
Abstract
Osteoporosis affects one out of three postmenopausal women. Their remaining lifetime risk of fragility fractures exceeds that of breast cancer. The risk of osteoporosis and/or fragility fractures can be reduced through healthy lifestyle changes. These include adequate dietary intakes of calcium, vitamin D and protein, regular weight-bearing exercise, reduction in alcohol intake and smoking cessation. European guidance for the diagnosis and management of osteoporosis in postmenopausal women recommends a daily intake of at least 1000 mg/day for calcium, 800 IU/day for vitamin D and 1 g/kg body weight of protein for all women aged over 50 years. The development of programs that encourage lifestyle changes (in particular balanced nutrient intakes) are therefore essential for the reduction of osteoporosis risk.
Osteoporosis is a progressive disease characterized by a decrease in bone mass and deterioration of bone structure leading to an increased risk of fragility fractures. Common osteoporotic fractures, such as those to the hip, spine, forearm and humerus, are often associated with debilitating pain that can lead to further physical disability, loss of independence, depression and premature death [1]. Using the WHO definition for osteoporosis (bone mineral density [BMD] ≥2.5 SD below the young adult mean), osteoporosis affected more than 22 million European women (22%) and 5.5 million men (7%) aged over 50 years in 2010 [1,2]. In 2010, the number of deaths due to fractures in Europe was 43,000 and the overall cost of osteoporosis to European healthcare systems was more than €37 billion [2]. Incident fractures accounted for 66% of this cost, long-term fracture care for 29% and pharmacological prevention for 5%. Given that the risk of osteoporosis significantly increases in people aged over 50 years, incidence is predicted to increase as the population ages and costs are expected to rise by 25% by 2025. Greater efforts are therefore required to prevent and manage this debilitating disease. The aim of this manuscript is to review the benefits of nutrition for the prevention of osteoporosis in postmenopausal women and to assess what can be done to increase osteoporosis awareness and encourage healthy lifestyle changes within this population.
Risk factors for osteoporosis
Bones start to grow before birth and continue to increase in size, strength and density until the end of the second decade of life, by which time more than 95% of maximum bone strength and density (peak bone mass) is acquired. After this, there is little change until menopause, when a rapid drop in estrogen production leads to an increase in bone turnover and accelerated bone loss, accompanied by microstructural alterations [3]. The overall effect of menopause is an average annual bone loss of 2–3% during the first few years and 0.5–1% thereafter [4]. Menopause is the biggest risk factor for osteoporosis in women.
Approximately 60–80% of peak bone mass variance is determined by genetics [5]. However, we can postulate that the risk of osteoporosis can be reduced by adopting healthy lifestyle choices that increase peak bone mass in children and adolescents, and reduce bone loss in adults [1,6–8]. Factors that improve bone health include nutrition (particularly calcium and protein intake, but also vitamin D, potassium, phosphorus and other micronutrients and macronutrients), regular weight-bearing exercise, smoking cessation (where appropriate) and reduced alcohol intake [6,8].
The role of nutrition in the prevention & management of osteoporosis
Calcium
Calcium is embedded in collagen fibrils in the form of calcium phosphate (hydroxyapatite) and is essential for bone rigidity. Studies show that children whose mothers consume higher levels of calcium-rich foods during pregnancy (milk, milk products, pulses, nonvegetarian foods, green leafy vegetables and fruit) have a higher bone mineral content (BMC) and BMD at 6–9 years of age [9,10]. Similarly, daily calcium supplements are associated with significant increases in total body BMC and upper limb BMD in children aged 3–18 years, even after the supplement is discontinued [11–14]. These studies suggest that increasing the level of calcium intake in children and adolescents has the potential to increase peak bone mass, thereby reducing the risk of osteoporosis later in life. In women who have already achieved their peak bone mass, increased calcium intake is associated with negligible bone loss (which means −0.014% per year vs −1% in control subjects) [15]. Moreover, high levels of dietary calcium intake and/or calcium supplements can significantly improve BMC and BMD, and reduce the risk of fractures during menopause [6–7,15–27]. Notably, however, studies in postmenopausal women and older men suggest that calcium supplements alone may not be sufficient to reduce fracture risk and that additional vitamin D supplementation is required [28].
