
Abstract
Teratogenic medications are commonly prescribed to women of reproductive age. Caring for women who may benefit from the use of teratogenic medications requires clinicians to engage patients in shared decision-making on the risks and benefits of medication use in the context of the patient's fertility goals, the implications of the patient's medical condition for a pregnancy and the risks and benefits of various contraceptive methods, Effective communication about all of these issues is essential to avoiding medication-induced birth defects. However, data suggest that I such communication remains inadequate, leading some women to face unintentional exposure of a pregnancy to a teratogen, undesired pregnancy or, sometimes, the need for pregnancy termination services. This review outlines key information needed to ensure safe prescribing to women of childbearing age. It includes recommendations for changes in medical education, healthcare delivery and health policy to facilitate thoughtful prescribing and comprehensive care.
Keywords
Birth defects are the leading cause of infant mortality in developed countries [1]. Birth defects are common; for example, the US CDC estimates that 3% of births in the USA result in major birth defects [2]. The exact number of defects attributed to teratogenic medication use is not known. However, potentially teratogenic medications are commonly prescribed for women of reproductive age. A UK-based study using the national General Practice Research Database found that one out of every 164 women was prescribed a US FDA-designated category X medication in early pregnancy [3]. In the USA, an analysis of the National Ambulatory Medical Care Survey (NAMCS) found that from 1998 to 2000, 11.7 million potentially teratogenic medications were prescribed to women of childbearing age in the USA [4]. Furthermore, 6% of US pregnancies are exposed to potentially teratogenic medications, and up to half of US pregnancies are exposed to drugs for which there is limited evidence of safety during pregnancy in humans [5].
Pregnant women may have chronic medical conditions that persist during pregnancy or may develop new medical problems during pregnancy, so the use of prescription medication may be both appropriate and necessary. However, given the frequency of use of potentially teratogenic medications and the high stakes, it is essential that providers take a systematic approach to the use of these medications, using the best available evidence. Failure to engage women in appropriate discussion of the risks and benefits of medication use can result in inadvertent exposure to the fetus, and at times even pregnancy termination. Alternatively, a lack of guidance about medication use during pregnancy may result in unnecessary discontinuation of important medications, resulting in maternal or fetal harm.
Medication use in pregnancy presents clinicians and patients with complex challenges. First, scientific evidence proving teratogenicity is notoriously limited, so that regulatory bodies, clinicians and patients must base decisions on imperfect information. Second, medical training in toxicology and pregnancy risk, as well as preconception and contraceptive counseling, is limited, especially among primary care clinicians. Third, half of all pregnancies in the USA are unplanned – a rate that reflects the challenges women and men face in accessing contraceptive services [6]. Fourth, upon this foundation of limited training, incomplete data and inadequate access to preventive services, within a short office visit, clinicians and patients must engage in decision-making that is medically complex and emotionally charged. As one FDA expert describes, “All prescribing and drug-use decisions in pregnancy require consideration of various clinical and individual factors including the potential effects of the drug on the mother and fetus, the severity of the mother's condition, maternal tolerance of the drug, coexisting maternal conditions, the impact of maternal illness on the fetus, and available alternative therapies” [7].
For women of reproductive age who are considering taking teratogenic medications, the following services are essential:
For women who are not pregnant, discussion of fertility goals, including the potential risks, benefits and alternatives of a medication if she becomes pregnant;
For women who do not desire pregnancy, monitoring for pregnancy and provision of highly effective contraception that is safe in the setting of pre-existing medical conditions;
For women who wish to become pregnant, preconception counseling, monitoring for pregnancy and thorough discussion and documentation of the risks and benefits of continuing, initiating or stopping a particular medication;
For women who are pregnant, thorough discussion and documentation of the risks and benefits of continuing pregnancy, and of continuing or stopping a given medication; referral for appropriate prenatal care or access to pregnancy termination services when needed.
In this review, we will first discuss what is known about drug teratogenicity and discuss the existing safety categories commonly used by clinicians in the USA. We will then offer detailed clinical guidelines for addressing the needs of women of reproductive age who are considering taking potentially teratogenic medications. Finally, we will discuss changes in clinical practice, medical education, healthcare delivery and policy that can help providers better address these needs.
