
Abstract
A considerable number of breast cancer diagnoses are made in older women. Differing physiological needs of older patients and biology of tumors compared with younger patients may alter treatment options between surgery and nonsurgical primary approaches. Adjuvant therapies may benefit these patients; however, concerns about toxicity and physical demands of treatment may affect patient choice regarding treatment. Furthermore, quality of life may be more important to the older individual than curative treatment alone. Growing evidence is emerging for employing Comprehensive Geriatric Assessment to determine other factors that may contribute to treatment decision-making in the older population. The way geriatric oncology is delivered varies, bringing the importance of the multidisciplinary team to the forefront of care delivery in this age group. Future research in this area should include combined consideration of tumor biology and geriatric needs.
The ‘problem’
In 2010, breast cancer accounted for 31% of female cancer diagnoses in the UK, being the second most common cause of cancer death in women [1]. Survival from breast cancer has improved in recent years and this can be attributed to improved diagnostic and management facilities [2]. Over 45% of breast cancer diagnoses are made in those over 65 years of age and 33% in those over 70 years. With 16% of the UK population considered elderly and the fact that this figure is likely to be increasing, it is concerning to discover that most research efforts in breast cancer have been aimed at younger patients [3,4]. Current literature suggests that older women are often ‘under’-treated [5,6].
As age advances, women not only have a higher risk of developing breast cancer but there is also evidence suggesting changes in the biological characteristics of the tumors; for example, breast cancers in older women tend to be estrogen receptor (ER)-positive and HER2-negative [7,8]. However, there is only limited literature available focusing on understanding the biology of breast cancer in older women. Studies are mainly retrospective and/or based on multi-institutional registries such as those from the Surveillance Epidemiology and End Result (SEER) program and San Antonio database, where variations exist in terms of the methodology of tumor analysis [8]. Definitions of the older population in these studies also vary, for example, using postmenopausal status or age at diagnosis as cut-offs (55, 60, 65 and 70 years). The authors' group has also attempted to compare the biology of breast cancers in younger versus older women managed in one single institution and using the same laboratory methodology [9]. Not only was a changing pattern with age shown but also a new cluster with distinct biological pattern (‘low ER luminal’) has been identified in the older cohort (Figures 1 & 2).
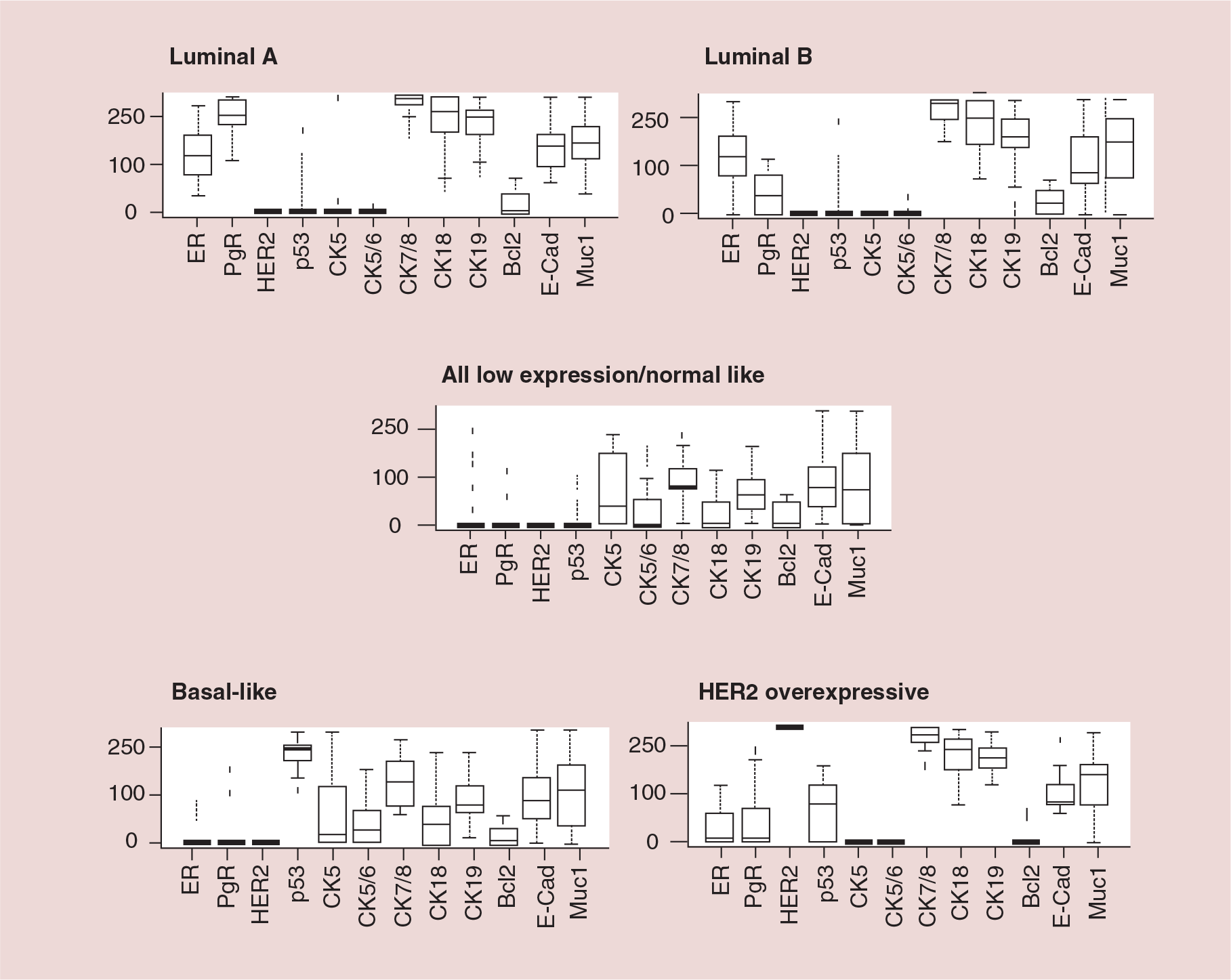
Biological classification of primary breast cancer in young (>70 years) women.
