
Abstract
Noncardiac chest pain (NCCP) is very prevalent in the community. Although mortality remains low, morbidity and the financial implications are high, Women, especially those of middle age, should be thoroughly investigated as per current guidelines for coronary artery disease before labeling their chest pain as NCCP. Gastroesophageal reflux disease is the most common cause of NCCP; however other esophageal pathology including esophageal hypersensitivity, neuromuscular disease and eosinophilic esophagitis may also cause NCCP. Proton pump inhibitors are commonly used initially to manage NCCP, although patients who do not respond to this therapy require further investigation and differing treatment regimes. This article will focus on current knowledge regarding Gl tract-related NCCP management strategies.
Keywords
 Medscape: Continuing Medical Education Online
Medscape: Continuing Medical Education Online
This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education through the joint sponsorship of Medscape, LLC and Future Medicine Ltd. Medscape, LLC is accredited by the ACCME to provide continuing medical education for physicians.
Medscape, LLC designates this Journal-based CME activity for a maximum of
All other clinicians completing this activity will be issued a certificate of participation. To participate in this journal CME activity: (1) review the learning objectives and author disclosures; (2) study the education content; (3) take the post-test with a 70% minimum passing score and complete the evaluation at www.medscape.org/journal/wh; (4) view/print certificate.
Learning objectives
Upon completion of this activity, participants should be able to:
Analyze the epidemiology of noncardiac chest pain among women
Assess outcomes of coronary artery disease among women
Evaluate the role of gastroesophageal reflux disease in noncardiac chest pain
Compare different treatments for gastroesophageal reflux disease in the setting of noncardiac chest pain
CME Author
Authors and Disclosures
Editor
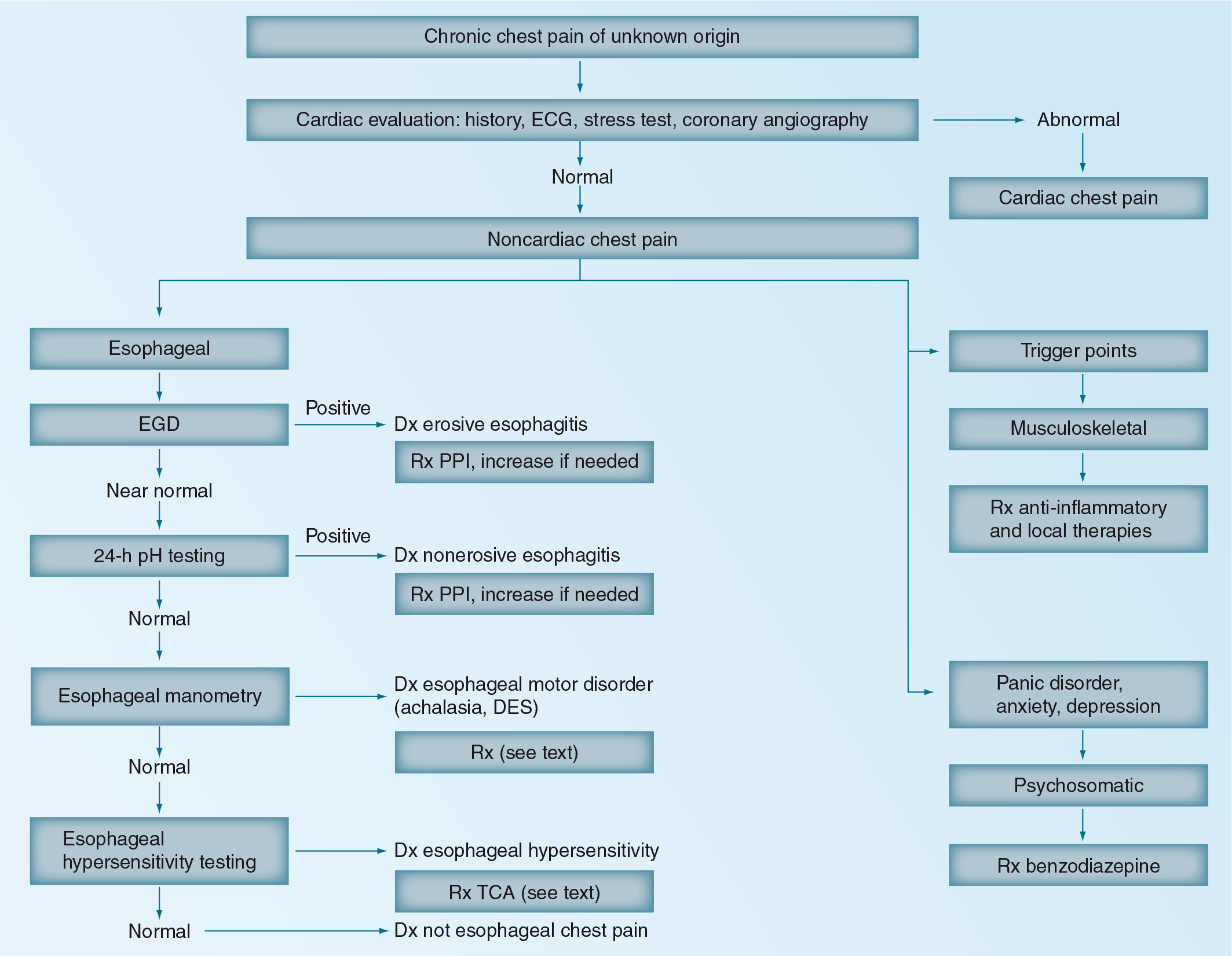
Noncardiac chest pain (NCCP) is defined as recurring substernal chest pain of noncardiac origin. It may be of musculoskeletal, pulmonary, gastroenterological, psychosomatic or neurological etiology. As the symptoms can be indistinguishable from ischemic heart disease, a thorough cardiological evaluation is required. Up to 30% of coronary angiograms performed in the USA are normal or have an insignificant degree of obstruction [1].