Defining pregnancy risk
Teratogenic medications can be characterized as ‘high-risk teratogens’ (e.g., isotretinoin, which is thought to affect approximately 20–30% of exposed fetuses [8]) or ‘moderate-risk teratogens’, which increase the risk of a birth defect to a smaller degree [9]. Potential fetal effects after exposure to teratogenic medications include spontaneous abortion, malformations, visible developmental impairment, small size for gestational age, impaired intellectual development, carcinogenesis and increased risk of genetic mutations [10]. These fetal effects are modified by a variety of factors, including medication dose and duration of exposure [11], gestational age at exposure [11,12] and genetic susceptibility [11]. Adequate nutrition (e.g., folate intake may be able to decrease the risk of teratogenicity of some medications; e.g., in animal studies, folic acid attenuates the risk of valproic acid-related birth defects [13]).
Unfortunately, the most significant adverse effects of medications occur early in pregnancy, before many women realize that they are pregnant. From conception to 2 weeks after fertilization, teratogens increase the risk of early fetal death and spontaneous abortion [12]. Organogenesis occurs during weeks 3–8, and during this time the fetus is at risk of developing major morphologic abnormalities [12]. During later weeks of gestation, teratogenic exposures increase the risk for more subtle morphologic abnormalities and can produce biochemical, behavioral or reproductive abnormalities. Of note, however, the consequences of later exposures can still be of great clinical significance (e.g., renal impairment from angiotensin-converting enzyme inhibitor use, which can be fatal for the fetus [11]).
Balanced against the risks that many medications pose to a fetus are the risks that medical conditions can pose to both the mother and fetus. Poorly controlled diabetes, cardiovascular, renal and thyroid disease all have potentially adverse effects on a fetus. Depression during pregnancy can affect a woman's participation in prenatal care, make her more likely to use tobacco and alcohol during pregnancy and may affect fetal growth and infant behavior [14].
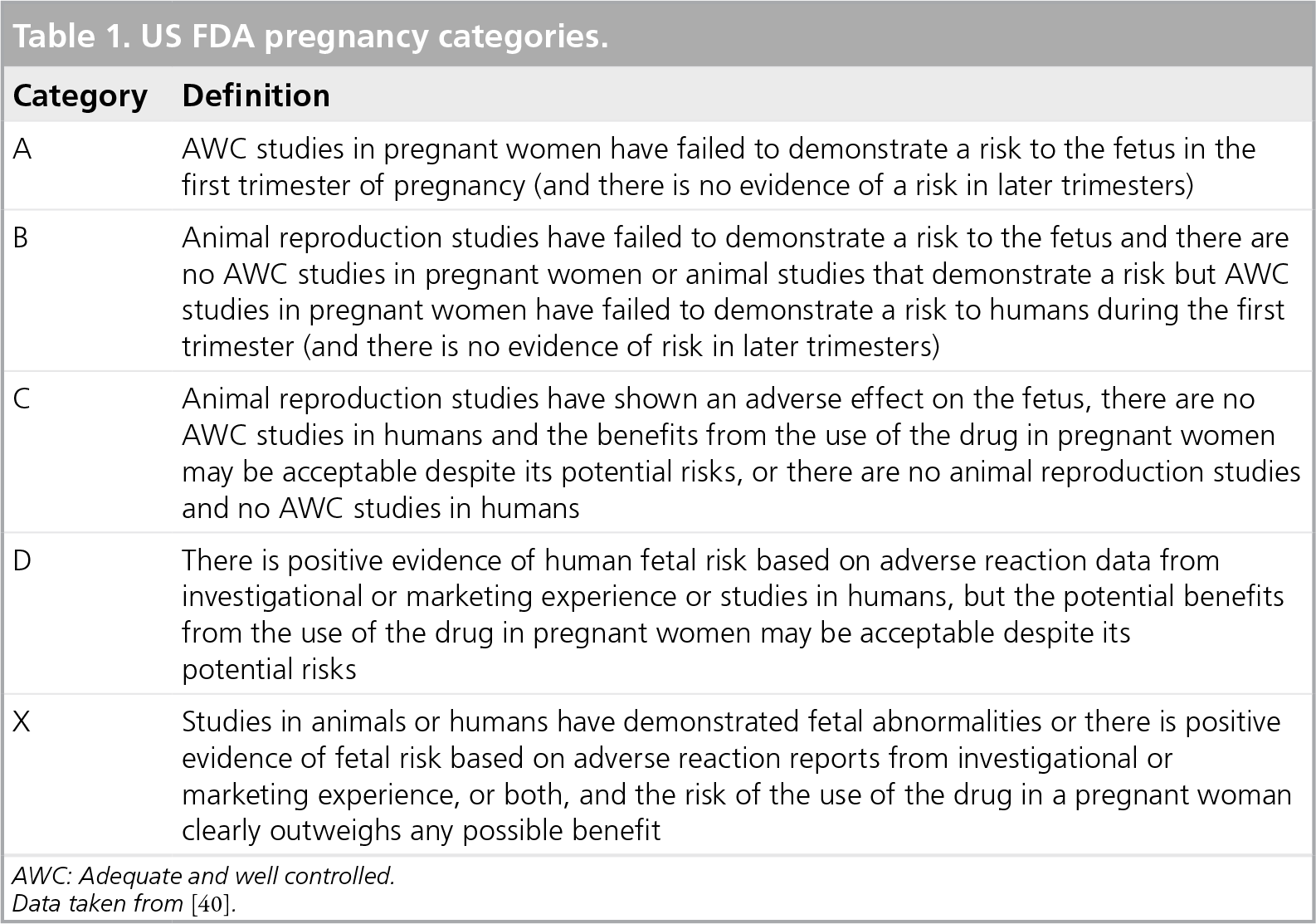
Since 1979, the FDA has provided a pregnancy risk classification system to guide decision-making about medication use (
