
Abstract
Osteoporotic fracture is associated with considerable morbidity and mortality in women throughout the world. However, significant variation in hip fracture rates among women from different nations has been observed and is likely to represent a combination of real and apparent differences due to ascertainment bias. Higher rates are observed in Caucasian women, with lowest rates observed in black women and intermediate rates among Asian women. These differences are likely to represent a combination of genetic and environmental differences; for example, among European women, the highest fracture rates are observed in Scandinavian women where vitamin D insufficiency is common. In all groups, an increase in absolute fracture numbers is anticipated due to demographic changes.
Osteoporosis is a skeletal disorder characterized by low bone mass and microarchitectural deterioration of bone tissue with a consequent increase in the fragility of bone [1]. It represents a major public health problem through its association with low trauma fractures. These fractures increase dramatically with age and are more frequent in women than men. The most common fracture sites are the hip, spine and distal forearm. These fractures represent the most serious outcome of the condition and lead to severe morbidity and mortality, and are a significant burden on society in general, causing a huge impact economically. Osteoporotic fractures alone cost the USA approximately US$17.9 billion per annum and the UK approximately GB£1.7 billion [2].
This review aims to explore the geographic variation and secular trends of fragility fractures (with a particular emphasis on hip fracture) in postmenopausal women, within the methodological limits of comparing data drawn from different countries, where fracture ascertainment may be influenced by, for example, ICD coding or databases used. The studies included in this review were identified through a PubMed search that included the keywords: ‘osteoporosis’, ‘fracture’, ‘geographic,’ ‘variation’, ‘women’ and ‘epidemiology‘.
Definition of osteoporosis
Traditionally, osteoporosis has been defined in women as a bone mineral density (BMD) value of more than 2.5 standard deviations below the young normal mean [3], with osteopenia being defined as BMD levels between 1 and 2.5 standard deviations below the young normal mean. However, this definition does not consider any of the microarchitectural changes that may weaken the bone independently of any effect on BMD [3]. More recently, in a move to incorporate the strongest risk factors for fracture and to make results more intuitive for patients and clinicians, BMD results can now be incorporated into an assessment of individualized 10-year absolute fracture risk through the WHO FRAX tool [4]. This has the advantage of including risk factors that are partly independent of BMD, such as age and previous fracture, to more accurately predict outcome.
Global observations regarding incidence & prevalence of osteoporosis
Osteoporosis-related fractures are a great healthcare burden, as highlighted by the US Surgeon General 2004 report [5]. An estimated 10 million Americans over 50 years of age have osteoporosis and another 34 million are at risk of the disorder. This is likely to increase to over 14 million in 2020. There are an estimated 1.5 million fragility fractures each year. The lifetime risks of osteoporotic fracture for women aged 50 years or over are 17.5% for hip fracture, 15.6% for clinically diagnosed vertebral fracture and 16% for distal forearm fracture.
The UK population fracture risk, based on data from the General Practice Research Database in the UK [6], is similar to that in the USA. A half of women will have an osteoporotic fracture in their lifetime. The majority of these will be hip, vertebral or wrist fractures. The lifetime risk of hip fracture is 14% for women and rates of radiographic vertebral fracture are somewhere between one-quarter and one-third. Finally, one in eight women will suffer a wrist fracture at some point in their life.
Global observations regarding age variation in fracture incidence & prevalence
Peak bone mass is generally achieved by the age of 30 years. Thereafter, bone density progressively falls with age and, consequently, the prevalence of osteoporosis thus increases. While most white women under the age of 50 years have normal bone density, by the age of 80 years 27% are osteopenic and 70% are osteoporotic at the hip, lumbar spine or forearm [7].
Fracture incidence is bimodal. There are peaks in childhood and in the elderly. In young people, fractures may follow significant trauma and predominantly affect long bones. In the elderly, by contrast, fractures are typically due to minor or moderate trauma. They usually occur following falls from the standing position, but have been known to occur spontaneously. The incidence of fractures of the hip, vertebrae and wrist is greater in elderly women than in elderly men [8].