NCCP is very common, with an observed prevalence varying from 14 to 33% in different population-based studies [2–4]. NCCP affects both genders; middle-aged women have a significantly higher prevalence of NCCP compared with men [3]. Caucasians are more likely to report chest pain symptoms when compared with African–Americans [5]. NCCP patients are younger, consume more alcohol, smoke more often and are more likely to suffer from anxiety [6]. A recent study observed that women have increased NCCP symptoms during pregnancy (9%) as opposed to the year before conceiving (2%) [7].
NCCP patients frequently utilize healthcare resources, resulting in a high economic burden [8]. Patients are often not reassured by investigations; in a study of patients suffering from NCCP, 44% believed they had heart disease in spite of a normal angiogram [9]. There is some evidence that the process of investigation itself may entrench the mistaken idea of cardiac disease [10]. NCCP causes a high personal economic and psychological toll as a half of the patients remain or become unemployed, a half remains on cardiac medications and approximately 75% continue to experience pain [11]. NCCP has a significant negative impact on patients' quality of life and social well being [12].
Chest pain & coronary artery disease in women
Coronary artery disease (CAD) is the leading cause of death among women in the USA, with 233,886 deaths recorded in 2003 [13]. The risk for in-hospital mortality in women with postacute myocardial infarction (MI) was 20% greater than for men after adjusting for covariates [14]. Clinical trials commonly under-represent women and there may be gender differences in therapeutic responses that need to be further investigated in trials involving a larger representation of women [15]. In a recent large study of 125,161 patients in the USA, of which 50,162 (40%) were female, women aged 40–60 years had a 3.5% longer time to presentation than men despite adjusting for possible confounders. This demonstrates a significant gender gap remaining despite national awareness campaigns in the USA for women [16].