Commonly used teratogenic medications.

see
Use during late pregnancy is avoided due to concerns about premature ductal closure.
Includes irritability, weak or no crying, tachypnea, temperature instability, hypoglycemia and occasionally seizures [14].
ACE: Angiotensin-converting enzyme; SSRI: Selective serotonin reuptake inhibitor.
Adapted with permission from [10].
The limitations of the FDA pregnancy categories have been widely acknowledged and exemplify the challenges of translating pregnancy safety data into clinical recommendations. First, the data underpinning the labeling is limited. Animal studies have limited ability to predict adverse effects in a human fetus because of variations between mammalian species and also the different doses that are administered in animal studies [9,15]. Few premarketing drug trials include pregnant women for ethical reasons and, moreover, most such studies would be too small to detect differences in the incidence of birth defects [9]. Postmarketing surveillance is thus an essential source of information. Types of postmarketing data sources include epidemiologic studies such as cohort studies, pregnancy registries (i.e., cohort studies in which pregnant women exposed to a certain drug are enrolled and maternal and infant outcomes are followed through time and sometimes compared with a control group) and case–control studies [11]. These types of studies can be very helpful, but are often limited by bias (e.g., recall bias for case–control studies, and self-referral bias for pregnancy registries) and the challenge of selecting an appropriate comparison group (for pregnancy registries) [11]. Pregnancy registries are often initiated by pharmaceutical companies and are drug-specific. In addition, since birth defects are rare, cohort studies are often not adequately powered to detect an increased rate of events with exposure to a medication. Lastly, reporting of birth defects (e.g., by patients and by maternal providers) is often inaccurate, partly because some abnormalities may only be detected later in an infant's life [11]. Case reports and adverse-event reporting systems such as the FDA's have also been used in raising concerns about medication safety and may also influence pregnancy safety labeling, but are vulnerable to underreporting and reporting bias, and cannot establish causality [15].
