
Abstract
Stroke is a major cause of death and disability in adults worldwide. Prevention focused on modifiable risk factors, such as hypertension and hyperlipidemia, has shown them to be of significant importance in decreasing the risk of stroke. Multiple studies have brought to light the differences between men and women with regards to stroke and these risk factors. Women have a higher prevalence of stroke, mortality and disability and it has been shown that preventive and treatment options are not as comprehensive for women. Hence, it is of great necessity to evaluate and summarize the differences in gender and stroke risk factors in order to target disparities and optimize prevention, especially because women have a higher lifetime risk of stroke. The purpose of this review is to summarize sex differences in the prevalence of hypertension and hyperlipidemia. In addition, we will review the sex differences in stroke prevention effectiveness and adherence to blood pressure and cholesterol medications, and suggest future directions for research to reduce the burden of stroke in women.
Stroke is the fourth leading cause of death in the USA, after heart disease, cancer and chronic lower respiratory disease, and the most common cause of permanent disability in adults worldwide [1]. Statistics from the American Heart Association (AHA) Heart Disease and Stroke 2014 updates shows that the relative rate of stroke death fell by 35.8% and the actual number of stroke deaths declined by 22.8% from 2000 to 2010. Yet each year, 795,000 new or recurrent strokes occur in the USA with approximately 610,000 first attacks and 185,000 recurrent attacks. One of every 19 deaths in the USA is due to stroke. On average, every 40 s, someone in USA has a stroke and dies of one approximately every 4 min [1].
Hypercholesterolemia and hypertension are well-established risk factors for stroke, they are modifiable, and thus are a major focus of stroke prevention [2]. The identification of patients who may be targeted for prevention with lifestyle changes is also well established [3]. In addition, the AHA has identified total cholesterol less than 200 mg/dl (untreated) and untreated blood pressure (BP) less than 120/<80 mm Hg for adults as two of the seven components of ideal cardiovascular health [4]. According to 2014 AHA statistics, 77% of patients with first-time stroke have BPs greater than 140/90 [1].
Elevated total cholesterol levels are also a major focus of prevention programs because nearly 32 million adults over 20 years of age have total cholesterol levels greater than 240, for a prevalence of 13.8% [1]. In addition, 33.0% of US adults, or approximately 78 million people over 20 years of age, have hypertension. Unfortunately, this is a major public health problem because although nearly 82% of people with hypertension are aware of their condition, a smaller fraction (75%) are using antihypertensive medication; but more important, only 53% of those with hypertension are controlled to target levels [1]. Statistics for these risk factors are even worse in developing countries compared with developed countries. Although patients are prescribed medications for these conditions, they are not effectively treated, so the numbers of patients who reach treatment goals in developing countries are lower compared with the USAA and Europe [5].
Considering there are 795,000 strokes per year in the USA and that hypertension has a 49% population attributable risk for stroke, approximately 390,000 strokes could be prevented with adequate BP control. For cholesterol, an estimated 168,000 strokes could be prevented if adequately treated [2,6]. Hypertension and hyperlipidemia account for a very large proportion of preventable strokes in men and women.
In this review, we performed a literature search using Medline for articles focused on sex differences in hypertension and hyperlipidemia in relationship to primary and secondary stroke prevention. We also included carotid atherosclerosis as an intermediate outcome for stroke because hypertension and hyperlipidemia are major contributors to carotid disease. We selected cohort studies of both sexes and those with women only if BP and cholesterol were the focus. Also, clinical trials were included if they included the topics of interest, but we excluded case reports. Only studies with stroke or carotid atherosclerosis as outcomes were included.
Sex differences in stroke: outcomes
There are increasingly recognizable differences in various aspects of stroke outcomes between women and men. Nearly 55,000 more women than men suffer from stroke each year [1]. This is in part because women have a higher lifetime risk of stroke. Shown by the Framingham Heart Study, for people between the ages of 55 and 75 years, the lifetime risk of stroke was one out of five for women and one out of six for men [7]. Women, have a lower incidence of stroke than men between the ages of 45 to 84 years, but after the age of 85 years, the incidence in women is similar to, or exceeds that of men [8]. Women not only have a higher lifetime risk of stroke, but of those who die from stroke, women comprise nearly 60% [1]. Younger women are also at risk for worse outcomes than men [9].