A meta-analysis has raised the concern that calcium supplements, particularly when administered without vitamin D, are associated with an increased risk of myocardial infarction [29]. Some epidemiological studies support this series of analyses. However, it appears this possible increased risk of cardiovascular events are not observed with food sources of calcium, despite similar benefits on bone density, and may be on fracture risk. Therefore food sources of calcium may be preferable.
Vitamin D
Calcium homeostasis is, to a significant extent, regulated by vitamin D. Vitamin D is obtained from cutaneous synthesis after sunlight exposure (80–90%) and from a limited number of foods, such as oily fish, mushrooms and some fortified dairy products (10–20%) [30]. Vitamin D deficiency decreases the amount of calcium absorbed from the intestine and increases levels of parathyroid hormone (PTH). This, in turn, rebalances the decrease in serum calcium by increasing calcium resorption from the bone [7,31–34].
Serum levels of 25-hydroxyvitamin D [25(OH)D] lower than 50 nmol/l have a detrimental effect on bone health and may exacerbate osteoporosis in elderly or postmenopausal women by increasing the rate of bone turnover. Studies have shown that vitamin D supplementation is associated with a reduced risk of fragility fractures [35–37] and survival [38,39] in elderly subjects. Moreover, vitamin D supplementation can reduce the risk of falls by improving muscle strength and physical stability [40–42].
Protein
Protein accounts for approximately 50% of bone volume and about a third of its mass [43]. Cross-linking of collagen molecules in bone involves the modification of amino acids, and many of the collagen fragments released during the bone remodeling process cannot be reused to build new bone. As well as providing the structural matrix for bone, protein optimizes levels of IGF-I, a hormone that stimulates bone growth, increases calcium and phosphorus absorption in the gut, through the synthesis of calcitriol and increases the rate of phosphate reabsorption from the kidney [32]. Adequate supplies of dietary protein are therefore required for healthy bone maintenance.
Variations in protein intake within the ‘normal’ range (around 0.8–1.5 g/kg body weight/day) account for 3–4% of the variance in peak bone mass attainment in well-nourished children and adolescents [6,44]. A higher dietary protein intake is associated with greater muscle mass and strength, both in postmenopausal women [45–49] and in young, healthy women following exercise [50]. In older people with osteoporosis, increased levels of protein intake (≥0.8 g/kg body weight/day or 24% of total energy intake) are associated with higher BMD [48,51–53], a slower rate of bone loss [49,54] and a reduced risk of hip fracture [55,56]. In one study, low serum IGF-I concentrations predicted the risk of osteoporotic fractures in postmenopausal women independent of BMD [57]. This suggests that IGF-I concentrations may have an important role in maintaining bone and muscle strength.
Nutritional targets for the reduction of osteoporosis risk
Balanced nutritional intakes represent the first step in an effective preventive strategy. However, in the presence of increased risk of fracture and/or osteoporosis, this approach may not be sufficient and the management of those patients requires the administration of drugs whose antifracture efficacy has been demonstrated in well conducted clinical trials with fracture as the primary outcome. Regarding vitamin D, a meta-analysis of 17 studies including 52,625 subjects aged over 50 years showed that adequate levels of both vitamin D and calcium were associated with a 12% risk reduction in all types of fracture and a reduced rate of bone loss in studies reporting BMD [17]. These data are supported by a further meta-analysis in which high levels of calcium and vitamin D were associated with an 18% reduction in hip fracture risk compared with no treatment [18]. More recent studies support a target intake of 800 IU vitamin D per day with or without additional calcium supplementation with a documented significant 30% reduction of hip fractures and a 14% significant reduction of any nonvertebral fractures [35,37]. Based on these and similar studies, the Institute of Medicine suggests a recommended daily intake (RDI) of 800 mg/day for calcium and 400 IU for vitamin D throughout adult life and, for women aged over 50 years, a recommended daily allowance of 1000 mg/day for calcium (Table 1) [58]. Slightly higher RDIs for calcium and vitamin D, plus a new target for protein, are recommended by the European Guidance for the Diagnosis and Management of Osteoporosis in Postmenopausal Women (Table 1) [59]. Here, the RDIs for women aged over 50 years are ≥1000 mg/day for calcium and 800 IU for vitamin D (800–1000 IU/day for those with serum levels of 25-hydroxyvitamin D [25(OH)D] lower than 50 or 75 nmol/l in those with a high risk of falls and fractures) and 1 g/kg body weight for protein [59]. The best way to achieve these targets is though a healthy diet. As calcium is mainly provided in dairy products, dairies fortified with calcium and vitamin D that provide at least 40% of the RDI of calcium (400 mg) and 200 IU of vitamin D per portion are valuable options for the long-term attainment of these targets [59].