As consumers and clinicians felt that the FDA categories were overly simple and often misleading, suggesting to some a gradation in risk from A to X and including medications with substantially different pregnancy-risk profiles in different categories would be useful. Starting in 2008, the FDA added more detailed labeling to these categories with the plan to eventually exclude letter categories and instead provide more information on risk:benefit calculations, including clinical considerations and a more in-depth presentation of supporting data. However, the final version of these regulations has not yet been published [7]. It is hoped that these will offer a more nuanced portrait of the risks associated with medications in pregnancy. Given the limitations of the underlying data, even with the new labeling, physicians and their patients will probably continue to face clinical situations fraught with uncertainty, which will require highly individualized decision-making.
The challenge for providers
Along with the multiple other tasks inherent to primary care, it is primary care providers who often bear the chief responsibility for guiding such decision-making as the majority of teratogenic medications are commonly used in primary care practice. In the NAMCS study, the most commonly prescribed potential teratogens were anxiolytics, anticonvulsants, antibiotics and HMG CoA reductase inhibitors (‘statins’) [4]. Of the approximately 12 million category D or X medications prescribed to women of childbearing age in this study, primary care physicians prescribed 45% of these medications, followed by dermatologists and psychiatrists [4].
Importantly, these groups of physicians may have limited training in addressing medication teratogenicity, preconception counseling and contraceptive care. Indeed, ample data suggest that physicians in the USA are not consistently providing these services. In the NAMCS analysis, for example, only 20% of women of childbearing age who were prescribed a teratogenic medication received contraceptive counseling or provision [4]. In another study of a large health maintenance organization, only half of the women receiving Class D or X medications were documented to have received contraceptive counseling or prescription contraceptive [16]. Many general physicians have limited training in identifying teratogenic medications, investigating fertility intentions and counseling patients about appropriate contraception [17,18]. In a qualitative study, primary care providers identified numerous barriers to counseling about teratogenic medications. These included a dearth of reliable information sources on teratogenic medications, lack of time for thorough patient counseling, lack of reimbursement for contraceptive and preconception counseling and uncertainty about patients' pregnancy plans [18].
The reproductive health needs of women on teratogenic medications
The fundamental initial steps in caring for women of reproductive age who are candidates for teratogenic medications include recognition of a medication as a potential teratogen and assessing a woman's pregnancy status and fertility intentions.
Identifying teratogens
Providers must consider teratogenicity each time they prescribe medications to women of reproductive age, just as they should counsel women about fertility goals and offer preconception or contraceptive counseling. Information resources available to providers include drug labels, which may draw on information from pregnancy registries, retrospective cohort studies, case–control studies and pregnancy surveillance programs. Commonly used drug information resources such as Micromedex® (Thomson Reuters, NY, USA) can be useful, as is information provided by the Organization of Teratology Information Specialists [101] and Teratogen Information Service [102]. Proposed mechanisms for improving provider education and access to information are described in the last section of this review.
Assessing fertility intentions
Any woman of reproductive age who is taking or considering taking a teratogenic medication should be encouraged to articulate her fertility goals. Particularly for women with chronic medical conditions, regardless of her stated fertility intentions, the implications of a patient's medical condition for her pregnancy, including the risk of teratogenic medications, must be regularly discussed. Pregnancy intentions should be assessed regularly as they may change with time. When possible, pregnancy intentions should be assessed in an open-ended way, which may be more consistent with women's actual experience. For example, questions can be phrased as ‘How would you feel about becoming pregnant?’ or ‘Would you mind becoming pregnant?’ [10]. Ambivalence about becoming pregnant is common and is a risk factor for use of less effective contraceptive methods [19]. If providers sense such ambivalence they should be aware that unplanned pregnancy is more likely and teratogenic medications should be avoided as much as possible.
Preconception counseling & pregnancy testing
For women desiring pregnancy, the teratogenicity of a given medication must be discussed in detail and documented, with acknowledgement of the uncertainty surrounding these issues. In addition, the risks and benefits of stopping a given medication must be discussed. Of note, women who have depression or anxiety may be more likely to have inflated concerns about the teratogenic risks associated with medications. Providers should be particularly aware of this given the risk of depression during pregnancy; physician reassurance can often mitigate patients' concerns [20,21].
