
Abstract
The risk of developing pericarditis is similar in men and women. However, systemic autoimmune diseases are more common in women and may determine an increased risk of recurrences and complications. Specific management issues for women with pericarditis include pregnancy and lactation. Relatively few data have been published on pericardial involvement during pregnancy, and major concerns of clinicians are related to management issues, especially medical treatment. Nowadays, the general outcomes of these pregnancies can be similar to that expected in the general population when carefully followed by dedicated multidisciplinary teams. The aim of this article is to review the management of pericarditis with a focus on gender-specific issues.
Pericarditis is relatively common in clinical practice and may present as an isolated disease or as a manifestation of a systemic disease [1,2]. Few epidemiological data have been published. A reported incidence is 27.7 cases per 100,000 population per year in an urban Italian area [3]. The clinical diagnosis of pericarditis is relatively easy and based on clinical criteria, while the etiology search is more challenging and difficult in the clinical setting. Most cases are classified as idiopathic using a conventional diagnostic approach in developed countries with a low prevalence of tuberculosis [4–6]. Systemic inflammatory diseases (SID) and postpericadiotomy or postinjury syndromes (5–10% of all unselected cases), neoplastic pericardial disease (5%) and tuberculous pericarditis (<5%) are the more common specific etiologies recorded in unselected series on pericarditis. The prognosis and the risk of complication are related to the etiology, and idiopathic cases generally have good outcomes [7]. Recurrent pericarditis is the most common complication of the disease affecting approximately 30% of patients with acute pericarditis [4,7].
There is no specific gender predisposition to pericarditis, although women may be prone to specific etiologies, such as autoimmune systemic diseases that predispose women to more recurrences and complications [8–10]. The aim of the present paper is to review the management of pericarditis in women. Specific gender issues include the management of pericarditis during pregnancy and lactation [11,12] will be reviewed. Potentially relevant studies published up to January 2012 were searched in BioMedCentral, the Cochrane Collaboration Database of Randomized Trials, ClinicalTrials.gov, EMBASE, Google Scholar, MEDLINE/PubMed and Scopus, including a comprehensive Medline search with the MeSH terms ‘pericarditis’ with and without sex limits. Articles were selected on the basis of their clinical relevance and potential impact on disease management, including either original papers or specific reviews. At present there are no updated international guidelines on the management of pericardial diseases beyond the 2004 guidelines issued by the European Society of Cardiology [8].
Etiology of pericarditis in women
Women are more commonly affected by specific forms of pericarditis related to SID. On this basis, female gender has been reported as a possible risk factor for a specific etiology in a prospective study on 453 patients with acute pericarditis (mean age 52, 46% women) [4,10]. Unfortunately, there are no specific data available on the different etiologies of pericarditis according to gender. Considering the overall population including males, a specific cause was found in 76 out of 453 patients (16.8%) in the cited study: autoimmune in 33 patients (7.3%), neoplastic in 23 patients (5.1%), tuberculous in 17 patients (3.8%) and purulent in three patients (0.7%). In a multivariable analysis, women (hazard ratio [HR]: 1.67) and patients with fever 38°C (HR: 3.56), subacute course (HR: 3.97), large effusion or tamponade (HR: 2.15), and failure of aspirin or of NSAIDs (HR: 2.50) were at increased risk of specific causes.
Cases with pericarditis related to SID are associated with more recurrences than idiopathic ones; on this basis, women may have more recurrences than men [10]. In a multivariable analysis, women (HR: 1.65) and patients with large effusion or tamponade (HR: 2.51) as well as failure of aspirin or NSAIDs (HR: 5.50) were at increased risk of complications. A list of possible poor prognostic predictors in acute pericarditis is reported in
The estimated incidence of pericardial involvement in more common SID is variable and reported in
Estimated frequency and type of pericardial involvement in more common systemic inflammatory diseases.
Major clinical poor prognostic predictors in acute pericarditis.