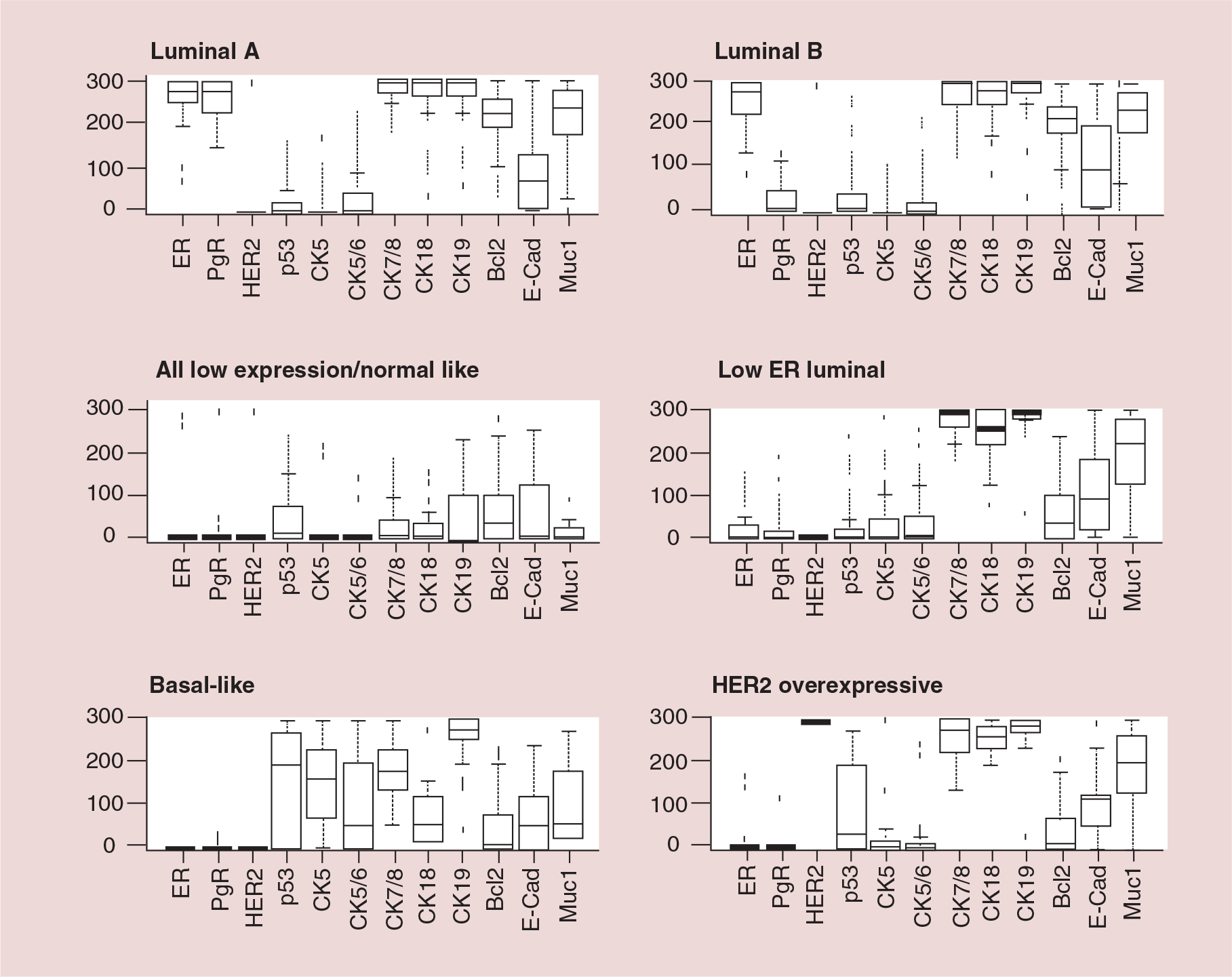
Biological classification of primary breast cancer in older (≥70 years) women.