Epidemiology of hip fracture
Hip fracture incidence increases exponentially with age, with approximately 90% affecting people over 50 years of age [9]. Worldwide, it is estimated that 1.66 million hip fractures occurred in 1990 and includes 1,197,000 fractures in females. The total figure is predicted to rise to 6.3 million by 2050 owing to an increasing number of elderly people in the population [10]. Above 50 years of age, there is a female:male incidence ratio of approximately 2:1 [11]. In the UK, the 10-year risk of hip fracture is 0.3% for a 50-year-old woman and 8.7% at the age of 80 years [6]. In addition to increased skeletal fragility observed with aging, the risk of falling also rises with advancing age. The direction of falling is important; a fall laterally onto the hip has a greater likelihood of resulting in a hip fracture than falling forwards [12]. In women aged 40–49 years, approximately 20% will fall each year. This figure rises to 50% of women over 85 years of age, highlighting fall prevention as one important component of fracture prevention [13].
Epidemiology of vertebral fracture
Most vertebral fractures are asymptomatic. Only approximately one-third of all vertebral deformities noted on radiographs come to medical attention. As a result, in studies using radiographic screening of populations, the incidence of all vertebral deformities has been found to be even higher than that for hip fracture [14,15].
A study carried out in Rochester (MN, USA) showed that the age-adjusted incidence of clinical vertebral fractures in women is almost twice that in men [14]. Data from the EPIDOS study also demonstrated an increased prevalence of vertebral fractures in women, with figures rising from 19% among women aged 75–79 years to 41.4% among those aged 85 years and older [16]. In the EVOS, vertebral deformities were noted in approximately one in 20 women aged 50–54 years. While far fewer data are available describing geographic variation in vertebral than hip fracture, findings from the EVOS study will be described later in this review.
Epidemiology of the wrist & other fractures
Wrist fractures show a pattern of occurrence which differs from that of hip and vertebral fractures. There is an increase in incidence in white women between the ages of 45 and 60 years, followed by a plateau (
Proximal humerus, pelvis, proximal tibia and distal femur fracture incidences increase with age and are linked with low bone density [17]. The incidence of proximal tibia fractures is bimodal with peaks in the young and in the elderly [18]. Very few data are available describing geographic variation in wrist fracture.
Morbidity & mortality associated with osteoporotic fracture
Morbidity
Many of those who sustain a fragility fracture are left with long-term impairment: in the USA approximately 7% of survivors of all types of fragility fractures have a degree of permanent disability and 8% end up requiring long-term nursing homecare. Overall, after any type of fracture, a 50-year-old US white woman has a 13% chance of experiencing attributable functional decline [19].
Following a hip fracture, patients are at risk of acute complications. These include urinary tract infections, pressure sores and bronchopneumonia. The degree of functional recovery after hip fracture is age dependent. Fourteen percent of 50–55-year-old patients require nursing home care following discharge from the hospital, and this figure is more than 50% in those over the age of 90 years [20]. Premorbid status is also a strong predictor of outcome. In the USA, 25% of formerly independent people became at least partially dependent, 50% of those who were dependent prefracture were admitted to nursing homes and those who were already in nursing homes remained there [21].
Despite only a minority of vertebral fractures coming to clinical attention, they account for approximately 52,000 hospital admissions in the USA and 2188 in England and Wales each year in patients aged 45 years or over. The major clinical consequences of vertebral fracture are back pain, kyphosis and height loss [20]. This can be associated with functional loss and lead to depression, loss of self-esteem and social isolation. Participants in the EPOS, with radiologically identified vertebral fracture at baseline, had repeat radiographs performed 3 years later. Women who had suffered a further fracture during this period experienced substantial levels of disability with impairment in key physical functions of independent living [22].