For patients of reproductive age who are sexually active and have no history of surgical sterilization, a pregnancy test should be conducted prior to initation of a teratogenic medication. Some experts recommend monthly pregnancy testing for sexually active women who are not using prescription contraception [10]. For women desiring pregnancy, this will facilitate early diagnosis and appropriate monitoring as needed. Along with medication counseling, other preconception counseling, such as prescription of prenatal vitamins, and counseling about smoking cessation and nutrition, should be undertaken at the same time.
Prescribing for women who are pregnant or desiring pregnancy
For acute, relatively mild medical conditions that do not pose a significant risk to a woman or her pregnancy (e.g., a viral upper respiratory infection), medications should be avoided during the first trimester if possible. When the benefit of a medication is felt to outweigh potential risks, clinicians should consider prescribing the lowest effective dose of the medication with the most data on safety in pregnancy. Of note, the relationship between dose and teratogenicity has been primarily shown in animal studies [13]; human studies rarely show variation in teratogenic responses by dose presumably because of the narrower therapeutic dose range in clinical use [11]. Older medications with good safety records are generally preferred to newer medications with less supporting data [10]. For chronic medical conditions or conditions that pose a risk to the woman or fetus if untreated, safer alternatives to a medication should be sought if they exist. For example, pregnant women or women desiring pregnancy with severe hypertension, oral agents of choice include methyldopa, labetalol and metoprolol. Some women with severe depression will need to continue receiving pharmacologic therapy while pregnant. Selective serotonin reuptake inhibitors are considered to be safer than tricyclic antidepressants, but paroxetine should be avoided since it has the strongest association with fetal cardiac malformations [14]. Many women with rheumatoid arthritis are transitioned from disease-modifying antirheumatic drugs, such as methotrexate, to higher doses of steroids during, or in anticipation of, pregnancy. While steroids carry risks for pregnant women and fetuses, they are probably safer than many disease-modifying antirheumatic drugs [22].
Contraceptive care
With typical use of condoms or fertility awareness-based methods, 15–25% of women become pregnant within the first year of use. With no contraception, 85% of sexually active women become pregnant within a year [23]. Thus, to prevent birth defects, it is essential that women taking potentially teratogenic medications who do not desire pregnancy use effective contraception. If a woman declines contraception, the provider must document that the patient has expressed understanding of and willingness to accept an increased risk of a birth defect or other adverse outcome for her infant. For those women who are willing to use contraception, highly effective reversible contraceptive methods such as intrauterine devices and subdermal implants are preferred. For example, less than 1% of women using a Mirena® (Bayer, Leverkusen, Germany) or Paragard® (Teva Pharmaceutical, Petah Tikva, Israel) IUD will have an unintended pregnancy within the first year of use, whereas 8% of women using oral contraceptive pills will be pregnant within a year of typical use [23]. Unfortunately, these highly effective methods remain underused in the USA; only 5.5% of contracepting US women currently use an IUD [24]. This appears to be at least partly because of inadequate provider knowledge about these methods [25,26], as well as relatively high out-of-pocket costs for patients [27–29].
Many women on teratogenic medications have chronic medical conditions that may affect contraceptive recommendations. The US Medical Eligibility Criteria for Contraceptive Use (US MEC), a free resource available on the internet, provides a large amount of useful information when determining the safety of various contraceptive options in the setting of chronic medical conditions [30]. The US MEC assigns each contraceptive a category from 1–4 for a large number of medical conditions, where 1 represents a condition for which there is no restriction to a given contraceptive method, 2 represents a condition for which the advantages of using the particular method generally outweigh the theoretical or proven risks, 3 indicates a condition for which the theoretical or proven risks usually outweigh the advantages and 4 indicates a condition that represents an unacceptable risk if the contraceptive method is used


Women taking potentially teratogenic medications and oral contraceptives have been found to display similar rates of nonadherence to oral contraceptive pills compared with the general population [31]. In situations in which nonadherence seems likely, methods that depend minimally on patient adherence should be recommended or, in discussion with the patient, teratogenic medications should be avoided. Pregnancy tests should be performed routinely for women for whom adherence is challenging. Particularly for women using less effective methods of contraception, emergency contraception should be provided in advance, since this has the potential to increase timely use and reduce the risk of unintended pregnancy [32].