Apart from differing tumor biology, there are geriatric issues specific to the older population that would impact on the management of breast cancer. There are often larger individual variations in terms of sensitivity to anesthetics, physiological reserve in renal function and other body systems, which could have a bearing on postoperative complications, recovery time and hospital stay following surgery [10–13]. In addition, older patients are more likely to be suffering from other comorbidities. Patients ≥80 years of age have been found to have on average five medical conditions that affect their overall survival, as compared with patients in their fifties who have been shown to have only one or two other serious illnesses [14]. The presence of comorbidities increases the risk of death from causes other than breast cancer [15]. For these reasons it may be that chemotherapy and radiotherapy are much more commonly used to treat younger patients and older patients are often not keen to undergo more aggressive therapies. These adjuvant therapies may have adverse effects, for example, regarding cognitive impairment and behavioral deficits, of which the elderly are more susceptible to [16]. Moreover, some of these patients may have only a limited life span from coexisting disease or may have contraindications to undergo intensive therapy. However, when considering early operable primary breast cancer in the elderly, the morbidity associated with surgery for breast cancer is minimal [5].
Managing primary breast cancer: ‘fixing’ the problem
In order to ‘fix’ the problem, which is of growing concern due to the aging population worldwide, both the unique tumor biology and specific geriatric needs of the older woman in question have to be considered. Possible ideal models of care need to be explored in order to optimize the treatment of primary breast cancer in this group of patients.
Biological differences & clinical relevance Primary treatment (breast)
Surgery versus nonoperative therapy
Surgery has been the standard of treatment for early operable primary breast cancer. However, in older frail patients, or those with a number of comorbidities and limited life expectancy and also those with a number of social issues, surgery may not be the appropriate answer. Given the high preponderance of ER-positive tumors in older women, tamoxifen was historically used with the hope of controlling the cancer in these frail women who might eventually die from inter-current illnesses. A Cochrane systematic review of seven randomized controlled trials comparing surgery with primary endocrine therapy in this population did not show any significant difference in overall survival [17]. However local control was better in the surgery arm. The key issue here is the fact that all except one trial were unselected for ER. Inclusion of patients with ER-negative tumors (amounting to ~20% even in the older population [18]) could potentially ‘contaminate’ the results. Summaries of the studies are given in Tables 1–3 and there is a trend of increasing chance of response with ER positivity seen [19–26].
Summary of studies assessing the role of primary endocrine therapy in older women with operable primary breast cancer: randomized studies – estrogen receptor nonselective.
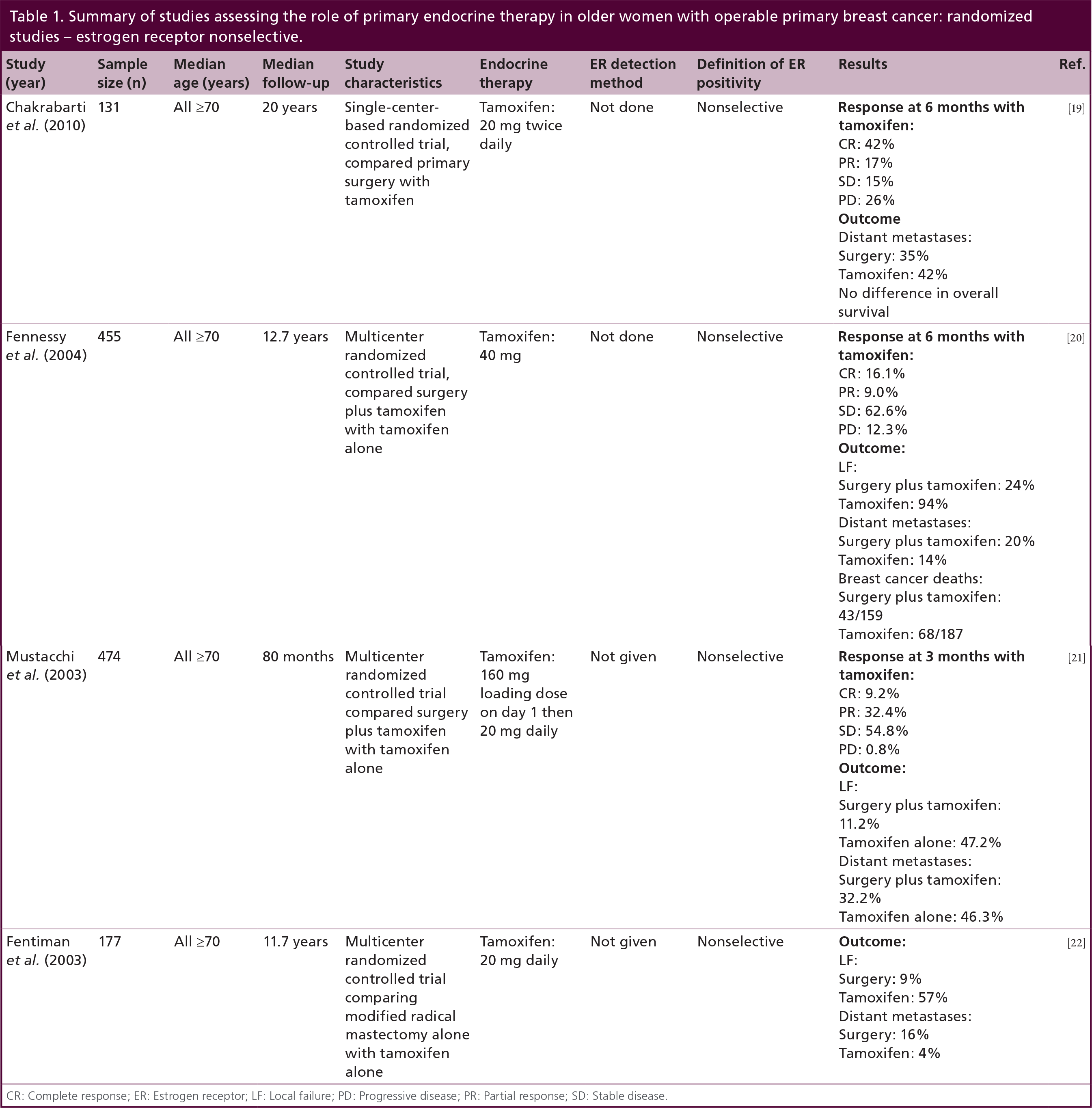
CR: Complete response; ER: Estrogen receptor; LF: Local failure; PD: Progressive disease; PR: Partial response; SD: Stable disease.
Summary of studies assessing the role of primary endocrine therapy in older women with operable primary breast cancer: nonrandomized studies – estrogen receptor selective.