Wrist fractures may impact on some activities such as writing, washing and dressing. Overall few patients are completely disabled, but after 6 months, half of patients still report poor function. In addition, complications such as reflex sympathetic dystrophy, neuropathies and posttraumatic arthritis are not infrequently seen [20]. There is a shortage of epidemiological studies reporting long-term outcome after these fractures, with most studies reporting outcome after different orthopedic procedures to reduce and stabilize fractures.
Mortality
People who sustain hip or vertebral fractures have increased mortality rates compared with those without fractures. Survival rates 5 years after a hip or vertebral fracture in Rochester were found to be approximately 80% of those expected for women of similar age without fractures [23].
Hip fracture mortality increases with age and is greater for those with poor prefracture functional status and coexisting illnesses [24]. In the USA, approximately 3% of women aged over 50 years die during the initial admission. Mortality rates after hip fracture continue to rise over the subsequent months and peak at 1 year with a rate of 21% [25]; studies from the UK show similar rates [6]. The risk of death is greatest immediately after the fracture and decreases gradually over time. The elevated risk has been shown to persist for up to 10 years [26]. In only 25% does the cause of death occur directly due to the fracture itself or resulting complications, such as infection, thromboembolic disease or surgery [27]; in the remaining majority, it is attributable to coexisting morbidity due to underlying diseases.
The increased mortality after vertebral fracture persists for up to 5 years [23,26]. In the UK Global Practice Research Database study, survival at 1 and 5 years postvertebral fracture were 86.5 and 56.5%, respectively. This was markedly lower than the expected levels of 93.6 and 69.9%, respectively [6].
Geography & ethnicity: an overview
The remainder of this review will focus on what is known regarding geographic variation in hip fracture rates among women and how secular changes in fracture rate vary by region. It is well known that there are considerable variations in fracture rates depending on geographic area and race, with lower rates observed in black than in Caucasian or Asian populations. In general, people who live in latitudes further from the equator seem to have a higher incidence of fracture. The highest rates of hip fracture are seen in Caucasians living in northern Europe, especially Scandinavians. The rates are intermediate in Asia [28], China [29] and Kuwait [30], and lowest in black populations [31]. Generally, when hip fracture risk is high, there is a propensity for this to be reflected by high levels of other fragility fractures in the same area [32,33].