Fever >38°C
Subacute onset
Large pericardial effusion
Cardiac tamponade
Lack of response to aspirin or NSAIDs after at least 1 week of therapy
Adapted from [9].
Clinical presentation & diagnosis
Pericarditis maybe acute (first attack), recurrent and sometimes chronic with an arbitrary term >3 months.
Chest pain, usually pleuritic, is the more common reported symptom of pericarditis (
Symptoms and clinical findings at presentation in acute pericarditis (data based on personal unselected series).
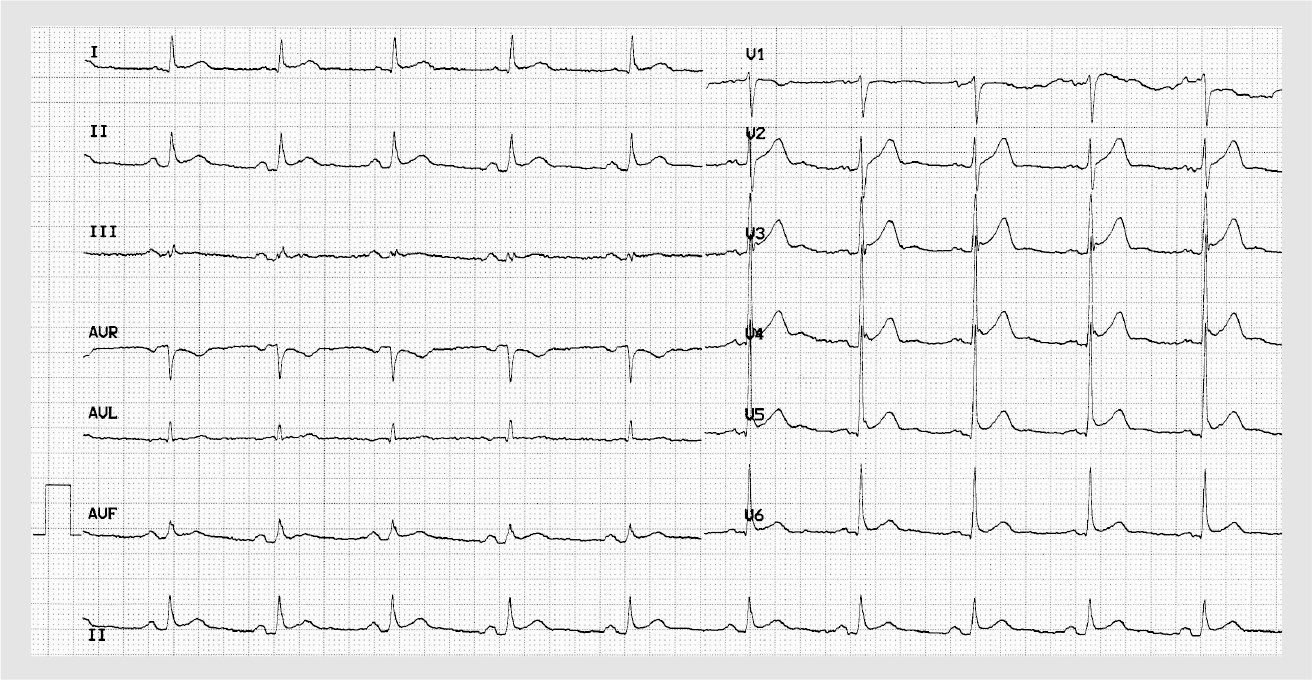
Diagnosis based on clinical findings supported by ECG.
Adapted from [15].