CR: Complete response; ER: Estrogen receptor; ERICA: Estrogen receptor immunocytochemical analysis; IHC: Immunohistochemistry; LF: Local failure; PD: Progressive disease; PR: Partial response; SD: Stable disease.
Summary of studies assessing the role of primary endocrine therapy in older women with operable primary breast cancer: randomized studies – estrogen receptor selective.

CR: Complete response; ER: Estrogen receptor; ERICA: Estrogen receptor immunocytochemical analysis; PD: Progressive disease; PR: Partial response; SD: Stable disease.
Not only is selection of ER positivity important, but the degree of ER positivity is also vital in determining the scale of benefit of primary endocrine therapy. In a large series from the authors' group, older women with strongly ER-positive (histochemical [H]-score ≥250 [out of 300]) tumors showed comparable breast cancer-specific survival regardless of initial treatment by surgery or primary endocrine therapy [28]. For patients with significant comorbidities increasing the chance of dying from other competing causes, such equivalence in breast cancer-specific survival (which is a surrogate for biological behavior of the tumor) could translate into an improved overall survival benefit. In addition all patients having an H-score ≥250 achieved clinical benefit at 6 months from starting primary endocrine therapy [28], which has previously been shown to correlate with a survival advantage when compared with those patients who progress prior [29].
Therefore, while surgery is the primary treatment of choice, primary endocrine therapy is an excellent alternative in those older women with strongly ER-positive tumors, especially when they have limited life expectancy due to frailty and/or comorbidities. With the superiority of aromatase inhibitors (AIs) shown over tamoxifen in the adjuvant setting, it is likely that when an AI is used for this purpose, the scale of benefits of primary endocrine therapy as explained above would be enhanced. For the significant minority of patients with ER-negative disease, surgery remains the most important treatment.
Primary treatment (axilla)
Axillary surgery remains an important part of the surgical management regardless of age. As will be explained later, while sentinel node biopsy is now the standard axillary staging procedure, the key questions for those patients with positive sentinel node(s) are whether axillary dissection is required, and whether it could be replaced by axillary radiotherapy, in order to reduce morbidities, notably lymphoedema. Furthermore, how are these questions relevant to the older population given their distinct biology?
A multicenter randomized controlled trial comparing axillary dissection versus no axillary dissection in older women with clinically node-negative early operable primary breast cancer receiving adjuvant tamoxifen (regardless of ER status) did not show any significant difference in metastasis and disease-free survival at a median follow-up of 6.6 years [30]. Regional recurrence rate was slightly higher in the no axillary surgery arm (3 vs 1% in the axillary surgery arm) although the difference was not statistically significant. In a retrospective review of 184 older women with operable primary breast cancer undergoing primary surgery, 25 of them had excision of obviously enlarged lymph nodes at the same time. After a median follow-up of 54 months, 16 and 14% had regional recurrence in patients with and without axillary exploration respectively. In addition, those who developed regional recurrence had ER-negative and high-grade tumors [31]. These suggest that ER status and endocrine therapy have a role to play in influencing the risk of regional recurrence.