Kanis et al. determined the 10-year probability of hip fracture standardized for gender and age in 29 separate countries [34]. Large differences were found in the 10-year probability of hip fracture between countries.

Variations between estimates of incidence trends throughout the world are summarized in
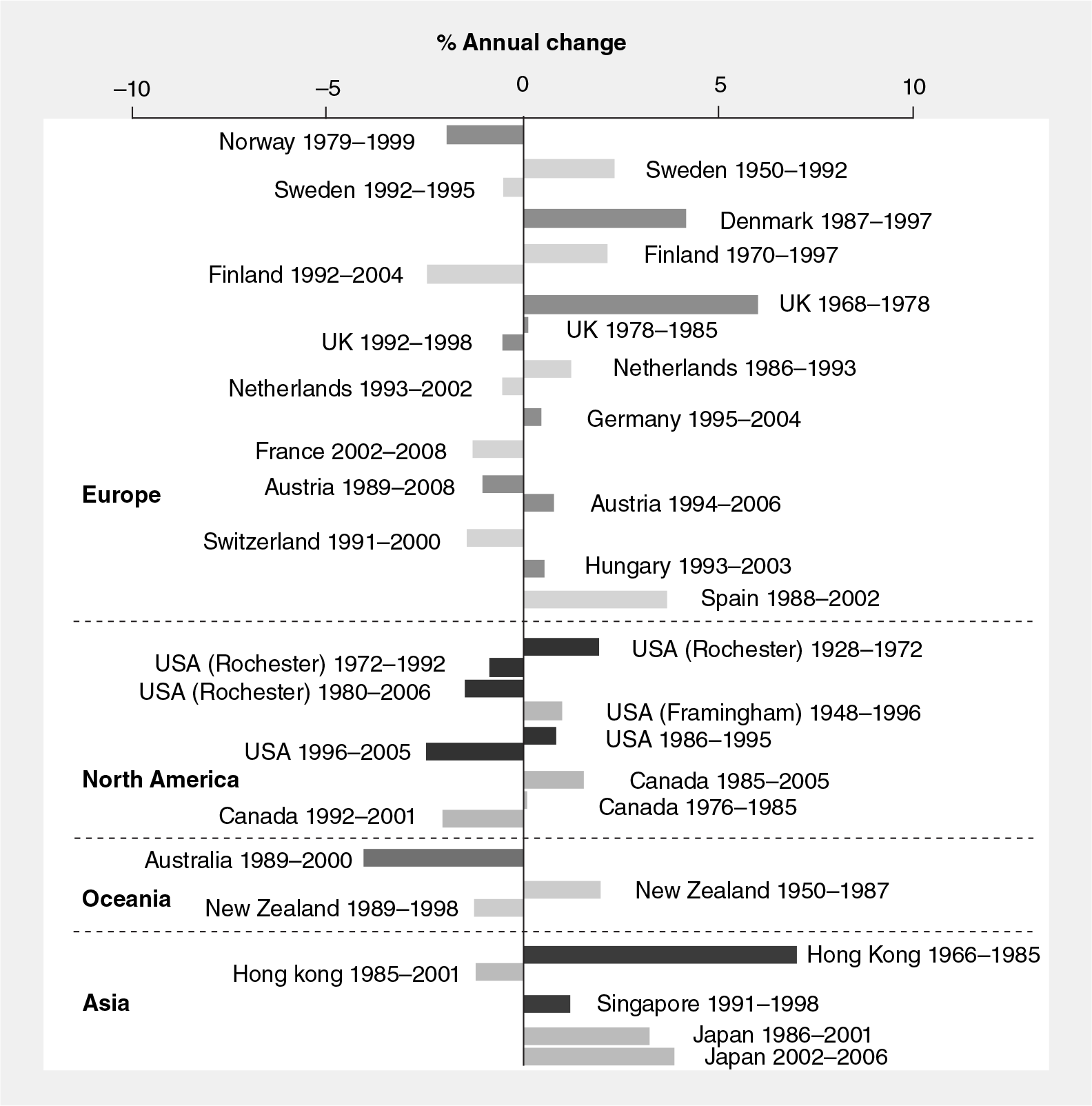
North America
The USA has some of the highest fracture rates in the world. Age-standardized incidence of hip fracture has been reported to range from 511 to 553 per 100,000 person-years in women [38]. These rates have plateaued over the last 20 years and in some areas have been observed to decrease. Data from Rochester suggest that age-adjusted hip fracture incidence rates initially began stabilizing from around 1955 [39] and fell between 1980 and 2006 [40]. In addition, in those over 65 years of age, Brauer et al. noted a change in trend in the age-adjusted hip fracture incidence over several decades [41]. It increased by 9% from 1986 to 1995 and, subsequently, significantly declined by 24% from 1995 to 2005. The decline corresponded to an increase in bisphosphonate use among participants. The annual mean number of hip fractures per 100,000 person-years in this age group was 957.3 for women [41]. When the age-adjusted incidence of hip fractures among white women aged over 65 years, according to their county of residence in the USA, were calculated, rates were found to be higher in the south than the north and in those counties with a larger proportion of those over 65 years of age below the poverty line [42].
The difference in hip fracture rates among ethnic minorities in the USA has also been studied. Zingmond et al. reported that in those over 55 years of age, between 1983 and 2000 the age-standardized hip fracture incidence fell by 0.6% per year in non-Hispanic white women [43]. By contrast, in women of Hispanic ethnicity these figures rose by 4.9 %. No significant change was reported among black or Asian women. While these observations might be explained by differences in physical activity and risk of nutritional deficits between the populations, an alternative explanation relates to variations in environment during growth and development.
It has been suggested that a birth cohort effect may also be operating in the Framingham Study, a population-based cohort studied from 1948 to 1996 [44]. Researchers demonstrated rates of hip fracture 20 and 40% higher among women born from 1901 to 1910 and from 1911 to 1920, respectively, compared with those born by 1900. Such an effect has also been reported in European studies and points to etiological factors acting early in the lifecourse [45,46].