Management of unintended pregnancy
For the substantial number of women who may become pregnant while taking a potentially teratogenic medication, options for management of the pregnancy must be presented in a compassionate and open-ended way. For those women who wish to terminate the pregnancy, whether because of concerns about the medication exposure or for other reasons, comprehensive pregnancy options counseling should be provided and when need be, the patient should be referred promptly for desired services. For those women who are ambivalent about continuing their pregnancy, referral to a teratogen information specialist (see [101]) or an obstetrician or gynecologist is indicated to explore the implications of use of specific medications during pregnancy, and conduct early fetal surveillance as needed or wherever possible, in order to guide decision-making.
Management of desired pregnancy
If a woman becomes pregnant while taking a teratogenic medication and wants to continue the pregnancy, referral to an obstetrician–gynecologist and preferably a maternal–fetal medicine specialist is important early in pregnancy in order to provide thorough counseling about the risks. While clinicians must present the scientific uncertainty that exists with regard to the teratogenic effects of most medications, patients must be aware of serious adverse effects that may be seen in the fetus. In addition, special monitoring or treatment may be warranted during pregnancy depending on the drug exposure. For example, if a medication is known to cause fetal cardiac defects, fetal echocardiography may be indicated. Higher doses of folic acid are prescribed for women taking some agents known to cause CNS deficits. In addressing the woman's own medical condition and providing any additional monitoring for the fetus, close communication and coordination of care between the patient's obstetrician/gynecologist, specialist provider and primary care are essential.
Improving providers' ability to address women's reproductive health needs
A number of types of evidence suggest that providers in the USA are not adequately meeting the reproductive health needs of women who are considering use of potentially teratogenic medications. Diverse interventions are needed to address this problem. First, the need for better data on drug safety in pregnancy is clear. A solid evidence base could help prevent women with chronic medical conditions from stopping or underdosing necessary medications, and help other women avoid medications that could be harmful to the fetus. Many experts have argued that pregnant women should be more consistently included in certain research studies, in particular those studies that examine medications already used widely in pregnancy, or randomized controlled trials of drugs treating conditions for which there is no other known effective therapy [33]. In addition, there is an opportunity to more systematically collect and analyze the experiences of women already taking certain medications while pregnant, including through improved coordination of pregnancy registries, and other postmarketing surveillance strategies [15,33]. Data have been published recently from international networks of birth defect surveillance programs that suggest promise from global collaboration [34].
Second, healthcare providers need better education in identifying potentially teratogenic medications, evaluating the risks and benefits of such medications, counseling patients appropriately and prescribing effective contraception. This is particularly important for primary care physicians, who not only prescribe the majority of teratogenic medications in the USA, but may also find themselves at the center of coordinating care while weighing the views of multiple specialists who may be involved in managing a patient's chronic medical condition, and the clinicians who are focused on the well-being of the pregnancy. Training in contraceptive counseling, and in the provision of highly effective reversible contraceptive methods, are particularly important for primary care providers. Medical school, residency training and continuing medical education are important forums for such education.
Third, changes in healthcare finance and delivery systems can support providers in meeting patients' needs. Since primary care providers have identified limited clinical time and lack of reimbursement for time spent counseling patients as barriers to preconception and contraceptive counseling [18], health reform legislation should consider increasing reimbursement for these important preventive activities. Clinics may wish to designate mid-level providers or counselors to assist with these services, for example through documentation of a ‘contraceptive vital sign’ that assesses and records patients' contraceptive use prior to meeting with a physician [35]. Appropriate use of health information technology in decision support shows promise in increasing rates of counseling by assisting providers in identifying potentially teratogenic medications as well as women in need of preconception or contraceptive care [36]. Healthcare reforms may also improve coordination of care and provider communication. For example, in the USA, patient-centered medical homes and accountable care organizations may facilitate communication between specialists, primary care providers and obstetricians/gynecologists allowing improved risk:benefit calculations to guide decision-making about medication use.