ECG changes include widespread ST-elevation and PR depression (usually the first ECG change) and are reported in most cases (
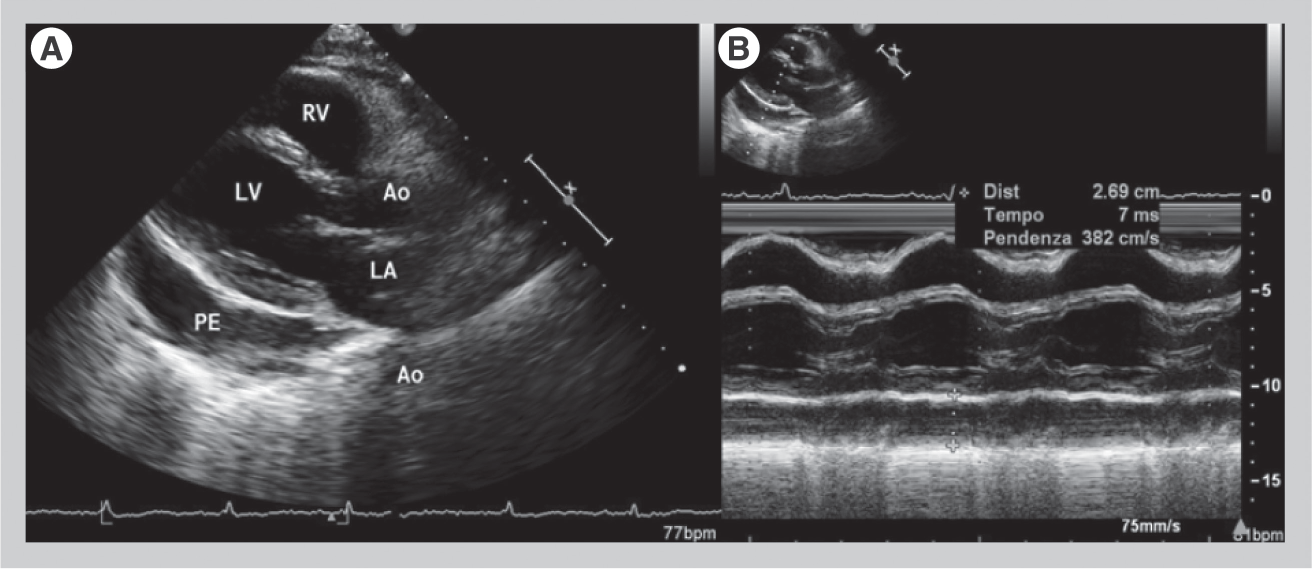
Echocardiography findings are generally nonspecific. A pericardial effusion has been reported in approximately a half of patients with acute pericarditis [9,15,16]. Transthoracic echocardiography allows a quick assessment of the presence and hemodynamic importance of pericardial effusion. In clinical practice a common semiquantitative classification of pericardial effusion is based on the estimation of pericardial effusion echo-free spaces at the onset of the QRS complex in diastole (
Gender-specific issues for management: pregnancy & lactation
The most common form of pericardial involvement is isolated pericardial effusion, which is usually a benign condition recorded by the third trimester in approximately 40% of pregnancies [12,17]. Acute pericarditis is the second most common form of pericardial involvement during pregnancy, although the exact frequency of the disease is unknown in the setting of pregnancy. Idiopathic pericarditis is the usual diagnosis in this setting, although a systemic autoimmune disease may be an alternative cause especially in cases with significant effusions or cardiac tamponade at the initial presentation, particularly for systemic lupus erythematosus [13]. During pregnancy, cardiac tamponade manifestations may be attenuated by the physiologic increase of blood volume. On this basis, a pregnant woman is usually able to better tolerate a large effusion compared with an age-matched nonpregnant woman. On the contrary, pregnant women are less tolerant in the case of initial constriction [17].
Other etiologies are less common. Tuberculosis is an important cause in developing countries, where the disease is often associated with HIV infection, as well as in immigrants. Neoplastic pericardial disease is rare, with breast cancer being the most common malignancy to be diagnosed during pregnancy, often at an advanced stage and with a high mortality [18].
Few data have been published on pericarditis during pregnancy. At present, the largest published series of pregnant women with acute pericarditis included only six women (mean age 30 years, mean gestational age at delivery 38 weeks and mean birth weight 2839 g), all with idiopathic etiology [11]. Four women were treated with 800 mg aspirin three-times daily.