Typical chest pain from CAD is more often identified in middle-aged men with risk factors for atherosclerosis; however, women, patients with diabetes mellitus and the elderly may not present with classical symptoms. For example, in a retrospective study of 94 patients admitted to a hospital with MI, 32% presented with ‘atypical’ symptoms, particularly women above 65 years of age when compared with men of the same age group [17]. Elderly women who are diagnosed with a ‘nonspecific chest pain’ are potentially at higher risk of cardiac morbidity [18]. Atypical' chest pain is a term best avoided as it heightens the risk of a misdiagnosis in women, the elderly, patients who have long-standing diabetes and those with a MI presenting with symptoms such as dyspnea or postprandial epigastric pain.
Coronary artery dissection is a rare, but often deadly cause of MI that mainly affects otherwise healthy, young females [19]. The etiology is unknown, and most patients presenting with this entity do not have risk factors for coronary heart disease.
Cardiac syndrome X is a syndrome of angina-like, nongastrointestinal chest pain associated with normal epicardial coronary arteries and a positive response to exercise testing. However, this syndrome may still reflect coronary insufficiency [20]. There is no direct association with gastroesophageal reflux disease (GERD) [21] and the syndrome is most commonly found in premenopausal women and has been associated with underlying panic disorder [22].
Over 30% of patients with CAD suffer from persistent chest pain caused by extracardiac sources overlapping or mimicking precordial symptoms originating in the heart [23,24]. These result primarily from the coexistence of gastroesophageal reflux, aspirin-induced GI tract damage and musculoskeletal or panic disorders [24–28].
A large multicenter US study, Internet Tracking Registry for Acute Coronary Syndromes (i*trACS), prospectively collected data on 17,737 patients with chest pain [29]. They concluded that when the initial impression is NCCP, high-risk features such as traditional cardiovascular risk factors or a history of CAD are still associated with adverse cardiac events. If patients present with these features, the treating physicians should consider further investigations before diagnosing patients with NCCP [30].
It should be noted that in patients with CAD, both cardiac and noncardiac causes of chest pain may exist concurrently. In any patient presenting with chest pain, cardiovascular risk factors such as diabetes, hypertension, dyslipidemia, obesity and smoking should always be managed appropriately.
Approach to NCCP
NCCP has a broad differential

Approximately 60% of chest pain diagnoses were not ‘organic’ in origin (i.e., not due to cardiac, gastrointestinal or pulmonary disease);
Musculoskeletal chest pain accounted for 20% of all diagnoses, with costochondritis (diagnosed by the history and physical exam) accounting for 13%, as did reflux esophagitis at 13%;
Stable angina pectoris was responsible for 10% of chest pain episodes in patients presenting with chest pain to primary healthcare physicians; unstable angina or MI occurred in only 1.5% of patients [31].
These findings are compatible with other reports of the frequency of etiologies of chest pain in primary care practice [32–36]. Pulmonary causes of NCCP include disease of the pulmonary vasculature, lung parenchyma or pleura.
Factors that likely contribute to NCCP include GERD, esophageal motility disorders, visceral hyperalgesia and psychiatric conditions
Patients who have non-GERD-related NCCP are considered to have functional chest pain of presumed esophageal origin [45]. Possible mechanisms include esophageal mechano-physical abnormalities, central and peripheral hypersensitivity and sustained contractions of the esophageal longitudinal muscle [46,47]. Balaban
In a recent study it was observed that an abnormal eosinophilic infiltrate was present in 14% of patients undergoing endoscopic evaluation for NCCP, suggesting that eosinophilic esophagitis should be considered in the differential diagnosis of NCCP [48].
Psychiatric evaluation of patients with NCCP has suggested a significant portion may meet the criteria for panic disorder, while others may suffer from depression [49,50]. There is an overlap with other mechanisms of NCCP such as esophageal mechano–physical abnormalities in these patients [49]. Therapy should be aimed towards the potential underlying disorder.
