
Abstract
Congenital abnormalities of the breast and chest wall are seen frequently in breast, pediatric and plastic surgery clinics. Management involves a multidisciplinary team approach. The treatment for many of these conditions includes surgical correction. If the child is still growing, treatment timing is crucial and many of the surgical corrective procedures require more than one operation over a number of years. Although these deformities have less impact on functional capacity, the psychological consequences can be serious in adolescent patients. They can experience embarrassment, social isolation and complexities during sexual development, and this results in problems with relationships. The aim of this article is to spread awareness among the medical community of this range of conditions, so appropriate referrals are made and their impact is reduced by timely appropriate surgical intervention if appropriate.
Keywords
 Medscape: Continuing Medical Education Online
Medscape: Continuing Medical Education Online
This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education through the joint sponsorship of Medscape, LLC and Future Medicine Ltd. Medscape, LLC is accredited by the ACCME to provide continuing medical education for physicians.
Medscape, LLC designates this Journal-based CME activity for a maximum of
All other clinicians completing this activity will be issued a certificate of participation. To participate in this journal CME activity: (1) review the learning objectives and author disclosures; (2) study the education content; (3) take the post-test with a 70% minimum passing score and complete the evaluation at www.medscape.org/journal/wh; (4) view/print certificate.
Learning objectives
Upon completion of this activity, participants should be able to:
Describe classification of congenital abnormalities of the breast and chest wall
Describe overall principles of management of congenital abnormalities of the breast and chest wall
Describe characteristics and management of Poland's syndrome
Congenital abnormalities of the breast and chest wall are common. The first ever documented evidence of congenital breast deformity (athelia: absence of a breast) was reported in the Bible: “we have a little sister, and she hath no breast, what shall we do for our sister in the day that she shall be spoken for?” (Song of Solomon).
There is also evidence of congenital abnormalities in Greek mythology and art. Artemis, the goddess of childbirth is depicted as having multiple accessory breasts (polymastia). The wood carving of ‘Therese Ventre of Marseilles’ shows a supernumerary breast and nipple on her thigh (polythelia).
Psychological issues are important in this patient group, particularly during puberty and adolescence; issues include social embarrassment, low self esteem, depression and isolation from peers. Problems that occur relate to sexual relationships and cultural beliefs. There are also functional problems encountered later in life with lactation and breast feeding.
The aim of this review is to outline the various congenital abnormalities that can affect the breast and to discuss how and when they can be corrected or treated.
Embryology
The breast is a modified apocrine gland. During the 4–6th week of gestation, an ectodermal ‘mammary ridge’ or the ‘milk-line’ develops, which extends from the future axilla to the groin. The epithelial cords appear as 15–20 buds. These buds disappear or coalesce in human embryos, and usually one bud that is located in the 4th or 5th intercostal space persists and develops. The future breasts develop from these buds in an identical manner in male and female infants. These ectodermal buds grow into the underlying mesoderm as branching lactiferous ducts by 15–20 weeks.
The nipple and areola develop from the ectoderm at the junction of 15–20 lactiferous sinuses that arise from the ducts.
Maternal levels of estrogen are low during pregnancy, but increase at birth. Stimulation by the neonatal pituitary to secrete prolactin and the effect of estrogen can cause unilateral or bilateral breast enlargement, and even secretion of ‘witch's milk’. These changes are seen in male or female infants, but usually settle down within weeks. These secretions should not be ‘squeezed out’ as it can lead to persistence of milk production.
The breast tissue undergoes lobular proliferation in females at puberty, when the breast buds develop into adult size breasts; the process is called the larche.
Congenital abnormalities of the breast

Common congenital abnormalities of the breast and chest wall.
Congenital abnormalities of the nipple
Accessory nipples are seen in 1–5% of the general population (differences among ethnic groups have been noted) with the same incidence in male and females [1].
Accessory nipples develop along the milk line; more than 90% are seen in the inframammary region. These nipples can be unilateral or bilateral and are quite well developed with surrounding areola in some (