Conclusion
The use of potentially teratogenic medications is a significant public health issue that affects millions of families each year. Despite challenges that include limited data and competing clinical tasks, safe prescribing for women of reproductive age should be a national priority. There are ample opportunities in research, medical education, clinical practice and health policy to improve care for women of reproductive age who are taking or considering taking teratogenic medications. With increased attention to this issue, clinicians and policy-makers can help promote healthy pregnancies and healthy lives.
Future perspective
Changes in health policy and delivery may have a profound impact on the care of women of reproductive age. The next 5 years promise to bring dramatic changes in medical practice throughout the developed world, as escalating healthcare costs force nations to intensify their focus on prevention and cost-effective care. In the USA, patient-centered medical homes and accountable care organizations may offer healthcare delivery and payment reforms that have the potential to improve and integrate care for women with medical conditions that make them eligible for teratogenic medications. In addition, expanded access to care in the USA could offer improved services for women of reproductive age. In particular, the US Institute of Medicine recently recommended a set of key preventive services for women that should be covered by insurers without cost sharing. These services included routine preconception care, as well as contraceptive counseling and provision. These recommendations were accepted by the Secretary of Health and Human Services and have the potential to expand access to preventive services for many insured women in the USA by 2012 [37]. They will need to be accompanied by increased provider training in counseling and contraceptive provision.
Management of teratogens in women of reproductive age is a concern in developing nations as well, where rates of serious birth defects are even higher [1]. While there are many reasons for high rates of birth defects in many low and middle income countries, teratogenicity of medications is an important concern particularly as non-communicable diseases such as diabetes pose an increasing public health burden, and since some chronic diseases such as rheumatic heart disease and peripartum cardiomyopathy disproportionately affect young people. Awareness must be raised about teratogenicity, and family planning must be closely integrated early on into nascent chronic disease management programs [38].
The FDA's intensive revisions of pregnancy risk categories will provide an opportunity for education of providers and the public about the risks associated with teratogenic medications and could potentially serve as an example worldwide. Through increasing awareness of the limitations and complexity of decision-making around medication use during pregnancy, these new labels may also serve as a call for increased research on the effects of medication use during pregnancy. As discussed, more focus on the reproductive implications of medications, and international coordination of surveillance programs, could dramatically improve the care of women who are pregnant or of reproductive age.
Despite these opportunities, challenges remain to the provision of comprehensive reproductive health services to women who are prescribed potentially teratogenic medications, and these challenges are likely to persist in the next several years. In the USA, political opposition continues to thwart efforts to increase women's access to comprehensive contraceptive care, for example through threatened funding cuts for public family planning programs and proposed exemptions to insurance coverage for contraception. In addition, education in contraception is highly variable and often sidelined in medical school and residency curricula, whether for political reasons or simply because of the range of topics competing for limited time [39]. Finally, controversy persists around the issue of including pregnant women in clinical trials. Clinicians should call attention to these issues in their educational institutions, clinical practices and state and national governments, in order to advocate for comprehensive care for women and families.
Executive summary
Women of reproductive age are frequently prescribed potentially teratogenic medications and birth defects are common.
The US FDA's pregnancy safety categories are the most widely known categorizations, however, these have been widely criticized and are under revision.
Pregnancy labeling is notoriously challenging because of the limitations of the underlying data.
Better data and improved coordination of pregnancy surveillance programs are needed.
Partly because of the dearth of adequate data, and also owing to educational gaps, providers are often inadequately prepared to address the reproductive health needs of women who are taking or considering taking teratogenic medications.
Comprehensive care for women of reproductive age who may benefit from potentially teratogenic medications requires careful assessment of risks and benefits associated with the medication or its cessation, and shared decision-making between the clinician and patient.
It includes assessment of fertility intentions, pregnancy testing and preconception or contraceptive counseling and care.
Changes in medication education and training, healthcare delivery and policy can facilitate provision of these services to women of reproductive age.
Footnotes