Aspirin was stopped at 20 weeks in three women and continued until delivery in one case. All women were treated with prednisone at low to moderate doses; four women received prednisone throughout pregnancy, and two cases only during the third trimester. Five pregnancies (>80%) were uneventful, with one case of HELLP syndrome in the woman who continued aspirin until delivery. The HELLP syndrome refers to a syndrome characterized by hemolysis with a microangiopathic blood smear, elevated liver enzymes and a low platelet count, occurring in less than 1% of normal pregnancies [19]. All infants had a good outcome. Recurrences rates were similar to nonpregnant cases (20–25%) after a mean follow-up of 21 months. These data show that pregnancies complicated by pericarditis generally have a good prognosis with event rates similar to nonpregnant women. The outcome is more correlated to the underlying etiology rather than pericarditis itself.
The proposed treatment protocol included aspirin being gradually stopped at 20 weeks of gestation, plus low dosages of prednisone if needed throughout pregnancy and lactation (
Proposed treatment scheme for medical therapy of pericarditis during pregnancy.
Low-to-moderate doses are considered (<25 mg/day), usually from 2.5 to 15 mg/day.
Possible association with aspirin or a NSAID; the dose of aspirin of 100 mg/day or less is not useful as an anti-inflammatory therapy (colchicine is contraindicated except for familial Mediterranean fever). Paracetamol 500–1000 mg every 8–12 h is always allowed. Adapted from [12].
In regard to pericarditis, the reported outcome has been relatively better than that usually reported in nonpregnant women with a very low recurrence rate (<20%) [20]. This may be due to the fact that no corticosteroid tapering was attempted during pregnancy.
Diagnostic issues
During pregnancy the main diagnostic issue is to avoid diagnostic testing that may be harmful to the fetus, in particular avoiding exposure to radiation. Echocardiography remains the imaging method of choice for diagnosis, follow-up and guidance for pericardiocentesis [21]. As for the general population of pericarditis patients, high-risk features at presentation include large pericardial effusion, cardiac tamponade, and a lack of response to aspirin or a NSAID [4,14,22].
A positive result for antinuclear antibodies (ANA), often as a fortuitous observation, may be a cause for concern in idiopathic recurrent pericarditis; this nonspecific finding may occur during pregnancy or in nonpregnant women. In an Italian study, ANA were detected in 53 out of 122 (43.4%) patients with idiopathic recurrent pericarditis, and in only 12 out of 122 (9.8%) controls (p < 0.001). Low titers (one out of 40 to one out of 80) were found in the majority of cases, while moderate positivity (one out of 160 to one out of 320) was more common in patients with a known rheumatic disease (26.7 vs 5.7%; p = 0.020). Women were at increased risk for ANA (odds ratio: 2.22; 95% CI: 1.07–4.60; p = 0.033). During a mean follow-up of 32 months, complications and new diagnoses were similar in patients with or without ANA positivity. Routine serologic testing for ANA suggests a source for recurrent pericarditis in less than 10% of cases, and in these cases other evidence typically suggests the underlying disease [23].
Therapy issues
In patients with a previous history of pericardial disease, pregnancy should be planned in a phase of stable remission. Specific precautions include withdrawal of colchicine before conception, which is eventually substituted with aspirin and/or low-dose prednisone [24]. The appropriate therapy (i.e., high-dose aspirin plus low-dose prednisone) should be reached and tested before conception, and then continued throughout pregnancy, with aspirin gradually tapered around week 20. Nowadays, the general outcomes of pregnancies in these women can be similar to that expected in the general population. Dedicated multidisciplinary teams are recommended to provide careful assessment and follow-up.
As for the general population of pregnant women, all medications that are not necessary should be avoided. Current knowledge on drug safety during pregnancy and lactation is mainly based on animal data, human case reports and small series with inadvertent exposure. When pericarditis is treated in a pregnant woman the above recommendations should be considered.
