional change. For instance, in a US study of 24 cervical cancer patients, Ahmad et al. concluded that the mean bladder volume decreased dramatically by 71% compared with the treatment planning CT scan [18]. Herlev Hospital is a pioneer in the application of the Clarity 3D US system with a focus on GYN diagnoses. The present study started by applying Clarity on a phantom and a healthy volunteer and it will subsequently be tested for GYN patients at Herlev Hospital.
Different studies on the prostate have concluded that one of the drawbacks of using 3D US as the IGRT method is probe pressure-induced uncertainty of the target and OAR locations. However, to our knowledge, no specific probe pressure study on GYN patients has been published. In the present phantom study, we found no statistically significant differences in uterine COM shifts using pressure versus no pressure. All the acquired US scans indicated that uterine COM displacements were in the vicinity of zero, with a daily mean value of less than 1 mm in all three cardinal directions (L/R, A/P and I/S). Since the shifts of the bladder–uterus interface is interesting to study – as a portion of the bladder receives an undesirable high radiation dose owing to its proximity to the uterus – further studies focusing on the bladder–uterus interface are necessary. In an MRI study by Chan et al., the uterus was divided into three sections; cervical os, uterine canal and uterine fundus [21]. GYN patients underwent a pelvic MRI scan before treatment followed by weekly scans. The interfractional displacement was largest at the fundus, moderate along the canal and smallest at the cervical os. A similar study using 3D US is recommended to verify these findings. Our volunteer study revealed a clinically critical large interfractional displacement in all three directions. The largest uterine positional displacement was 15 mm in the I/S direction between days 1 and 2. Although our volunteer US scans are limited to three sessions, the result agrees well with a recent study by Jurgenliemk-Schultz et al., which investigated vaginal positional change and the correlation between vaginal shift and bladder–rectal filling [22]. These authors reported a vaginal clinical target volume positional change of up to 2.3 cm in the A/P direction. However, in contrast to previous studies, they did not find any correlation between vaginal positional displacement and bladder–rectal filling, except an extremely weak one in the case of A/P position shift and rectal filling.
The challenge experienced by most of our operators during 3D US acquisition was to find an appropriate probe handling technique that captured the entire uterus from the cervical os to the fundus, as the image quality was poor in some cases. Obviously, poor image quality has an adverse influence on uterine delineation, thus leading to uncertainty in COM shifts. This challenge is illustrated in the boxplots (Figure 3) and by the SD (Table 2) of the uterine COM shifts on day 2, which was more than 6 mm in the I/S direction. The plot in Figure 3D illustrates the large dispersion of COM shifts on day 2 in the I/S direction. Our experience of suboptimal image quality is confirmed by the study of Johnston et al., who compared assisted segmentation (employed in the present study) and manual segmentation of prostate patients using the Clarity 3D US system [23]. During quality classification of the acquired US images, they found that up to 33% were of bad quality, which hinders accurate outlining of the target.
Finally, it should be noted that the phantom used is not necessary representative of a real GYN patient, therefore a clinical study is needed to validate the results of this study. The daily bladder and rectal volume variations can strongly affect the position of the uterus, which cannot be simulated by our phantom. Furthermore, statistical evaluation of the interfractional uterine positional changes based on a single volunteer must be considered with caution, and a clinical study is needed to validate the present result.
Conclusion
The large daily uterine positional displacement of the volunteer outweighs the submillimeter impact of probe pressure in all directions. The difference in phantom uterine COM shifts using probe pressure versus no probe pressure is not statistically significant. Based on a single volunteer case, a large uncertainty in using 3D US on GYN patients is the poor quality of the acquired image due to the challenge of handling the probe. A clinical study is required to validate phantom probe pressure-induced uncertainty. The large interfractional variations based on a single volunteer warrant further investigation.
Future perspective
In radiotherapy, it is vital that the daily target alignment is correctly applied prior to each treatment. Today's widely used X-ray IGRT techniques are poor in terms of visualizing soft tissue in the female pelvic region and for this reason bone match instead of soft tissue match is employed. However, it has been previously demonstrated that uterine mobility relative to the bone structure can be several centimeters in all directions. In the present study we have shown daily uterine positional displacements of several centimeters using the novel Clarity US system. US is nonionizing, fast, inexpensive and good for visualizing soft tissue organs. Despite challenges in probe handling to obtain optimal images, the US is a good choice as a future IGRT system for cervical cancer patients.
Acknowledgements
Sincere thanks to our hardworking colleagues who helped to conduct this study; L Gullander (radiation therapist), SK Pedersen (radiation therapist), T Zarp (radiation therapist), S Jacobsson (radiation therapist), S Pazhang (radiographer) and VK Lynnerup (radiographer).
Executive summary
In radiotherapy it is important that the target is correctly aligned to the planned images on a daily basis.
This study quantifies the impact of ultrasound probe pressure on uterine displacement in a phantom and compares positional uncertainty with the daily uterine motion of a young healthy volunteer.
The phantom mimics the female pelvic region and incorporates organs that are at risk of probe pressure displacement.
To quantify the uterine positional uncertainty induced by ultrasound probe pressure on a phantom and determine the day-to-day uterine displacement of a young healthy volunteer.
A uterine phantom and a volunteer underwent ultrasound scans conducted by seven operators. The phantom mimics the female pelvic region and is easily defined in ultrasound scans. A total of 42 phantom scans, 21 with light probe pressure (without pressure) and 21 using strong probe pressure (with pressure) and 16 volunteer scans were performed. Shifts in the uterine center of mass relative to the reference volumes were measured in three directions; left-right (LR), anterior-posterior (AP) and inferior-superior (IS).
For the phantom the difference between with pressure and without pressure was not statistically significant (p > 0.43 for each cardinal direction). The mean (±1 SD) of the daily center of mass displacements of the uterine position in the volunteer, as recorded by the seven observers, were (mm); LR: day 1 (0.3 ± 1.1), day 2 (–1.6 ± 1.7), day 3 (9.5 ± 3.1), AP: day 1 (0.2 ± 1.7), day 2 (–2 ± 1.2), day 3 (–4.5 ± 2.5) and IS: day 1 (–7.7 ± 2.6), day 2 (7.6 ± 6.1), day 3 (–6.5 ± 2.5), respectively.
The study reveals no significant shifts in any direction using light or strong probe pressure.
The larger daily uterine positional displacement in all directions in the volunteer outweighs the submillimeter displacement due to the probe pressure. A clinical study is required to validate the phantom probe pressure-induced uncertainty. The large interfractional variations based on a single volunteer warrant further investigation.
Footnotes
The current study is a part of a 3 year PhD research project at Herlev Hospital that is funded by Elekta, Inc. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.