Sex differences in hyperlipidemia & hypertension
In the USA, the National Health and Nutrition Evaluation Survey (NHANES) data shows that prevalence of hypertension increases in women, particularly in midlife. Specifically, men are more likely to have hypertension below the age of 45 years, between the ages of 45 to 64 years this prevalence is similar and after the 65 years of age hypertension is more common in women [1]. For hyperlipidemia in adults over the age of 20 years, women have a higher prevalence of total cholesterol greater than 200 mg/dl (44.9% vs 41.3% in men), but men have a higher prevalence of low-density lipoprotein (LDL) greater than 130 mg/dl (31.9% vs 30.0% in women) and high-density lipoprotein (HDL) less than 40 mg/dl (31.8% vs 12.3% in women) [1], suggesting a worse overall pattern of cholesterol in men than women.
Sex differences in primary prevention of stroke
Baseline sex differences in BP and cholesterol levels were noted in the Management of Elevated Cholesterol in the primary prevention Group of Adult Japanese (MEGA), which evaluated the usefulness of pravastatin in primary prevention of cardiovascular events [10]. This prospective, randomized, open, blinded end point study was conducted between 1994 and 2004, evaluating 7,832 patients (women: 5356, 68.4%) between the ages of 40 and 70 years with hypercholesterolemia and no history of coronary heart disease (CHD) or stroke. The aim was to compare the effects of pravastatin plus diet on the incidence of cardiovascular events compared with diet alone, with a special emphasis on the outcomes in women. The comparison of baseline characteristics between men and women enrolled in this study showed that more women (42.6%) than men (40.2%) had hypertension (Table 1). Baseline triglycerides were higher in men, but HDL-cholesterol (HDL-C) was higher in women and total cholesterol and LDL-C were similar [10].
Baseline characteristic of participants of Management of Elevated Cholesterol in the primary prevention Group of Adult Japanese (MEGA) study.

DBP: Diastolic blood pressure; HDL-C: High-density lipoprotein-cholesterol; LDL-C: Low-density lipoprotein-cholesterol; SBP: Systolic blood pressure.
Adapted with permission from [10].
There was no significant difference between diet plus pravastatin versus diet alone in prevention of stroke events in men or women and, thus, no sex difference in the treatment impact. However, men had a trend towards benefit in diet plus pravastatin for CHD protection, whereas women had no significant benefit (Table 2) [10].