Dietary reference intakes for calcium, vitamin D and protein in women over the age of 50 years.
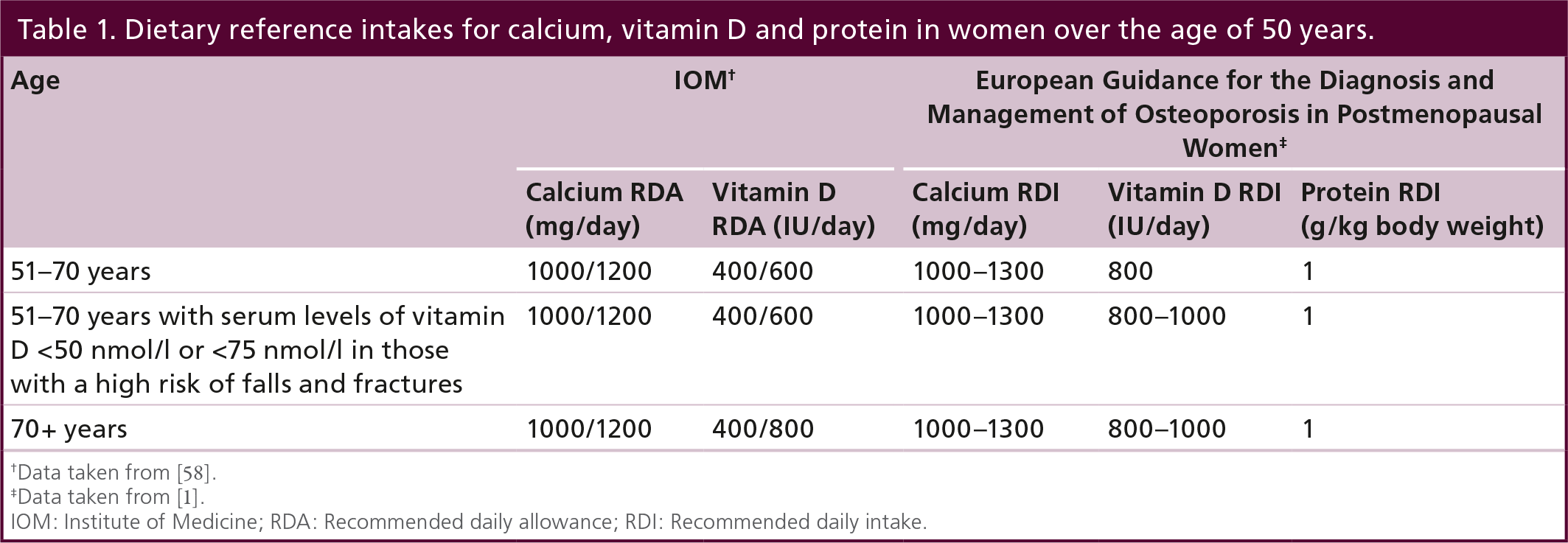
Data taken from [58].
Data taken from [1].
IOM: Institute of Medicine; RDA: Recommended daily allowance; RDI: Recommended daily intake.
Role of dairy products in the reduction of osteoporosis risk
Dairy products provide more calcium, protein, magnesium, potassium, zinc and phosphorus per calorie than any other food (Table 2) [32,60]. Approximately 250 mg of calcium can be obtained from a single 200 ml glass of milk, a 180 g serving of yoghurt or 30 g of hard cheese, which means the RDI for calcium can be obtained from only three to four portions of dairy. Up to 24 servings of green vegetables, or 48 servings of whole grain or refined grain foods would be required to have the same effect [61]. In addition to calcium, 1 l of milk provides around 32–35 g of protein [6]. Overall, dairy products may represent up to 52–65% of the RDI of calcium and 20–28% of the RDI of protein [6,14, 62]. Moreover, given the high prevalence of vitamin D insufficiency and the relatively low number of vitamin D rich foods (Table 3), a number of countries supplement certain foods (often milk, margarine, butter and yoghurt) with vitamin D [63]. The rationale for this is that vitamin D and calcium – both key elements for bone health – should be available in the same food products.