NSAIDs
NSAIDs and aspirin are considered as first-line treatment in patients with pericarditis. These drugs can be continued until the second trimester [24] as nonselective COX inhibitors are not teratogenic and can be continued during the first and second trimester. There are no reliable data on selective COX-2 inhibitors, which should be avoided. After gestational week 20, all NSAIDs (except aspirin 100 mg/day or less) should be withdrawn because of possible constriction of the ductus arteriosus and impairment of fetal renal function. Most NSAIDs are excreted in small quantities into human breast milk. Several NSAIDs (i.e., ibuprofen, indomethacin, diclofenac, naproxen and piroxicam) are considered consistent with breastfeeding by the American Academy of Pediatrics [25]. Aspirin (>100 mg/day) should be considered with caution during breastfeeding because of potential adverse effects to the infant. Exposure to the infant may be reduced if these drugs are given after breastfeeding [12,24].
Corticosteroids
Corticosteroids are commonly used during pregnancy. Corticosteroids are metabolized by the placenta with different efficiencies. Prednisone is actively metabolized and only 10% of the active drug reaches the fetus [26]. On the contrary, dexamethasone and betamethasone are less metabolized and may reach higher concentrations in the fetus; for this reason they are used only for selected fetal indications (e.g., lung maturity induction and autoimmune congenital heart block). On this basis, prednisone is considered a category B drug in terms of its risk for pregnancy by the US FDA. Other corticosteroids are considered category C. Use of corticosteroids during pregnancy is associated with a three- to four-times increase in oral clefts.
Particularly during pregnancy, use of low doses of prednisone (i.e., 0.1–0.3 mg/kg/day) should be favored over higher doses because severe side effects are more common with high doses and may be responsible for more withdrawals, recurrences and disease-related hospitalizations according to a retrospective study on recurrent pericarditis, at present the largest available experience on this topic [27]. During pregnancy, specific feared corticosteroid dose-related side effects are hypertension, diabetes, premature rupture of membranes and prematurity, where prematurity is the first recognized cause of neonatal mortality and long-term neurological impairments in children. Breastfeeding is allowed during corticosteroid use, although high doses of corticosteroids should be postponed [12,24].
Colchicine
Colchicine has been traditionally prescribed for the treatment and prevention of gout attacks, but also for pericarditis management and prevention [28–32]. Colchicine has been recommended for the treatment of acute (class IIa recommendation) and recurrent pericarditis (class I recommendation) in the 2004 guidelines of the European Society of Cardiology based on experts consensus [8]. In the reported guidelines, the recommended therapeutic scheme included an attack dose with 2 mg/day for 1–2 days followed by 1 mg/day. Subsequent randomized studies have confirmed this indication, showing that colchicine may improve remission rates and symptoms resolution during the acute attack and may halve recurrence rates when used for several months [29,30,32]. Tolerability is improved avoiding the use of loading doses and starting with lower doses following weight-adjusted doses (i.e., 0.5 mg twice-daily for patients ≥70 kg, but only 0.5 mg once-daily for patients <70 kg).
Colchicine's anti-inflammatory mechanism of action is only partially known. The drug, even when used at low oral doses (0.5–1.0 mg/day), is able to concentrate in white blood cells, especially granulocytes, inhibiting tubulin polymerization and interfering with microtubule function, which in turn interferes with leukocyte function. The high concentration of colchicine in white blood cells exerts anti-inflammatory effects mainly related to the interference with microtubules. Colchicine may also interfere with the mitotic spindle, affecting cell division. This effect is related to the possible negative effects on fertility, pregnancy, breastfeeding or childhood [33]. Colchicine is a highly poisonous alkaloid with a narrow therapeutic index and fatalities have been reported after oral ingestion. The severity and the mortality rate of the poisoning is directly related to the ingested dose. Reported mortality rates are 10–50% with absorbed doses of 0.5–0.8 mg/kg and 100% with doses >0.8 mg/kg. Common toxicity symptoms include gastrointestinal symptoms at lower doses and initial stages followed by bone marrow aplasia, alopecia and circulatory failure in advanced cases with high doses. However, when carefully prescribed at low oral doses, the drug is safe and efficacious. No significant adverse events have been recorded on fertility, pregnancy or fetal or child development in familial Mediterranean fever even after prolonged use [34,35]. Although potential teratogenicity cannot be absolutely excluded based on animal research [33], and amniocentesis with karyoting has been recommended whenever colchicine is given during pregnancy [36], a recent Israeli paper has concluded that amniocentesis is no longer routinely recommended in these women [37]. Thus, colchicine is contraindicated during pregnancy and lactation beyond specific indications, such as familial Mediterranean fever [33,36,37]. Gradual drug withdrawal is recommended before pregnancy.