Incidence of end points in the MEGA study stratified by sex
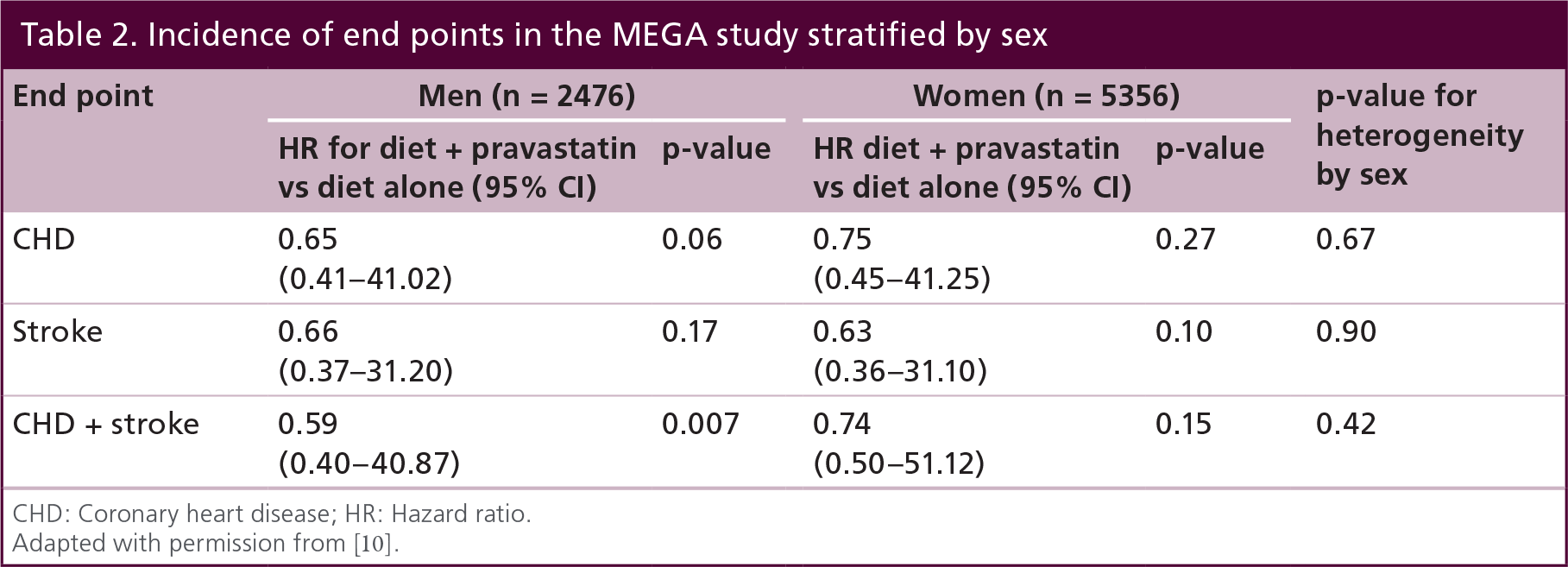
CHD: Coronary heart disease; HR: Hazard ratio.
Adapted with permission from [10].
The Asia Pacific Cohort Studies Collaboration, which includes 29 cohorts from Asia and 7 cohorts from Australia and New Zealand, assessed the joint effects of blood pressure and cholesterol on the risk of stroke, both ischemic and hemorrhagic subtypes. The investigators found that the slope of stroke risk jointly impacted by the various strata of cholesterol and systolic BP was similar in men and women [11]. Another analysis of 214,032 women in the same cohort assessed the impact of various risk factors on stroke risk. They reported that for every extra 10 mmHg increase in systolic BP, the risk of ischemic stroke increased by 36%, even after adjustment for other risk factors [12]. For total cholesterol, there was a 12% increased risk for each 1 mmol/l increase. These results emphasize the impact that improved risk factor management could have on stroke risk in Asia and Australia/New Zealand.
Sex differences in risk factor profiles of stroke patients
Cohort studies have pointed out the difference between risk factor profiles in men and women who have suffered a stroke [13–15], although the results from these studies are very inconsistent and differ greatly between countries [16]. In a meta-analysis done specifically to focus on sex differences in stroke and risk factors, 45 articles with data from 673,935 patients were reviewed [17]. The cumulative analysis showed that women, on average, were 5.2 years older than men at the onset of stroke (p < 0.001). Hypertension was more prevalent in women (69% vs 65% in men) and hyperlipidemia was more common in men (37% vs 34% in women; Table 3). Subgroup analysis showed there was some geographic variation. For example, hyperlipidemia was more common in men than women in North America (odds ratio [OR]: 0.87, 95% CI: 0.78–70.98; p = 0.02) but this difference was not observed in Europe (OR: 0.95, 95% CI: 0.78–71.14; p = 0.56) [17]. A cohort study from Australia with data obtained from the late 1990s noted that women were less often taking lipid-lowering therapy on presentation with a stroke, but this difference was attenuated when adjusted for age, history of cardiovascular disease and other medical and sociodemographic factors [18].
Meta-analysis evaluating risk factor differences between men and women with ischemic stroke.