Nutrient content per 100 g (unless otherwise stated) of selected dairy food.

Depending on the preparation procedure, yoghurt may have calcium and protein contents similar to plain milk.
Data taken from [64].
Vitamin D content per 100 g (unless otherwise stated) of selected food.
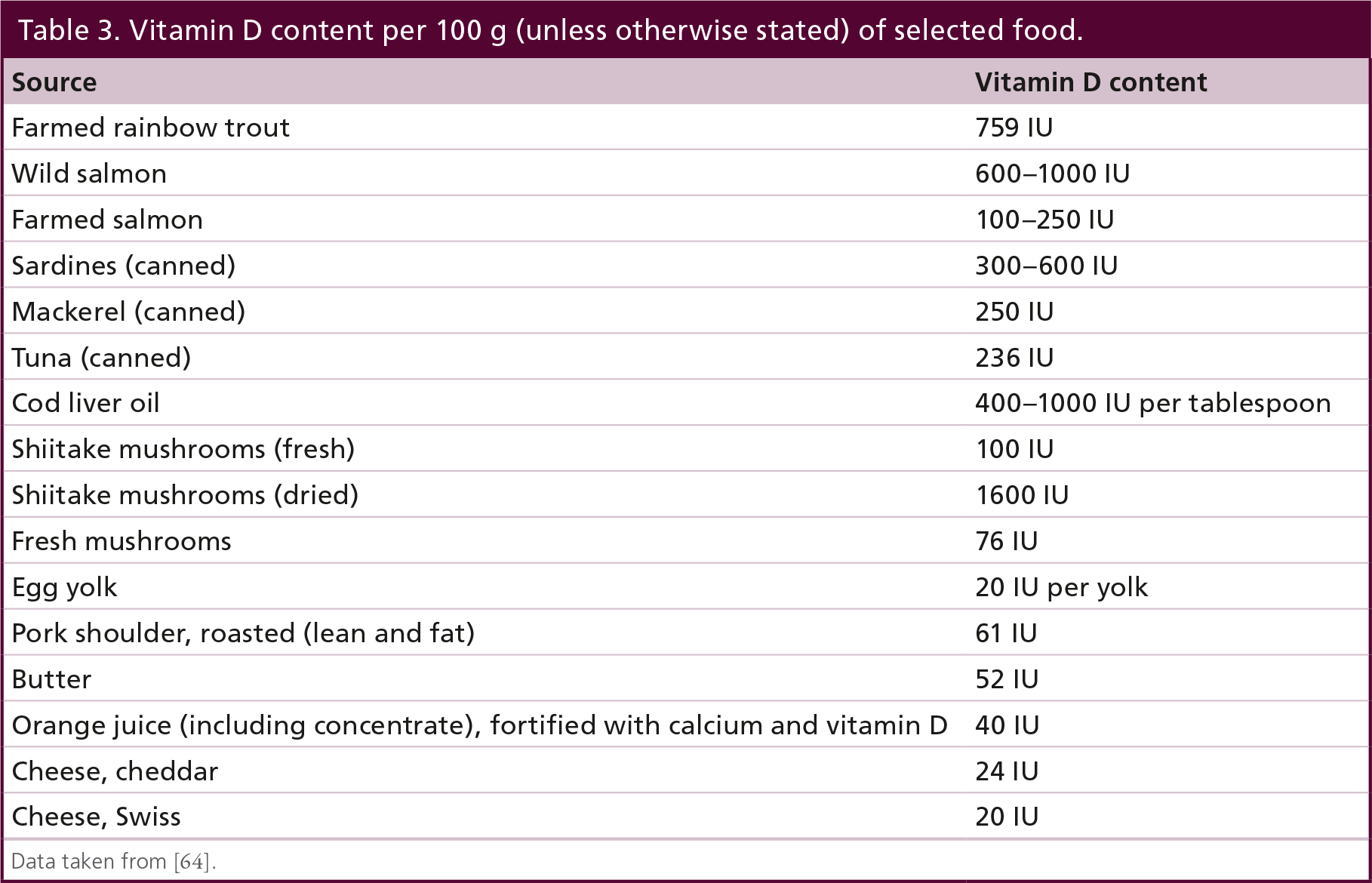
Data taken from [64].