The aforementioned question has since been explored in the era of sentinel node biopsy by randomized controlled trials such as the IBCSG 23–01 trial and ACOSOG Z0011 trial [32,33]. The results demonstrated no additional benefit by completing axillary dissection following removal of positive sentinel nodes as part of the sentinel node biopsy procedure. The Z0011 trial demonstrated this in a series of postmenopausal women treated also by intact breast irradiation following breast conserving surgery, and by adjuvant endocrine therapy for ER-positive disease [33]. This again supports the effect of endocrine therapy in regional control, even in cases of known involved sentinel nodes. On the other hand, another possible contributing factor is the effect of tangential coverage of the low axilla by radiotherapy, which was intended to treat the whole breast following surgery.
The effect of formal axillary radiotherapy as an alternative to axillary dissection was tested by the AMAROS trial, which randomized patients into either treatment following a positive sentinel lymph node biopsy [34,35]. Regional recurrence rates were shown to be very low in both arms (0.54 and 1.03% in axillary lymph dissection and radiotherapy arms, respectively, at 6.1 years median follow-up).
Given these findings, which have been demonstrated in trials that included younger patients, adopting a more conservative approach to the axilla should be of even greater relevance to older women with breast cancer, especially those with strongly ER-positive disease taking endocrine therapy. For those with ER-negative disease, a more aggressive approach to the axilla should be considered, especially in patients who are deemed unfit to receive chemotherapy, which could have an additional impact on regional control.
Breast reconstruction
The trend of breast reconstruction following mastectomy reduces as the age advances. Data including 19,234 patients from the SEER database demonstrated that only 6% of older (≥65 years) women had reconstruction following mastectomy [36]. There is literature available suggesting similar outcome of the reconstruction; however, due to longer hospital stay and related social issues, older patients tend to avoid reconstruction procedures. Zidak and colleagues analyzed women's choice regarding reconstruction according to their age, and concluded that younger women are more concerned regarding their body shape as compared with older women [37].
Primary radiotherapy
Primary radiotherapy may be an option for those patients with low ER-positive or ER-negative disease. Evidence is limited regarding the use of radiotherapy in the primary setting. The use of hypofractionated radiotherapy (single weekly dose of 6.5 Gy corresponding to 5 fractions, with total dose of 32.5–45.5 Gy) was reported in two relatively small retrospective studies showing a reasonable local control in those patients who did not have surgery [38,39]. However, the interpretation of their results is confounded by the use of concurrent tamoxifen. In the neoadjuvant setting, a small series including 75 patients aged from 32–82 years were given 45 Gy dose of radiation in 5 weeks preoperatively for operable breast cancer (T2 and T3 disease). All patients then underwent lumpectomy and the pathological analysis of the tumors showed 11% complete remission of the tumors [40]. The results suggest a potential role for radiotherapy as a primary treatment in selected group of patients.
For older women with ER-negative tumors (or ER-positive tumors that have developed
Adjuvant treatments Adjuvant radiotherapy
Postmastectomy radiotherapy
Young age is known to be associated with a high risk of local recurrence for breast cancer. Despite the lack of high-level randomized trials focusing on the older population, at least two large retrospective studies have demonstrated the benefit of postmastectomy radiotherapy, mainly in high-risk patients. An analysis of 11,594 older women (≥70 years) from the SEER database, where the majority of tumors were ER-positive (i.e., 82%), demonstrated that postmastectomy radiotherapy only produced a survival benefit in high-risk patients with T3/T4 tumors and/or positive axillary lymph nodes [42]. Similar findings were observed in another retrospective study of 2362 postmenopausal women [43]. Within the group of patients >70 years the locoregional recurrence was significantly higher among the patients with ≥4 positive lymph nodes (p < 0.001) [43].
Radiotherapy following breast conservation
In a similar way, age also plays a part in the risk of local recurrence following breast conserving surgery. The Oxford overview of 78 randomized controlled trials including all age groups (n = 7311) demonstrated that radiotherapy produced a significant overall improvement in local control, as well as in breast cancer-specific survival [44]. However, age-stratified analyses indicated a smaller absolute reduction of local recurrence in older women (11% in women over 70 years as compared with 22% in those <50 years).
As shown in the summary of the key studies, which included a reasonably large proportion of older women (Table 4), there appears to be a minimal impact on survival outcome due to adjuvant radiotherapy that mainly produced improvement in local control, which was already very good in this population [45–51]. These findings were supported by a multicenter randomized controlled trial (radiotherapy vs no radiotherapy in older patients taking tamoxifen) after a median follow-up of 10.5 years [52], which led to a change in the National Comprehensive Cancer Network guidelines in the USA. Thus, it would not be unreasonable to omit radiotherapy in low-risk older patients who are taking adjuvant endocrine therapy for ER-positive tumors following breast conserving surgery.
Summary of studies assessing the role of postoperative radiotherapy in older women with operable primary breast cancer.

Radiotherapy.
Local recurrence.
Breast cancer-specific survival.
Overall survival.
Wide local excision.
10-BCSS: Breast cancer-specific survival; 10-OS: Overall survival; adj.: Adjuvant; ER: Estrogen receptor; LR: Local recurrence; Mets: Metastases; OS: Overall survival; RR: Regional recurrence; RT: Radiotherapy; SEER: Surveillance, Epidemiology and End Result Project; Tam: Tamoxifen; WLE: Wide local excision.