Prognosis
A prospective 4-year cohort study of patients presenting to a referral hospital in Sydney, Australia, with chest pain was conducted [51]. The study observed that the majority of patients with NCCP continue to have unexplained chest pain over time and there was no significant difference with regard to mortality, continued chest pain and quality of life between patients presenting with cardiac and NCCP [51]. Further, it was observed that the mortality rate for those either initially diagnosed as having chest pain of cardiac or non-cardiac origin at baseline was not significantly different, suggesting that presentation to hospital with acute chest pain that is diagnosed as noncardiac and normally considered nonfatal confers the same likelihood of death within a 2-year period from a cardiac cause as someone who presents with cardiac chest pain [51]. This study had limitations, including a relatively small sample size and patient selection from one hospital practice, so more data are needed.
Treatment
GERD-related NCCP
Background
GERD is the most common esophageal-related cause of NCCP, occurring in up to 60% of patients [52]. NCCP is the most common atypical symptom of reflux disease [53]; hence, empiric treatment of GERD remains the first-line management. Initial options for management include lifestyle modification and use of acid-suppressing medications. Proton pump inhibitors (PPIs) are considered to be the foundation of GERD management, with up to 90% of patients demonstrating improvement in symptoms with their use [54]. Those patients who fail to have an adequate response to antisecretory drugs may progress to surgical alternatives if GERD is confirmed. These surgical procedures are not without significant potential complications and response to surgery is less optimal in patients who fail an adequate PPI trial [55]. A new focus of interest has been the effect of GABA agonists in suppressing reflux. Developments are also being made in endoscopic treatments of GERD. Few studies examining the sole issue of NCCP have been performed; therefore, the following treatment of GERD has been extrapolated as a suggested management plan of NCCP by association; however, it is clear that more research is required to fully explore NCCP in its entirety.
Lifestyle modifications
In the current management of GERD, and its symptoms such as NCCP, there is a plethora of medications and interventions available to clinicians. Simple lifestyle adjustments such as weight loss, cessation of smoking, avoidance of alcohol and coffee, and elevation of the head of the bed have become overshadowed as primary therapies. However, these modifications are consistent with an understanding of the pathophysiology of reflux disease. As such, lifestyle modification may be a useful adjunct in the treatment of GERD, but is not strongly evidence based and usually is not efficacious enough to be the sole therapy utilized [56].
PPIs
PPIs (e.g., omeprazole, rabeprazole, lansoprazole and dexlansoprasole) are a mainstay treatment of the management of GERD-associated NCCP by suppressing acid production in the stomach. Many recent studies have focused on the diagnostic value and the role of an empirical trial of PPIs in NCCP [53,53,57–61]. Debate still exists over the required duration of a ‘PPI test‘, with Bautista
Histamine-2 receptor antagonists
The usage of histamine-2 receptor antagonists (H-2RA) has declined in the management of GERD-related NCCP and, as such, limited recent studies have been performed. Nagahara and colleagues compared the effects of a PPI (rabeprazole) and an H-2RA (lafutidine). They found that total reflux symptom scoring only improved with the use of rabeprazole [64]. Another study reported that cimetidine in conjunction with antacid use was only effective in 42% of GERD-associated NCCP patients [65]. Thus, H-2RAs have been superseded by the use of the more efficacious PPIs.