Numerous randomized controlled trials and observational studies have examined the effects of dairy product consumption (including fortified dairy foods) on markers of bone activity and bone turnover in women [7,16,19,27,49,50,65]. In young, healthy women, consumption of fat-free milk versus an isoenergetic carbohydrate drink after resistance exercise promoted fat loss, lean mass gains or maintenance, improved BMD at clinically important sites and reduced bone resorption [50,65]. These studies suggest that the timing of milk protein intake after exercise is important for optimal bone health. In postmenopausal women of all ages, the consumption of soft cheese fortified with vitamin D and calcium increased protein intake and serum levels of IGF-I, and reduced levels of PTH, tartrate-resistant acid phosphatase isoform (TRAP) 5b and cross-linked teleopeptide of type 1 collagen (CTX) (biomarkers for bone resorption) [19,20]. Similar reductions in PTH levels and/or biomarkers of bone turnover were observed in premenopausal and postmenopausal women consuming milk or yoghurt fortified with vitamin D and/or calcium [21–25]. However, the greatest improvements in biomarkers for bone turnover were observed in studies that ensured compliance with fortified dairy products using a long-term (12–30 months) intervention approach that combined dietary changes with lifestyle and nutrition counseling [26,27].
High protein diets are often criticized for their potentially harmful effects on bone health, in particular increased urinary calcium excretion. However, a study in 130 overweight middle-aged subjects (71 female) randomized to a weight loss diet providing 1.4 g/kg/day protein and three daily servings of dairy protein or 0.8 g/kg/day protein and two daily servings of dairy showed that, if the protein source includes dairy, bone health can be improved [49]. In this study, the high dairy protein diet increased urinary calcium excretion but improved calcium intake and increased whole body, lumbar spine, hip and total BMD. Further studies are required to fully understand the effects of dairy versus nondairy protein on bone health.
Although BMD or BMC changes provide useful information about the impact of nutrition on bone strength, age and extraskeletal factors must be taken into account when determining fracture risk [66]. Data on the relationship between dairy food intake and fracture risk are limited. A meta-analysis data from six studies in 195,102 women found no overall association between total milk intake and hip fracture risk [67]. However, a 12-year follow-up of the Framingham Offspring Study showed that dairy intake was related to hip but not spine BMD, and that yoghurt intake was related to hip (trochanter) BMD alone [68]. Yoghurt intake also showed a weak positive protective trend for hip fracture, while no other dairy groups showed a significant association. This suggests that not all dairy products are equally beneficial for bone health and that further studies are needed to assess the impact of various dairy products on bone turnover, BMC/BMD and fracture risk.
Calcium, vitamin D & protein insufficiency is common among postmenopausal women
Calcium and vitamin D intakes for postmenopausal women in Europe typically fall well below the RDIs (Figure 1). Mean calcium intakes for women aged over 50 years across five European countries range from just over 600 mg/day in Bulgaria to 900 mg/day in Portugal (Figure 1A) [7]. Although calcium levels tend to decrease in older women, a survey of girls and young women (aged 11–23 years) from six European countries showed that mean calcium intake is also inadequate in younger populations [69]. In France, 63–73% of girls aged 11–17 years consumed less than two-thirds of their RDI for calcium [70]. This suggests that calcium insufficiency is common throughout life.