Intraoperative radiotherapy
Given the reduced absolute benefit of conventional radiotherapy related to the low risk of local recurrence in the older population, and the fact that most local recurrences tend to occur within the same quadrant of the original tumor, intraoperative radiotherapy could be an excellent alternative strategy. High-level evidence was obtained in a randomized international multi-center Phase III trial (n = 2232) including all age groups (40% were >65 years) [53]. At 4-year follow-up there was no significant difference in local failure where four local recurrences were observed in the intraoperative radiotherapy arm and five in the external radiotherapy arm. Given the biological argument mentioned above, intraoperative radiotherapy would appear to be ideal for older patients with low-risk and ER-positive disease receiving adjuvant endocrine therapy. This would save patient travel, which is of particular importance to this population.
Hypofractionated radiotherapy
Another way to reduce treatment time is hypofractionation. A retrospective analysis was carried out in a study which included 150 patients (median age 78 years) with T1–4 breast cancer [54], showing excellent local control with hypofractionation using 6.5 Gy in 5 fractions at a total dose of 32.5 Gy once weekly. Furthermore, the results of two randomized controlled trials comparing different radiotherapy regimens have recently been reported. The UK START ran two trials. The START A trial compared 50 Gy in 25 fractions over 5 weeks versus 41.6 Gy in 13 fractions over 5 weeks versus 39 Gy in 13 fractions over 5 weeks [55,56]. The START B trial compared 50 Gy in 25 fractions over 5 weeks with 40 Gy in 15 fractions over 3 weeks [56]. Both trials included all age groups where 11 and 12% of patients were over 70 years of age in trials A and B, respectively. They both demonstrated that better cosmetic outcome was achieved by the hypofractionated regimens while there was no difference in local control across all regimens. As such, hypofractionation has been proven to produce efficacy similar to the longer conventional regimen, without compromising cosmesis. This would appear an attractive option especially to the older population.
Adjuvant endocrine therapy
The currently available adjuvant endocrine therapy options are tamoxifen and the third-generation AIs including anastrozole, letrozole and exemestane. It has been established by multiple randomized trials (conducted not exclusively on the older population) that these AIs produce significantly greater survival benefits when compared with tamoxifen [57].
For long-term use of adjuvant therapy in older women, safety profile is a very important consideration. Although there might have been a selection bias towards the fit patients in these trials, with an underrepresentation of older women with comorbidities, in terms of bone (including debilitation due to arthralgia) and cardiovascular health, tamoxifen remains the better therapy and, for endometrial health, the AIs [58]. Nonetheless, owing to polypharmacy and drug interactions (e.g., between tamoxifen and warfarin), clinicians need to consider additional factors when deciding to prescribe an endocrine agent. From the biological perspective, as older women do not just tend to have ER-positive tumors, these tumors tend to be ER-rich (with a high H-score), making them extremely hormone sensitive [18]. Therefore, the efficacy difference between tamoxifen and AIs seen in younger patients may be narrower in the older population, implying that a switch between the two classes of agents due to tolerability might not produce a huge impact on clinical outcome.
Adjuvant chemotherapy
The use of chemotherapy in older patients is controversial due to their compromised physiological reserves, chemotherapy-induced toxicities and high prevalence of ER-positive tumors, where adjuvant endocrine therapy offers an excellent therapeutic option as discussed earlier. However, a small proportion of them develop ER-negative tumors (~20%), and for them chemotherapy is the only available option if they require any systemic therapy. There is also a small group of patients who have high-risk cancers (e.g., heavily involved axilla, HER2- and Ki67-positive tumors) where the consideration of chemotherapy, even in the presence of ER-positive tumors, may be appropriate. A retrospective analysis of the SEER database including 1711 older (>65 years) women with stage I-III disease with hormone receptor (both ER and PR)-negative tumors showed that adjuvant chemotherapy produced a 15% improvement in all-cause mortality at 7 years [59]. The effect of chemotherapy was noted to be independent of age, where all patients benefited equally when stratified by age, although it was more pronounced in patients with lymph node-positive disease, as shown in the latest Oxford Overview (meta-analysis of 123 randomized trials on adjuvant chemotherapy involving 100,000 patients) [60]. Older women are generally considered to have poorer general health and hence are thought to be less likely to tolerate conventional chemotherapy. As such Muss
The clinical relevance of differing biology in older women with breast cancer may not be restricted to ER-positive disease. The authors' group have investigated this in patients with triple-negative disease [62]. Comparing 127 patients aged 70 years or above with their younger counterparts (n = 342), although 47% of the latter received chemotherapy and none in the older group, no significant difference in clinical outcome was seen in both groups in terms of breast cancer-specific survival, and time to metastasis and local and regional recurrences. These findings suggest that there are other biological factors operating in the older patients which should be further explored when evaluating the precise role of chemotherapy in these patients.