GABA agonists
Recent studies have focused on reducing transient lower esophageal sphincter relaxation (TLESR), a mechanism that is responsible for the majority of reflux episodes [66]. TLESRs are modulated by GABA acting on GABAB receptors [67]. Baclofen is a GABAB receptor agonist, and recent studies have shown that baclofen reduces the number of TLESRs, and thus the number of reflux episodes, and well as increasing the basal tone of the lower esophageal sphincter (LES) [66,67]. Other GABAB receptor agonists such as lesogaberan and AZD9343 have also demonstrated these effects, with lesogaberan reducing the number of TLESRs by 36% [67,68]. However, a significant side-effect profile is noted with these medications: drowsiness and incidences of short-acting paraesthesia have been reported [68]. A recent study by Gerson
Surgery
Laparoscopic nissen fundoplication (LNF) is the most common antireflux surgery performed, with the laparoscopic approach being the procedure of choice [70]. Controlled trials of surgery in NCCP are lacking. Patti
Endoscopic gastroplication
Endoscopic gastroplication is an emerging treatment for gastroesophageal reflux disease but is not yet US FDA approved for this indication and has not been studied in NCCP. There is a need for randomized, controlled trials to assess the effectiveness of this intervention; however, initial studies appear promising. Schwartz
Non-GERD-related NCCP
Introduction
Nonreflux-associated NCCP is often attributable to esophageal motor disorders. These disorders are often difficult to manage; however, current options include muscle relaxants, pain modulation therapy, endoscopic botulism treatment and consideration of psychological management. Recent areas of interest include the use of phosphodiesterase type 5 (PD-5) inhibitors, theophylline, tricyclic antidepressants (TCAs), selective-serotonin reuptake inhibitors (SSRIs) and serotonin–norepinephrine-reuptake inhibitors (SNRIs). The choice of pharmacotherapy depends on the suspected etiology of the esophageal disorder. Other therapies such as the use of octreotide have been investigated in the past; however, no recent research has been conducted and as such they have not been included in this review.
Muscle relaxants
*Nitrates
Previous studies have suggested that nitric oxide (NO) plays a significant role in esophageal motility and the regulation of esophageal wall smooth muscle contraction [77]. It was postulated that the administration of nitrates could alleviate esophageal spasm, and thus reduce the NCCP in these patients. There are no recent data available, as prior studies demonstrated that while sublingual nitroglycerin causes a statistically significant reduction in LES pressure, it is only a transient effect [78]. The effect was not reproducible with topical nitroglycerin or with the administration of isosorbide dinitrate. Another study showed that a glyceryltrinitrate infusion can reduce symptoms [79]; however, this is an impractical long-term therapy. The administration of nitrates is not an effective therapy for long-term management of NCCP, although its transient effect on esophageal relaxation explains why it may have an effect on acute chest pain, and response to its administration cannot be used to differentiate between cardiac and NCCP.
Calcium channel blockers
Calcium channel blockers have been shown to relax gastrointestinal smooth muscle and lower the LES pressure in patients with achalasia, nutcracker esophagus or diffuse esophageal spasm [80–82]. Studies have shown variable effects of differing calcium channel blockers in addition to conflicting results. Allen
PD-5 inhibitor
As previously discussed, NO causes the relaxation of esophageal smooth muscle by increasing cellular concentrations of cGMP. PD-5 terminates this action of cGMP. By opposing the action of PD-5 using inhibitors such as sildenafil, relaxation of smooth muscle cells occurs [89]. Several studies have conclusively demonstrated that sildenafil decreases LES pressure and also lowers the amplitude of esophageal peristaltic contractions [89–94]. It has therefore been suggested that PD-5 inhibitors could be used to relieve pain associated with spastic esophageal motor disorders caused by a defect in NO neuromuscular communication, such as nutcracker esophagus, achalasia and hypertensive LOS [89,91,92]. One patient with achalasia in the study by Eherer
Antidepressants
*TCAs
TCAs, such as imipramine, have been shown to have an effect in reducing NCCP [95]. The proposed mechanism of action is modulation of visceral pain perception [96]; however, it has also been suggested that they have a muscle-relaxant effect via the inhibition of calcium channels [97]. Imipramine has been shown to decrease pain response in a study of 20 healthy male volunteers [98] and it was also demonstrated to decrease esophageal pain in the presence of distension, supporting a visceral analgesia effect [96]. Cannon
*SSRIs
A recent randomized trial of sertraline and pain coping skills training in patients with NCCP demonstrated decreased pain intensity and pain unpleasantness. The combination of coping skills training with sertraline produced significantly greater changes in pain catastrophizing and anxiety when compared with placebo [101]. Another randomized study with paroxetine-treated patients exhibited improvements in the Clinical Global Impressions Scale, but not pain, when compared with placebo [102]. The role of SSRIs in symptom management for patients with NCCP therefore remains to be fully clarified but they may be worth considering in clinical practice.