Between 1945 and 1994, age-adjusted incidence rates of distal forearm fracture increased, on average, by 0.5% per year in Rochester [47]. In women, the age-adjusted rate peaked in 1975 and declined thereafter. This is similar to the trends shown for hip fracture in the same population. In contrast to hip and distal forearm fracture, there was no overall increase in clinically ascertained vertebral fracture incidence rates, when evaluated between 1950 and 1989 [48].
In Canada, hip fracture rates are significantly lower than observed in the USA. In a population-based study in Canada, the age-standardized incidence of hip fracture per 100,000 person-years was 86.4 in women [49]. Overall fracture rates were almost 30% lower in Canadians compared with Americans who were over 80 years of age. Despite the marked differences mentioned above between Canada and the USA, trends in hip fracture incidence are similar. Age- and sex-adjusted rates tended to be stable throughout the 1980s and early 1990s, with a subsequent gradually increasing decline [50,51].
A Mexican study in 2005 estimated the annual rate of hip fracture at 169 per 100,000 person-years among women [52]. These rates of hip fracture are lower than the USA, similar to southern countries in Europe, but significantly higher than in Canada. In contrast to the USA and Canada, data from Mexico show an age-adjusted incidence increasing by approximately 1% per year between 2000 and 2006 [53].
South America
Limited data are available from South American countries. Reira-Espinoza reviewed data from Latin America and reported hip fracture incidence per 100,000 persons that ranged between 263 and 304 in community studies and between 40 and 362 in hospital-based studies [52].
In Argentina, age- and sex-standardized incidence of hip fracture per 100,000 person-years among women has been reported to range from 259.6 to 405.0 [54–57]. Of environmental factors that may contribute to the differences observed in hip fracture incidence, climate differences between regions, which may lead to differences observed in vitamin D levels of their population, may be important [58]. Plasma vitamin D levels in the elderly are increased by sun exposure [59] and vitamin D insufficiency raised fracture risk [60]. Thus, lower vitamin D levels in those further from the equator may play a role, as may physical activity; a lower incidence of hip fracture observed in the study among women from a predominantly rural area may represent a more physically active lifestyle. Such an effect was also reported in European studies [61,62].
In Chile, the incidence of hip fracture at the age of 80 years of age was one of the lowest reported in the world. The annual mean number of hip fractures per 100,000 person-years in this age group was 119 for women. By contrast, in Venezuela, this rate was 381 per 100,000 person-years; and in Argentina 1432 per 100,000 person-years) [34]. It is important to consider the possibility of ascertainment bias when interpreting fracture rates between countries measured in different studies, where different health reporting systems operate.
Europe
There have been a large number of studies investigating incidence rates of hip fracture in Europe. The incidence rates vary in southern and northern Europe, with the highest rates observed in Sweden and Norway, and the lowest in France and Switzerland.

The variation in hip fracture incidence in women across Europe in the late 20th century.
Scandinavia has the highest reported hip fracture incidence worldwide. In Oslo, Norway, the reported age-standardized annual incidence rate of hip fracture during 1996–1997 was 1180 per 100,000 in women [64]. In those over 80 years of age, these rates rise steeply to 1665 [34]. Studies from Norway and Sweden have shown a lower bone mass among Scandinavian women compared with other European populations [65], but this difference does not fully explain the greater fracture rates in these countries. Within central Norway, significant differences between rates in rural and urban settings have also been identified [66].
Epidemiological data from Scandinavian countries indicate that in early studies, dating from the 1950s, there was an increasing hip fracture incidence; these rates appear to have fallen in the last two decades. Studies from Sweden reported an increase in age- and sex-adjusted incidence of hip fracture between 1965 and 1980, and 1950 and 1985 [67,68]. In Malmo, Sweden, between 1992 and 1995, these figures plateaued [69]. Giversen also reported a steep increase in the incidence rate of hip fracture in Viborg county, Denmark, observed between 1987 and 1997 [70]. Similar trends were observed in Finland where the age-adjusted hip fracture rate per 100,000 person-years increased from 292 to 467 in women between 1970 and 1997 [71].