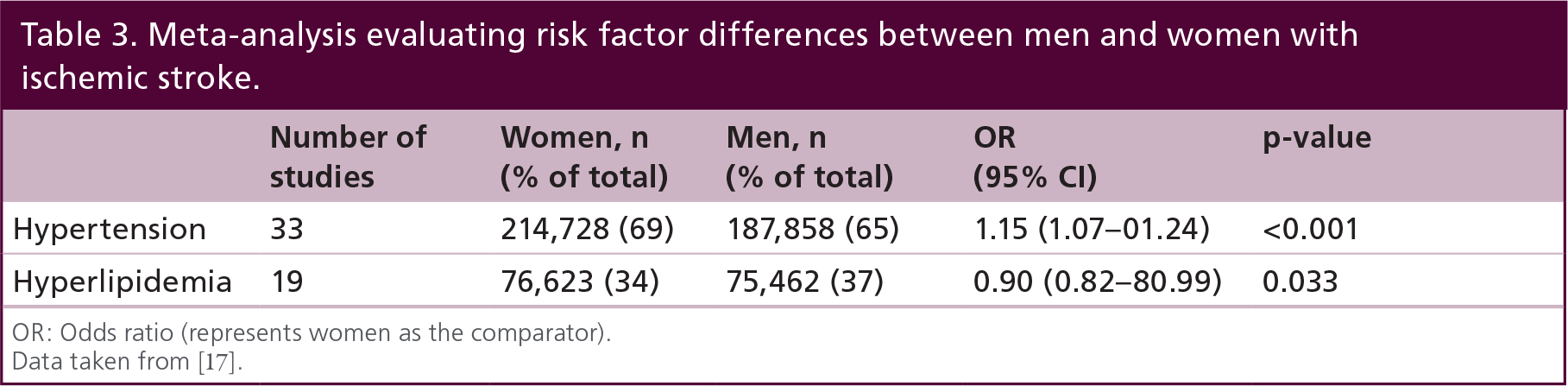
OR: Odds ratio (represents women as the comparator).
Data taken from [17].
Sex differences in younger stroke patients have also been documented. An Israeli study of men and women with stroke between the ages of 45 and 65 years showed that women were more likely to have diabetes, hypertension and hypercholesterolemia (29%) than men (14%), whereas men were more likely to have ischemic heart disease, smoking and alcohol consumption [19].
A study from Korea also evaluated gender differences in risk factors in 9,417 patients with ischemic stroke (42% women) admitted to 11 participating hospitals [20]. The aim of the analysis in this large cohort was to use statistical techniques to better understand the impact that age strata have on the sex differences among stroke risk factors. As expected, the mean age at stroke onset in women was approximately 6 years older than men. A number of risk factors were more prevalent in women versus men, specifically hypertension (64.1% in men and 71.0% in women) and hyperlipidemia (26.0% in men and 32.3% in women). When the prevalence ratios (men to women) were assessed by age strata, hypertension was more prevalent in men with stroke until 55 years of age, after which hypertension was more prevalent in women (p < 0.001; Table 4). Although the prevalence of hyperlipidemia decreased in both sexes with increasing age, this was still higher in women than men older than age 45 years and throughout the continuum of the age strata. When adjusted for age strata and other risk factors, only hyperlipidemia remained significantly more prevalent in women versus men. As for hypertension, the sex difference was no longer significant after BMI was added as a covariate [20]. These data are different from the meta-analysis, which suggested that cumulatively, hyperlipidemia appeared to be more common in men [17]. One could speculate that the Korean study illustrates unique geographic differences or differences in the criteria for hyperlipidemia from other studies.
Prevalence of hypertension and hyperlipidemia between male and females in Korean ischemic stroke patients, stratified by age.

adj: Adjusted for diabetes, atrial fibrillation, prior stroke, prior CHD, BMI, smoking, residence and education; unadj: Unadjusted p-value for prevalence ratio of men to women by age strata.
Data taken from [20].