Considering neutropenia as the major side effect of chemotherapy, the role of prophylactic use of granulocyte colony-stimulating factor cannot be underestimated. However there is insufficient evidence to recommend its routine use. A retrospective analysis of older patients receiving chemotherapy showed that when they were given prophylactic granulocyte colony-stimulating factor there was 17% reduction in hospitalization for neutropenia [63]. Thus, such prophylactic therapy may be considered in older patients receiving chemotherapy.
Trastuzumab
Only 16% of the studied patients belonged to the older population in the established trials on adjuvant trastuzumab including the HERA [64], NSABP B-31 [65] and NCCTG N9831 [65] trials. Regardless of age there was remarkable improvement in clinical outcome when trastuzumab was given. Age stratification analysis from the HERA trial showed 9% absolute benefit in disease-free survival in women >65 years of age, although the benefit in <50 years was much higher (46%).
Along a similar storyline is seen in triple-negative disease suggesting a more complex and differing biology operating in older women, data from the authors' group indicated similar breast cancer-specific survival in both age groups with HER2-positive breast cancer although none of the older patients received chemotherapy while 28% of the younger patients did. Furthermore, none of the patients received trastuzumab, which was nonstandard at the time of the study period [66].
A pooled analysis presented in 2013 of older women (over 60 years) from randomized controlled trials compared trastuzumab plus chemotherapy versus chemotherapy alone. This analysis showed a 47% relative risk reduction in those patients receiving trastuzumab, with a small (5%) risk of cardiac events [67].
Finally, there is limited literature available to comment on the use of adjuvant trastuzumab in combination with endocrine therapy or as monotherapy, which, due to the lower toxicity, could be a potentially important therapeutic strategy for older women with HER2-positive disease. The RESPECT trial is currently recruiting older women (70–80 years) to compare trastuzumab as monotherapy with the combination of trastuzumab and chemotherapy. The results are eagerly awaited.
Novel approaches
There are potential approaches in adjuvant therapies that may change the future of breast cancer therapy. A number of agents under investigations that target HER2 and other members of that receptor family are currently under development, such as lapatinib and pertuzumab, which hope to overcome the potentially serious adverse events found with trastuzumab and the emerging problem of resistance [68].
Geriatric needs & their impact
In addition to considering the different biology and its clinical relevance, specific geriatric needs are important when planning treatments for an older woman with primary breast cancer. Cancer care is undergoing a shift from disease-focused management to a patient-centered approach in which more attention is paid to psychosocial aspects, quality of life and patient individuality. Multidisciplinary teams emerge as a necessity for optimal coordination of these efforts. The drive towards the multidisciplinary approach in recent years has helped develop the concept of geriatric oncology [69–71].
An integrated onco-geriatric approach has emerged as a top priority within the international geriatric oncology community, focusing on the specific needs of elderly cancer patients related not only to their chronological age but to their biological age [72,73]. There are a few main areas of particular interest highlighted to this heterogeneous population: comprehensive geriatric assessment (CGA), functional decline, comorbidity evaluation and management and treatment outcomes [74]. These issues may present different management problems when compared with their younger counterparts.
CGA versus screening tools
There is still uncertainty in the literature regarding the interaction of geriatric conditions and treatment decision-making and also great variability in the measurement methods used to evaluate functional decline and comorbidity. Despite recognition that CGA is paramount in this setting, there is no consensus on a recommended assessment tool and how these results should be interpreted [71,75].
Comprehensive geriatric assessment is an investigative questionnaire aimed at assessing an older person's medical, psychological and functional capacity [75]. It provides additional information to the Eastern Cooperative Oncology Group performance status and detects health issues that may affect treatment outcome, contrary to the physician's judgement [76]. It consists of a combination of validated assessment tools regularly used in clinical practice, usually including: medical assessment of current health state including medications and nutritional status; assessment of physical function; psychological assessment of mood and mentality and social and environmental assessments. It can be used to improve diagnostic accuracy, plan treatment, and maintain functional capacity, independence and quality of life for the patient. It can also help coordinate care and reduce overall mortality. Furthermore, CGA may lead to better selection of patients for recruitment to clinical trials and in furthering research.
Disadvantages of CGA include its time-consuming nature and possible impediments in its completion [77], unique to the elderly population. There is currently a lack of consensus regarding when and to whom CGA should be implemented, which components should be included and how these results should be interpreted. This currently limits its use in every day practice. Despite these drawbacks there is growing evidence [78] for the use of CGA in oncology, including in the context of primary operable breast cancer in older women.
It may not be practical to implement CGA for every older woman with primary operable breast cancer, thus a method of screening may be considered to detect those patients who would benefit from further assessment in this manner. Examples of potential screening tools currently in use in geriatric oncology (not specific to the context of primary breast cancer at initial diagnosis) include: the abbreviated CGA called Geriatric-8 (G8), senior adult oncology program 2 questionnaire, triage risk screening tool, Vulnerable Elderly Survey-13 (VES-13) tool, Groningen Frailty Indicator Index (GFI) and onco-geriatric screening tool, as described and reviewed in detail by Extermann [79].