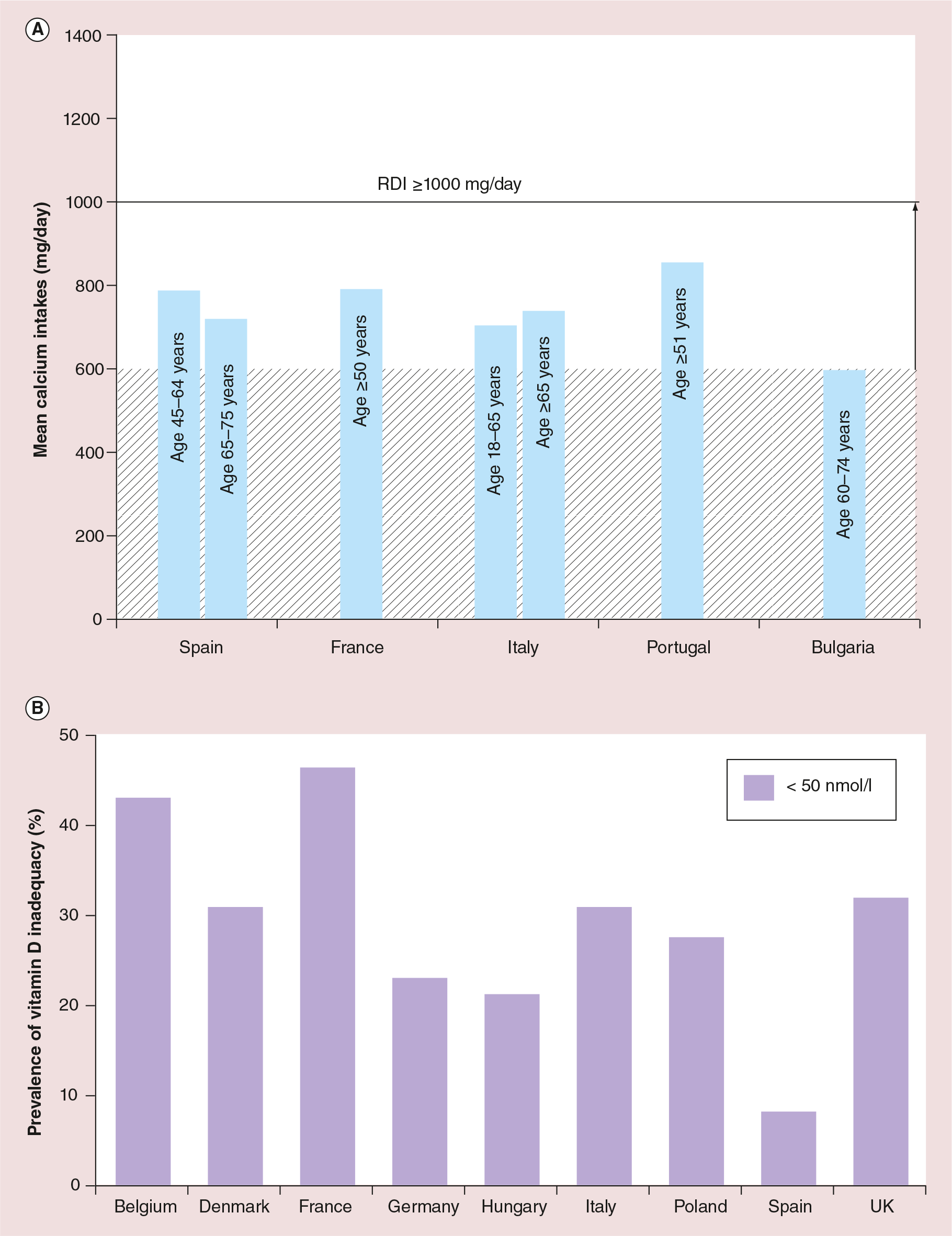
Assessment of vitamin D levels in 8532 post-menopausal women with osteoporosis or osteopenia in nine European countries showed that serum 25-hydroxyvitamin D [25(OH)D] levels ranged from 51.5 nmol/l in France to 85.2 nmol/l in Spain (Figure 1B) [71]. Overall, 79.6% of women had levels lower than 80 nmol/l and 32.1% had lower than 50 nmol/l. A further study carried out in 11 European countries showed that vitamin D levels are considerably lower in winter, when almost 50% of women have 25-hydroxyvitamin D [25(OH)D] lower than 30 nmol/l [77]. Unlike calcium and vitamin D intakes, protein insufficiency is generally not a problem among younger European adults [78]. However, approximately 27–41% of older women (aged over 80 years) ingest less than their RDI of protein [79].