Immunosuppressive drugs
Other immunosuppressive drugs are rarely indicated in recurrent pericarditis [9,38]. Use of these treatments requires appropriate knowledge and cooperation with different specialists. Among these drugs, methotrexate and cyclophosphamide are absolutely contraindicated and should be stopped 3 months before pregnancy, while other drugs (i.e., azathioprine, intravenous immunoglobulins-IVIG and cyclosporine) may be used in selected cases.
Although rarely indicated, surgical therapies (i.e., pericardiotomy and pericardiectomy) could be performed without risk for subsequent pregnancies [39].
Future perspective
Management of pericardial diseases is becoming increasingly evidence based because of the growing number of clinical researches and trials [4o]. However, further basic and clinical research is needed to improve the understanding of the pathophysiology of pericarditis, especially for recurrences, and to improve diagnostic tools to better address the etiologic search in order to develop targeted therapies. In addition, further clinical trials and prospective cohort and case–control studies are going to provide additional data on indication, dosing and treatment lengths in order to have more evidence based approaches to therapies [9]. Additional case series and registries on pericardial diseases during pregnancy are needed to improve the management of these conditions, since this condition has been excluded in clinical trials or is only poorly reported in current available literature.
Executive summary
Pericarditis is relatively common in clinical practice and may present as an isolated disease or as a manifestation of a systemic disease.
The clinical diagnosis of pericarditis is relatively easy and based on clinical criteria, while the etiology search is more challenging and difficult in the clinical setting, and most cases are classified as idiopathic using a conventional diagnostic approach in developed countries with a low prevalence of tuberculosis.
There is no specific gender predisposition to pericarditis, although women may be prone to specific etiologies, such as autoimmune systemic diseases that predispose women to more recurrences and complications.
Pericarditis may be acute (first attack), recurrent and sometimes chronic with an arbitrary term of >3 months. Chest pain, usually pleuritic, is the most common reported symptom of pericarditis, and usually the main cause of presentation.
Specific conditions to be ruled out include myocardial ischemia, pulmonary embolism, aortic dissection, pleuritis, pneumothorax, gastroesophageal reflux disease and musculoskeletal pain.
Gender-specific issues for pericarditis management in women include pregnancy and lactation.
Acute pericarditis is the second more common form of pericardial involvement during pregnancy after isolated pericardial effusion, which is usually a benign condition recorded by the third trimester in approximately 40% of pregnancies.
Idiopathic pericarditis is the usual diagnosis in this setting, although a systemic autoimmune disease may be an alternative cause especially in cases with significant effusions or cardiac tamponade at the initial presentation.
For pregnant women the diagnostic approach is aimed at reducing useless investigations that may be harmful for the fetus, especially avoiding the exposure to radiation. ECG is the imaging method of choice for diagnosis, follow-up and guidance for pericardiocentesis.
After gestational week 20, all NSAIDs (except aspirin at less than 100 mg/day) can cause constriction of the ductus arteriosus and impair fetal renal function and should be withdrawn in any case at gestational week 32. Low-to-medium doses of prednisone are allowed during all pregnancy and breast feeding. Colchicine is generally contraindicated during pregnancy, except in patients with familial Mediterranean fever or other compelling indications.
Footnotes
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.