Menopause & stroke risk factors in women
Hypertension and hyperlipidemia as classified in guidelines were assessed in a multiethnic cohort of women undergoing the menopausal transition (Study of Women's Health Across the Nation [SWAN]) [21]. Evaluation of lipid profiles of 1,349 women followed in this cohort showed that Chinese and Japanese women had the highest mean HDL levels and Hispanic women had the lowest mean HDL level (Table 5). Among all participants, 15% had LDL levels above the National Cholesterol Education Program's Adult Treatment Panel (ATP) III goals [22], with 9.5% requiring lifestyle modification, whereas 5.8% met criteria for additional drug therapy. In total, 9% of African–American and 6.6% of Hispanic women met criteria for drug therapy secondary to highest levels of LDL-cholesterol (LDL-C) and additional risk factors or history of CHD/Framingham 10-year risk greater than 20%, followed by 4.7% of Caucasian, 2% of Japanese and 0% of Chinese women [21]. The most recently published American College of Cardiology/AHA cholesterol treatment guidelines [23] focused on prevention of atherosclerotic cardiovascular disease (ASCVD) and do not specify a target, and they use a different ASCVD risk calculator, so it is unclear how the SWAN cohort results would be applied in terms of treatment.
Baseline characteristics of women participating in SWAN study by ethnic group.

DBP: Diastolic blood pressure; HDL-C: High density lipoprotein cholesterol; LDL-C: Low-density lipoprotein cholesterol; SBP: Systolic blood pressure.
Adapted with permission from [21].
Since the prevalence of hypertension in women increases in midlife and begins to exceed that of men, it is important to also evaluate BP in the menopausal transition. The SWAN investigators applied the criteria for the Joint National Committee (JNC-7) [24] for blood pressure to 1,460 participants in SWAN. They found that BP was highest among African–American (systolic BP [SBP] 125.2 mmHg) and Hispanic women (SBP 121.7 mmHg; Table 5). The rate of untreated hypertension among all participants was 9.1%. Unfortunately, the highest rate of untreated hypertension and lowest rate of control with medication was also among African–American and Hispanic women, whereas the lowest rate of untreated hypertension and highest rate of control with antihypertensive treatment was among Chinese and Japanese women [21].
Differentiating the impact of age versus the menopause (i.e., the physiologic hormonal changes) on hypertension and hyperlipidemia is important as women experience this midlife transition. As part of the SWAN, the investigators evaluated changes in CHD risk factors in 1,054 women during their transition to their final menstrual period (FMP) [25]. They divided the longitudinal transition into three segments: more than 12 months before the FMP; within 12 months before and after the FMP (corresponding to the decrease in follicle stimulating hormone or FSH); and, more than 12 months after the FMP. Using the slope of the changes in each risk factor during each of these timeframes allowed the investigators to determine whether the risk factor change slope was steepest during one of the phases or was linear across all three timeframes. Analyzing the slopes of change in risk factors during the year immediately before and after the FMP would suggest this occurred because of menopause rather than age alone. Results of this study showed that there was a significant increase in LDL-C and total cholesterol within a year of the FMP [25]. HDL-C showed a steady increase with peak at FMP and then declined after and plateaued during the transition to menopause. Interestingly, there was no difference between changes in lipid profile and ethnicity among participants in this study.
Another important finding was that changes in systolic and diastolic BP and other risk factors (glucose, insulin, lipoprotein(a), C reactive protein, Factor VII-c) were linear across all three timeframes, and therefore likely to be a function of age rather than the menopausal transition.
The recognition of modifiable risk factors in women, such as hypertension and hyperlipidemia, is increasingly important, especially in midlife. As described in this review, the prevalence of hyperlipidemia increases in women after menopause and hypertension increases after midlife due to aging. Recognition of these risk factors early, and the initiation of healthy lifestyle practices before or during the perimenopausal timeframe, could improve cardiovascular risk profiles [26], potentially reduce the need for cholesterol- and BP-lowering drugs, and provide the long-term benefit of reducing the risk of stroke and cardiovascular disease [3].
Sex differences in intermediate outcomes of stroke: carotid artery atherosclerosis
Subclinical detection of stroke risk can be performed with ultrasound through measurement of carotid intimal media thickness (CIMT) or with clinical ultrasound to detect stenosis or plaque size. Since BP and cholesterol are major factors in the progression of carotid disease, this review includes the sex differences in this intermediate outcome because of its importance in stroke risk identification [27,28].