*SNRIs
A small randomized, placebo-controlled, double-blind crossover trial of venlafaxine 75 mg versus placebo in 50 young patients with functional chest pain demonstrated significant symptom improvement in 52% of patients, with minimal side effects [103]. Further studies will need to be performed to confirm these findings.
Other pain-modulating therapy
*Benzodiazepines
Little recent evidence is available regarding the efficacy of benzodiazepines in the treatment of panic disorder in patients presenting with chest pain. Studies have reported that benzodiazepines, such as alprazolam and clonazepam, produced a significant drop in episodes of chest pain [104,105], although the sample size was limited. One of these studies reported eight out of 12 chest pain patients with panic disorders and normal coronary arteries halved the frequency of panic attacks within 4 weeks of clonazepam administration [104]. Further research is required to provide definitive evidence of their efficacy. In clinical practice, a trial of a benzodiazepine in patients with chest pain related to panic disorder may be of value.
*Theophylline
It has been suggested that theophylline may ameliorate esophageal chest pain by reducing visceral pain response via its actions on adenosine receptors [106]. An uncontrolled, open-label trial suggested that theophylline could be an effective treatment in functional chest pain [106]. A randomized control trial of intravenous and oral theophylline versus placebo was performed to further explore these results, and a reduction of symptoms such as number of episodes, duration and severity of chest pain episodes was shown in 58% of patients [107].
*Transcutaneous electrical nerve stimulation
Borjesson
Endoscopic treatment
*Botulinum toxin
Botulinum toxin (botox) causes muscle relaxation by inhibiting the release of acetylcholine from neurons at the neuromuscular junction. Therefore, botox may not only reduce esophageal muscle activity and thus the related symptoms of dysphagia and regurgitation, but also chest pain by reducing signaling in nociceptive (pain) pathways. A small uncontrolled study in patients with nonachalasia spastic esophageal disorders demonstrated reduction of chest pain in the majority of patients [109]. However, the first randomized, placebo-controlled, double-blinded study in 22 patients with nonachalasia esophageal hyper-motility disorder established that botox injections significantly improved dysphagia symptoms but had no significant effect on chest pain [110].
*Psychological treatment
Primary psychological causes of NCCP should be considered after negative evaluation of all organic causes. However, it is not uncommon for patients with NCCP to suffer from anxiety, depression and panic disorder. Psychological therapy could be of particular value in such patients [8,111,112] and early intervention might prevent these symptoms from becoming chronic. This is usually done using a behavioral framework, applying cognitive behavioral psychotherapy. A problem with many of the cognitive behavioral psychotherapy trials has been high attrition rates [113]. A recent study of manualized cognitive behavioral psychotherapy, including exposure to physical activity, showed it was an effective treatment for NCCP and benign palpitations over a 12-month follow-up but it was limited by its small sample size [114]. A small study of 28 patients with NCCP demonstrated that hypnotherapy helped alleviate pain intensity with improvement in overall well being [115]. Another study of 39 patients with functional chest pain, in which 21 patients were in the Johrei (a process of transmission of healing energy) group and 18 in the wait-list group, suggested that Johrei induced a significant reduction in symptoms. However, the authors concluded that further studies are needed to compare Johrei treatment with sham Johrei and supportive care [116]. Overall, it is still unclear whether it is of value to offer patients with NCCP psychological treatment and at what stage this should be considered.