What can be done to improve nutritional target attainment?
A survey carried out by the International Osteoporosis Foundation (IOF) (n = 1200) found that 60% of women know they are likely to develop osteoporosis at some point in their lives and that 99% of respondents (men and women) understand the importance of calcium (in particular dairy products) for maintaining bone health [80]. However, fewer respondents (65 and 59%, respectively) are aware of the benefits of vitamin D and protein intake, 60% are unaware of dietary sources of vitamin D and only a small proportion of respondents engage in preventive health behaviors. Frequently reported barriers to obtaining adequate calcium intake include uncertainty regarding nondairy calcium food sources and supplements, and concerns that the high fat/cholesterol content of calcium-rich foods might cause weight gain and cardiovascular disease [81]. Together, these studies highlight the need to educate patients about the importance and potential sources of calcium, vitamin D and protein, and suggest that patients need to be reassured that their increased consumption of milk fat is unlikely to increase their risk of cardiovascular disease [82].
A number of different approaches are used to increase bone health awareness and encourage lifestyle changes. These include public health education programs, community projects, websites and nutritional and fitness guidelines [7]. The overall goal of health education is to ensure that individuals have an understanding of their current health status in order to make informed decisions about lifestyle changes and treatment. If a patient is aware they have a low BMD, they are more likely to increase their knowledge of osteoporosis and take appropriate steps to reduce their fracture risk. In one study, providing healthy postmenopausal women with their bone scan results increased perceived susceptibility to fracture and led to significant increases in calcium intake over the next 6 months [83]. However, many individuals do not undergo appropriate osteoporosis screening and are unaware of their fracture risk [84]. Educating physicians about the use of the Fracture Risk Assessment (FRAX) tool will encourage them to determine their patients’ 10-year probability of hip fracture or a major osteoporotic fracture, and will most likely lead to greater patient awareness and improved lifestyle [66].
Recently, the scorecard for osteoporosis in Europe (SCOPE) project reviewed all information available on osteoporosis across the 27 countries in the European Union and developed color-coded scorecards that highlight differences between countries in the burden of osteoporosis and fractures, policy framework and treatment provision and uptake [1]. It is hoped that the scorecard will enable healthcare professionals and policy makers to assess their country's general approach to the disease, thereby improving the management of bone health throughout Europe.
Conclusion
Osteoporosis is a debilitating disease that leads to fragility fractures, high morbidity and mortality and high healthcare costs. The greatest risk factor for osteoporosis in women aged over 50 years is the menopause. However, risk can be reduced by adopting a healthy lifestyle that includes adequate levels of dietary calcium, vitamin D and protein, regular weight-bearing exercise, smoking cessation and limited alcohol intake. European Guidance for the Diagnosis and Management of Osteoporosis in Postmenopausal Women recommends an RDI ≥1000 mg/day for calcium, 800 IU for vitamin D and 1 g/kg body weight for protein for all women aged over 50 years. An easy way to achieve these targets is though a healthy dairy-rich diet, including dairy products fortified with calcium and vitamin D, such as yoghurt and milk. Despite this, calcium and vitamin D insufficiency in postmenopausal women is common across Europe.
Future perspective
Primary prevention should be implemented as early as during childhood and adolescence, and after the menopause. Further development of educational initiatives and behavioral change programs designed to increase osteoporosis awareness and improve dietary nutrient intakes are therefore essential if the prevention and management of osteoporosis are to be improved. The efficacy of these measures should be verified with appropriate indicators.
Executive summary
Factors that maintain bone health include nutrition, weight-bearing exercises and avoidance of deleterious influences.
Calcium and vitamin D reduce fall and fracture risk.
Adequate dietary protein intakes are required for healthy bone maintenance.
Dairy products provide more calcium, protein, phosphorus, potassium, zinc and magnesium per calorie than any other food.
There is a need to educate subjects about the importance and potential sources of calcium, vitamin D and protein.
Footnotes
R Rizzoli is part of the advisory board and speaker bureau for Amgen, Danone, GSK, MSD and Servier. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing and editorial assistance was provided by J Read and L Buttle of Chill Pill Media, LLP, thanks to a grant from the Danone company.