Carotid atherosclerosis manifested in stenosis greater than 60–70% stenosis is associated with a risk of ischemic stroke [27]. Based on multiple clinical trials of carotid endarterectomy (CEA) for symptomatic or asymptomatic stenosis, the procedure is recommended if the surgical risk is appropriately low [28].
However, there are significant differences in benefit from CEA in men and women, especially in asymptomatic carotid stenosis. A Cochrane Systematic Review from 2005 reported the stroke relative risk (RR) reduction after CEA for asymptomatic carotid stenosis was 51% for men (RR: 0.49, 95% CI: 0.36–30.66) versus 4% for women (RR: 0.96, 95% CI: 0.64–61.44; p = 0.008), suggesting it was more beneficial for men [29]. There are many theories as to why women do not benefit as much or do worse after CEA for asymptomatic stenosis. Women have smaller arteries, have higher surgical risk, and may have more embolic phenomenon during the surgery [30].
Another potential explanation for the sex differences in benefit from CEA for asymptomatic carotid stenosis is based on the differing morphology of carotid plaques. For example, Ota et al. evaluated sex differences in carotid plaque with 3.0 Tesla MRI in 131 patients (64 women) with asymptomatic moderate or severe carotid stenosis (50–99%) [31]. There were no sex differences in the prevalence of hypertension or hyperlipidemia at baseline. The imaging results showed a higher odds of thin/ruptured caps (OR: 4.41, 95% CI: 1.97–99.87; p < 0.01), lipid-rich/necrotic core (OR: 3.66, 95% CI: 1.67–68.00; p = 0.01) and a trend toward hemorrhage (OR: 2.15, 95% CI:0.93–94.98; p = 0.07) in men compared with women, after adjustment for stain use or MR angiographic degree of stenosis [31]. Similarly, Hellings et al. evaluated 450 patients undergoing CEA, and demonstrated that men had higher rates of unstable plaque with more inflammatory features, for example, higher concentration of fat, higher number of macrophages and higher levels of IL-8 and matrix metalloproteinase (MMP)-8 activity [32]. This was regardless of the types of symptoms attributed to the carotid (amaurosis fugax, hemispheric transient ischemic attack or ischemic stroke) or the cardiovascular risk profile [32].
In another study looking at sex-related differences in carotid plaque features and inflammation, 457 carotid plaques from 132 women and 325 men obtained with CEA from symptomatic and asymptomatic patients confirmed gender-related differences in pathology of the plaques [33]. Although in this study women had higher prevalence of hypertension (67.0% vs 53.1% in men; p = 0.023) and hypercholesterolemia (67.4% vs 56.3%; p = 0.028), they had a lower prevalence of thrombotic plaque and smaller area of necrotic core and hemorrhage. Men had more complex plaques with higher rates of ulceration and erosion compared with women with more stable fibrocalcific plaques. However, gender was no longer significantly associated with plaque features in the multivariable model when cardiovascular risk factors, baseline stenosis severity and symptom status were included [33].
Sex differences in the development of atherosclerosis have also been described. For example, CIMT obtained using standard ultrasound protocols was evaluated in 17 men and 35 women between the ages of 45 and 64 years who had at least one stroke risk factor (tobacco smoking, hypertension, hyperlipidemia or noninsulin-dependent diabetes) [34]. In whole blood, gene expression analysis was performed on hybridized RNA, and correlations between increasing CIMT as measured with standardized ultrasound methods and up- or downregulation of genes were compared. The main findings were that the expression of hundreds of genes correlated with CIMT that were unique to each sex, that there were genes that showed similar correlation patterns in men and women, but that there were also genes that correlated with CIMT in opposite directions [34]. Several of the genes with opposite correlation were associated with or regulated by estrogen. Other pathways include inflammation, such as IL-8, thrombin and endothelin-1 signaling, all of which are important in vascular diseases [34]. Although this study is small, lacked statistical correction for multiple comparisons and does not demonstrate cause and effect based on stroke events, it is a descriptive study showing that there are pathophysiologic sex differences in the development of atherosclerosis in a middle-aged cohort with risk factors for stroke. Therefore, further research and validation of these findings in a larger, adequately powered cohort are needed.