Conclusion
NCCP is common, and places a relatively high financial burden on the healthcare system [8,117,118]. Generally the prognosis of patients with NCCP is positive [119], but certain subgroups of patients such as middle-aged women may be at increased risk of misdiagnosis as they may not present with classical symptoms of CAD [17]. As GERD is the most common cause of NCCP, antireflux therapy plays an important role in diagnosis and treatment.
In non-GERD-related NCCP targeted treatment of visceral hyperalgesia and esophageal motility disorders is required. Many patients with NCCP have psychiatric conditions requiring psychological treatment.
Future perspective
The mechanisms inducing chest pain from the esophagus are now more readily identified in practice using pH-impedance, high-resolution manometry and, in specialized centers, endoscopic ultrasound evaluation of motor contractions. There are currently several proposed treatments that may be further developed for NCCP that is refractory to PPI therapy. The use of GABAB agonists reflects a different approach to the traditional management of decreasing acid secretion and aims to improve the effectiveness of the lower esophageal sphincter. Initial trials into this class of drug have shown a significant reduction in reflux episodes, and provided the adverse effect profile of these medications is limited, then GABAB agonists may offer a new management strategy for GERD. Further development of this class of medication is currently ongoing. PD-5 inhibitors have shown promise in the management of spasmodic esophageal disorders, with effective reduction of symptoms in trials to date. The development of long-acting forms of this medication may allow this to become a viable treatment option. A new target of therapy for treatment of non-GERD-related NCCP has been in the region of pain modulation. There are several pharmacological approaches for which preliminary studies have shown a reduction of symptoms. Theophylline and some TCAs have been demonstrated to have pain-modulating effects, via their action on receptors. Studies into the effect of SNRIs, SSRIs and psychological therapy have also found a reduction in symptoms and, although the mechanism of the symptom improvement is unclear and may be related to improved coping skills and anxiety relief, initial research nonetheless, shows a clear reduction in symptoms. Recent technological advances have allowed the expansion of endoscopic therapy. Gastroplication is one possible approach to reduce usage of antisecretory drugs in GERD-related NCCP. Further investigation is required to assess the long-term efficacy of these treatments; however, preliminary studies have shown positive results. The endoscopic administration of botox has shown a reduction in non-GERD-related chest pain in some studies, although the research to date has been of small patient samples and there have been inconsistent results and, additionally, the efficacy of the treatment is short lived. These therapies may have the potential to change current management of NCCP, and deserve further development and exploration in properly conducted clinical trials.
Executive summary
Noncardiac chest pain (NCCP) is very prevalent in the community and has high financial implications.
Coronary artery disease is the leading cause of death in women; patients should be thoroughly investigated for coronary artery disease before being diagnosed with NCCP.
Proposed causes of NCCP include gastroesophageal reflux disease (GERD), esophageal motility disorders, visceral hyperalgesia, psychiatric conditions and uncommonly eosinophilic esophagitis.
Generally good but some evidence suggests there is no significant difference with regards to mortality, continued chest pain and quality of life between patients presenting with cardiac and NCCP.
GERD is common and treatable; proton pump inhibitor treatment remains the mainstay of therapy in GERD-related NCCP.
Visceral sensation secondary to acid sensitization deserves further attention.
Combined reduction of both acid reflux and pain sensation may be the best hope for proton pump inhibitor failures.
Footnotes
Management of noncardiac chest pain in women
To obtain credit, you should first read the journal article. After reading the article, you should be able to answer the following, related, multiple-choice questions. To complete the questions (with a minimum 70% passing score) and earn continuing medical education (CME) credit, please go to www.medscape.org/journal/wh. Credit cannot be obtained for tests completed on paper, although you may use the worksheet below to keep a record of your answers. You must be a registered user on Medscape.org. If you are not registered on Medscape.org, please click on the New Users: Free Registration link on the left hand side of the website to register. Only one answer is correct for each question. Once you successfully answer all post-test questions you will be able to view and/or print your certificate. For questions regarding the content of this activity, contact the accredited provider,