In general, hip fracture rates in southern Europe are lower than in the rest of the continent. In Sienna, Italy, the overall incidence of hip fracture between 1980 and 1991 was 157 per 100,000 persons [72]. In Spain, between 1988 and 2002, there were no significant changes in age-adjusted incidence rates among women [73]. Some of the lowest incidence rates in Europe are found in Switzerland and France, with the former having age-standardized annual incidence rates of hip fracture per 100,000 of only 346 in women.
In Hungary, the reported rates of hip fracture between 1999 and 2003 were 430 per 100,000 in women [74]; during this period rates remained stable. Interestingly, in neighboring Austria, these figures were higher and rose from 637 to 759 [75]. In The Netherlands, the age-adjusted incidence of hip fracture increased in a linear fashion between 1972 and 1987 [76]. Rates then stabilized and began to fall [77]. In Germany, in women between 40 and 74 years of age, there was a similar period of stabilization before the rates began to decrease [78]. However, in those above 75 years of age, rates continued to increase. The increase was significantly higher in eastern compared with western Germany. The potential explanation for the high incidence rate of hip fractures in the oldest age groups may be the lack of a structured nationwide osteoporosis prevention approach in this country.
The incidence of hip fractures in the UK is shown in detail in
Some data are also available for geographic variation in vertebral fractures among Europeans; the EVOS study showed a threefold difference in prevalence of vertebral deformities between countries, with the highest rates again in Scandinavia [82]. The prevalence range between centers was 6.2–20.7% for women. Some of these variations could be explained by BMI and physical activity levels.
Asia
Hip fracture data are available from several areas in Asia and demonstrate considerable variability, with the highest rates observed in Singapore and Hong-Kong, and the lowest in central China.


In Singapore, in those above 50 years of age, age-standardized incidence of hip fracture rates between 1991 and 1998 were 402 per 100,000 persons in women [84]. When these values were compared with those derived in 1965, an increase in age-adjusted hip fracture rate of around 1–1.5% per year was reported. Interestingly, there were statistically significant racial differences with the highest rates among the Chinese, intermediate in Indians and the lowest in Malays; mean rates of fracture for these women when above 50 years of age were 410, 361 and 264 per 100,000 person-years, respectively. Time trends varied between different ethnic groups; an increase in hip fracture rates have been seen in Chinese and Malays, while rates in Indians appear to have decreased. Factors which may be responsible for these racial differences include bodyweight, physical activity, cigarette smoking, alcohol consumption and nutrition.
In the Tottori prefecture (Japan), the hip fracture incidence rate per 100,000 person-years after the age of 35 years was 368 in women [85]. There are limited data available from the Middle East. In Iran, studies using the Iranian Multicenter Study on Accidental Injuries report age-standardized hip fracture incidence rates per 100,000 person-years of 164.6 in women [86]. In Kuwait age-standardized rates per 100,000 person-years for hip fractures were 295 among Kuwaiti women and 374 among expatriates, who predominantly originate from southeast Asian and Arab countries [87].
Africa
There is a dearth of data from Africa, but those studies available suggest that fragility fracture rates are low. In Cameroon, the annual incidence of hip fracture per 100,000 persons in women above 35 years of age was 4.1 [88]. Similarly low fracture rates have been reported in Morocco in 2005 [89]. It appears that fracture rates in African counties are much lower than the western population. It is possible that the low rates of fracture documented are due to under-reporting owing to a lack of the necessary infrastructure.