Sex differences in stroke prevention & adherence to prevention therapies
Guidelines recommend medications for treatment of hypertension and hyperlipidemia to reduce the risk of recurrent stroke, that is, secondary prevention [35]. For example, the Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) study evaluated the effect of atorvastatin 80 mg/day on reduction of fatal and nonfatal stroke. It showed that participants randomized to the treatment group had a 16% reduction in stroke events compared with the placebo group [36]. A post hoc study used the same participants to evaluate any possible sex differences in the end points of this trial. The baseline characteristics and incidence of stroke (fatal and nonfatal) were compared between men and women [37]. Results showed that men were younger (62.0 + 0.21 vs 63.9 + 0.27), had lower SBP (138.1 + 0.35 vs 139.5 + 0.47), higher diastolic BP (82.2 + 0.20 vs 81.0 + 0.25), lower mean LDL-C (132.4 + 0.44 vs 134.4 + 0.57, p = 0.986), lower mean HDL-C (46.1+0.21 vs 55.8 + 0.34, p = 0.126) and lower total cholesterol (207.0 + 0.54 vs 218.9 + 0.67, p = 0.452) compared with women in their baseline characteristics. When end point results were compared, there was no significant difference between men and women in regards to stroke events and treatment-associated benefit was similar, emphasizing the importance of treatment in both men and women regardless of their baseline characteristics [37].
A meta-analysis of BP-lowering clinical trials showed that women received a similar benefit in reduction of stroke from antihypertensives as men, across all classes of these drugs [38]. A separate Cochrane review of over 26,000 women showed that black women may receive more benefit than white women. For example there was a 53% reduction in the risk of fatal and nonfatal cerebrovascular events in black women, whereas women overall had a 38% reduction of these events with BP lowering [39]. Although there have been some studies showing differences in the prescribed antihypertensive medications between men and women, there are no studies that definitively show a difference in response to BP medications. Therefore, control of BP, rather than the pharmacological approach, remains the goal for prevention of stroke in both men and women equally [8].
Nonadherence to cardiovascular medications in people with heart disease is associated with an increased risk for stroke [40]. Therefore, adherence to medications for hyperlipidemia and hypertension is very important in the management of these risk factors and ultimately stroke prevention. Gender has also been assessed as a factor that can influence medication adherence. Results of a study evaluating self-reported intentional and unintentional nonadherence and difference between male and female users, showed a total of 66.4% nonadherence among all participants with 67% in the female group and 65.4% in the male group [41]. Women had higher rates of intentional and combined (intentional and unintentional) nonadherence (n = 1151 women 67% vs n = 709 men 65.4%), and lower rates of unintentional nonadherence (women 49% vs men 51.8%) compared with men, but these results were only significant (p < 0.01) in the 55–64 years age group. Overall, unintentional nonadherence was the most frequent nonadherence behavior for both sexes. Among the reasons for nonadherence, forgetting to take medication (unintentional) is the most commonly reported in both genders and also more common in men than women. Women had higher rates of filling their prescriptions but not taking them, whereas men had higher rates of changing their medication doses [41]. In regards to self-discontinuation of medication, men had higher rates in the age group of 35–44 years, whereas women had higher rates in the age group of 45–54 years. There was no significant difference between men and women in relation to discontinuation of medication. Development of adverse reactions, another reason for medication nonadherence, was also reported by women more than men [41].
Adherence is also extremely important in patients who have suffered a stroke, since evidence-based recommendations include medications for secondary prevention. A study from Sweden tracked the use of stroke prevention medications in over 24,000 patients for 1 year after discharge from acute stroke [42]. In the multivariable model, men were less likely to be persistent with antihypertensive and antiplatelet drugs, there was no gender difference with warfarin and there was a trend toward lower persistence with statins in men. Other important factors associated with lower persistence included not receiving stroke unit care, having a recurrent stroke, low mood and poor perceived health status [42]. The Adherence Evaluation After Ischemic Stroke-Longitudinal (AVAIL) study assessed medication regimen persistence at 3 months and 12 months after stroke discharge. The persistent use of medications at 3 months was 76% [43] and 65.9% at 1 year [44]. There were no significant differences in men and women with medication persistence, although marital status was an important factor in maintaining medications when the analysis focused on self-discontinuation by 1 year [44].