Baitar
Molina-Garrido and Guillen-Ponce [81] compared the Barber Questionnaire (BQ) and the VES-13 to select patients who may benefit from CGA. They recruited 41 women older than 65 years of age, diagnosed with early breast cancer in a single center. The correlation between BQ and CGA was fair (intraclass correlation coefficient 0.672) but between VES-13 and CGA was very good (intraclass correlation coefficient 0.814). Therefore, they proposed the use of the VES-13 screening tool, with implementation of CGA with an impaired VES-13 score.
Psychosocial, quality of life & patient preference
There are a number of issues distinct to the elderly population, particularly regarding a diagnosis of breast cancer, which cannot be measured by formal assessment [82]. These include patient psychology, quality of life and patient preferences. These may be determined by life experience, spiritual and psychological needs and many other factors of which importance may increase over time. Some patients may decide that their quality of life is more important than curative treatment alone. They may explore the option of no treatment at all, a drastic contrast to the thoughts of the younger population [83].
Model of care
Multidisciplinary team approach
The multidisciplinary team approach remains a popular and practical way to assess older women with primary operable breast cancer [70]. Important members of the team include oncologists, surgeons, geriatricians, breast care nurses, physiotherapists, occupational therapists, social workers, patients, and patient families. Usually the team meet at a dedicated time and place to discuss the ongoing investigations and management of a number of patients. This may not necessarily include participation of the patient and their family at the time of discussion. Thus it evolves the concept of a specialized clinic developed solely for older women with primary operable breast cancer [84]. This design involves meeting of members of the relevant disciplines (e.g., clinicians and specialist nurses), the patient and their family, in a dedicated clinic, available at every stage of the disease process, including diagnosis, treatment decision and follow-up. This is in contrast to the model of care based upon the consultation with the surgical or oncology team alone. Therefore it would be the responsibility of the surgeon or oncologist to deliver and detect potential geriatric problems, through traditional clinical assessment and/or the application of a screening or full CGA tool and refer at risk patients on to a geriatrician for assessment.
Another suggested model requires the primary care physician to administer the screening tool to their patients and refer them on to the geriatrician for assessment where needed [85]. The underlying factor that may ultimately decide the model of geriatric oncology delivery in individual centers is cost–effectiveness. This proposed model could potentially reduce the burden on the specialist surgeon or oncologist of discovering and managing geriatric conditions. Thus extra thought should be given by individual centers as to the most cost-effective method of geriatric oncology in addition to current service provision and this should include training of surgeons, oncologists, geriatricians and primary care providers where necessary.
Challenges & future perspective
The challenges in studying older women seem to be multidimensional. This unique population are more likely to have confounding issues such as poor health, poor performance status and a lack of social support. These factors can increase the difficulty in allowing the older population to take part in clinical trials.
Executive summary
A third of breast cancer develops in older women.
The aging population is growing.
Current literature suggests that women are ‘under’-treated.
Advancing age suggests differing biology of the tumor.
There are geriatric issues specific to the older population that would impact on their management.
Primary and adjuvant treatments should be based on a combined assessment of tumor biology and patient characteristics including geriatric needs and quality of life.
Surgery is the standard of treatment for primary operable breast cancer.
There is a high percentage of estrogen receptor-rich tumors in the older population, making primary endocrine therapy a very good alternative in some patients, notably those who are frail with significant comorbidities limiting their life expectancy.
Axillary dissection remains important in reducing regional recurrence, especially in patients where adjuvant systemic therapies (e.g., chemotherapy) are considered inappropriate.
Breast reconstruction appears to be less popular with advancing age.
Primary radiotherapy may be considered in those patients who have estrogen receptor-negative tumors and are not suitable for surgery.
Adjuvant radiotherapy, chemotherapy and endocrine therapy should be considered wherever appropriate.
Comprehensive geriatric assessment (CGA) may help to identify factors that could potentially impact on treatment decision, which may have gone undetected.
There is widespread variation in the components of CGA and how it is used in clinical practice.
There are a number of screening tools that could potentially identify candidates for CGA.
Other factors such as psychosocial well-being, quality of life and patient preference cannot be formally measured within CGA but are also important in assessing the patient.
A multidisciplinary team approach is encouraged as part of the ideal model of care.
The challenges in studying older women are complex, including the appropriateness of conventional methodology.
Research in this area is still ongoing, and should take into account of both tumor biology and geriatric needs.
To overcome these challenges, when new trials are designed, consideration should always be given to abandoning age limits, and to introducing stratification by age at the time of randomization [86]. Furthermore, where randomized controlled trials are not appropriate and/or feasible (which is especially true in trials involving the older population), other methods such as national data statistics and prospective audits should be considered as an acceptable alternative to acquire evidence [87].
To optimize the management of primary breast cancer in the elderly, a combined consideration of the biological distinctiveness of the tumor as well as the patient's specific geriatric needs should be explored, and this should form the basis of improving current clinical practice and furthering research in this area.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.