Oceania
In both New Zealand and Australia the fracture incidence rates are comparable with those seen in Europe and North America. In New South Wales (Australia), between 1990 and 2000, the age-adjusted rate of hip fractures was reported at approximately 390 per 100,000 person-years in women [90]. During the period studied, the overall rates of fracture remained unchanged. Pelvic fracture data, from the same region, however, showed that the age-standardized hospitalization rate increased by approximately 50% from 1988 to 2000 [91]. Another Australian study, analyzing fracture rates in a suburban area to the northwest of Sydney between 1989 and 2000 showed that age-adjusted rates of hip fracture were declining [92]. Recent work using the Geelong Osteoporosis Study to examine possible reasons for a falling hip fracture rate among Australian women aged 75 years or over suggested that increasing adiposity and a consequent rise in BMD, and increased uptake of bone-active agents may be possible explanations [93]. Researchers working with the Geelong Osteoporosis Study have also recently demonstrated lower hip fracture rates in rural communities when compared with urban areas, which could not be accounted for by fracture ascertainment bias [94]. In New Zealand, age-adjusted rates for hip fracture increased significantly between 1950 and 1987 [95] before subsequently stabilizing. These overall trends are similar to those in Europe and North America.
Conclusion
Currently, approximately half of all hip fractures among elderly people occur in populations living in Europe and North America; however, hip fracture rates are falling in these populations, with observed decreases much too large to be explained by the use of antiosteoporotic medication [96]. In Sweden, where, traditionally fracture rates have been high, the age-standardized hip fracture incidence has decreased since 1996, more than counteracting the effects of the aging population and resulting in a decline in the annual number of hip fractures during the period of 1999–2002 [97]. Current projections suggest that this proportion of hip fractures seen in Europe and North America will fall to around one-quarter in 2050, when rapid increases in hip fractures rates will be seen in Asia and Latin America due to a combination of an aging population and secular trends in fracture rate. Several recent reports have highlighted the observation that the greatest increase in the number of osteoporotic fractures is likely to be in the Middle East, Asia and Latin America, where life expectancy will increase the most in the coming decades. Variation in fracture rates across nations represent a combination of genetic and environmental factors, many of which remain poorly elucidated. The association between socioeconomic status and fracture, if any, is unclear, but a recent systematic review has suggested that educational attainment was positively associated with BMD among women; further work is clearly needed in this area [98].
Future perspective
Over the next 5 years, we will see an increase in knowledge reagarding global epidemiology of osteoporotic fracture; it is to be hoped that much of the new data will come from areas of the world where few studies have been currently performed, including healthcare costs attributable to fracture in these populations. In a recent analysis, patients with osteoporosis-related fractures were found to incur an estimated nearly $10,000 in direct healthcare costs in the 6 months post-fracture compared with patients with no fracture, in a population identified from a commercially insured population with integrated medical and pharmacy claims [99]. From this research, an accurate picture of the size of the problem affecting all ethnic groups can be obtained and strategies developed to counteract this in the future.
Financial & competing interests disclosure
C Cooper has received honoraria and consulting fees from Amgen, Eli Lilly, Medtronic, Merck, Novartis and Servier. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Executive summary
Osteoporosis is a major public health problem.
Although osteoporosis is defined in terms of low bone density, 10-year fracture risk assessment tools are increasingly being used to further individualize fracture predictions.
Osteoporotic fractures are common, with approximately half of UK women developing one during their lifetime.
Osteoporosis prevalence increases with age, but fracture incidence is bimodal.
Hip fracture incidence increases exponentially with age.
Approximately two-thirds of vertebral fractures are asymptomatic.
Wrist fracture incidence increases between the ages of 45 and 60 years and then reaches a plateau.
Hip and vertebral fractures are associated with reduced survival rates at 5 years.
Hip fracture rates vary significantly around the world.
Scandinavia has the highest age-standardized rates of hip fracture in Europe.
Hip fracture rates are of similar magnitude in North America, Oceania and Europe.
Age-standardized rates of hip fracture are low in Africa; this may be due to under-reporting.
In many western countries, fracture rates increased over the second half of the 20th century and have since plateaued or begun to decrease.
The burden of fractures is likely to shift from Europe and North America towards Asia and Latin America over the next 40 years.