Overall, prevention treatments with BP-lowering and cholesterol-lowering medications are key strategies for decreasing stroke risk in both men and women. However, nonadherence is common and should always be considered when evaluating patients with poor outcome, such as a first-ever or recurrent stroke. Since patients with stroke may not be recognized as having hypertension and hyperlipidemia until after the first stroke, new medications for prevention will be initiated at that time. The AVAIL study showed that patients who did not know why they were taking medication, how to take them and how to refill them were at high risk for nonadherence [43]. Therefore, counseling and education about medications, reminder systems and pill boxes could potentially improve adherence to treatment regimens and subsequently optimize prevention effectiveness in both men and women.
Conclusion
Despite substantial progress in the treatment of acute ischemic stroke, ultimately, prevention will be more effective than acute interventions to reduce the burden of stroke. The higher lifetime risk of stroke and the prevalence of major vascular risk factors in elderly women in those who have experienced a stroke indicate that we need to redouble our efforts to prevent or treat these factors in women. There are major variations in the gender differences in these risk factors, which also varies by geographic region. In addition, when assessing these risk factors in stroke patients, age likely plays a significant role, especially in hyperlipidemia. In addition, hyperlipidemia appears to be the risk factor most influenced by menopause as opposed to age alone. The major impact of hypertension and hyperlipidemia is in the development of carotid atherosclerosis, in which significant gender differences are being more widely recognized. Lastly, the impact of stroke prevention with cholesterol lowering and BP lowering appears to be the same in men and women, but the attitudes about taking these medications may differ by gender.
It is now widely recognized that the prevalence of hypertension and hyperlipidemia is high in women, especially after menopause. Despite findings that major risk factors are more prevalent in women after middle age, cardiovascular and stroke risk is often under-recognized in women and, therefore, prevention and treatment strategies are less comprehensive than for men [45,46]. More work needs to be done to ensure that women receive adequate treatment of stroke risk factors in order to decrease the burden of stroke, especially in the elderly population.
Future perspective
Knowledge about stroke modifiable risk factors and their prevalence can help guide health policy-makers in developing more effective and tailored strategies for stroke prevention. Special attention is required to subpopulations having higher prevalence of certain risk factors. Not only do these subpopulations need to be recognized and the reasons for higher prevalence in their subgroup be identified, but further efforts have to be made to provide them with appropriate education regarding stroke, risk factors and medications to make prevention more effective.
Financial & competing interest disclosures
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Executive summary
Demographic studies have shown, that when matched by age, women have a lower risk of stroke but their rates of stroke are higher after the age of 85 years, since they are more likely to reach and exceed that age.
Women compose 60% of stroke mortality, have higher rates of disability and it has been shown that preventive and treatment options are not as comprehensive for women as for men.
Multiple studies evaluating baseline characteristics of patients with ischemic stroke and their comparison between men and women have shown that women have higher rates of hypertension and hyperlipidemia, which varies by geographic region.
Age plays a major role in the sex differences between risk factor prevalences in stroke patients, particularly hypertension, whereas hyperlipidemia is more prevalent in women regardless of age, as shown in a Korean study.
In women going through the menopausal transition, hyperlipidemia appears to be the risk factor most influenced by menopause, whereas hypertension appears to be more a factor of age due to its linear increase before, during, and after menopause.
Gender differences in relationship to adherence to stroke prevention medications are unclear because the results vary by the study. Regardless, nonadherence is of critical importance to the management of hypertension and hyperlipidemia and effective prevention of stroke in both men and women.
Knowledge of differences in modifiable risk factors between men and women with special attention to subgroups (race-ethnicities and geographic disparities) can help us in developing more effective strategies for stroke prevention and decrease its global burden.