Accessory nipple.
There is some evidence that polythelia may be familial and related to urological (ectodermal) abnormalities [2,3]. Urological workup has been recommended to rule out associated abnormalities [4], but in clinical practice this is not considered necessary as accessory nipples are common, whereas urological abnormalities are rare and usually obvious because of other symptoms.
Most require no treatment unless the nipple causes irritation or is excised for cosmetic reasons.
Congenital nipple inversion
Sir Ashley Cooper first described congenital inverted nipples in 1840. It is seen in 2% of the general population [5], with a family history of such a condition in 50% of patients. The cause for this abnormality is thought to be tethering and shortening of breast ducts, and development of fibrous bands behind the nipples during intrauterine life.
It can cause mechanical problems with breast feeding; however, many can breast feed without any difficulty, probably because of changes that occur in the breast during pregnancy.
There are a variety of procedures described for the surgical correction (e.g., tightening of the areolar edge circumferentially and use of adjacent dermal flaps to augment nipple); however, loss of sensation and inability to breast feed are major concerns with surgical procedures.
Most of the procedures involve short circum-areolar incision or an incision at the base of the nipple. The tight bands are stretched, but it is often required to divide the ducts. A stitch can be placed at the base of nipple when it is everted, but this is not recommended (

A device called a Niplette™ is available from pharmacies. This is a suction device that, when used regularly, is successful in a few women at everting the nipple.
Athelia
Complete absence of nipple and areola is termed as athelia. This condition can be familial (autosomal dominant), and may be unilateral or bilateral, and is seen in association with amastia or rare syndromes such as scalp-ear-nipple or SEN syndrome (scalp nodules and ear malformation), Al-Awadi/Rass-Rothschild syndrome and Poland's syndrome [6].
A thorough investigation to rule out any other associated ectodermal abnormalities is required. Nipple and areola reconstruction can be carried out using small tissue flaps along with tattooing of a new areola in the absence of any other deformity. Skin grafts could also be used to create areola.
Congenital abnormalities of the breast
Accessory breast tissue or supernumerary breasts: polymastia
Accessory breast tissue or supernumerary breasts are seen in approximately 1–2% of the general population, but figures as high as 6% have been reported. There is a female preponderance with some reported as hereditary cases [7,8].
In approximately a third of patients, accessory breasts are found in more than one site; the most common site is the axilla (

Bilateral accessory axillary breasts.
Polymastia is usually diagnosed at puberty or during pregnancy when the accessory breast tissue develops along with the normal breasts. These are mostly asymptomatic, but can cause discomfort, and in some are seen as cosmetically unacceptable. Accessory breast tissue is susceptible to all the normal changes and disease spectrum seen in the normal breast. Breast cancer cases have been reported in accessory breast tissue.
The best policy is to try and avoid surgery, as it may cause unsightly scars, restriction of movement, cause pain and is not without complications [9]. Any surgery needs an experienced surgeon and careful preoperative marking. Scar placement for any surgery is vital; it should not extend beyond the edge of the pectoralis major.
Liposuction is useful for the fatty element of accessory breasts, and in some cases it is the only treatment required. Liposuction is also valuable in helping to define the planes between accessory breast tissue and the underlying axilla.
A combination of surgery for the glandular element and liposuction of the fatty element has been described. Excess overlying skin should be excised in cases of large accessory breasts.
In the postoperative period, seroma, incomplete excision, damage to intercostal-brachial nerves, painful scar and deformity due to excess removal of tissue are some of the complications of surgery [8].
Down et al. reported 0.5% of all patients referred to a breast clinic had accessory breasts [9]. In their series, 28 women had surgery, 11 experienced postoperative problems (two had seroma; two had residual tissue; two had intercostal nerve injury; five had poor scarring and one had an infection), thus suggesting high incidence of postoperative complications. Hence, the need to avoid surgery if possible.
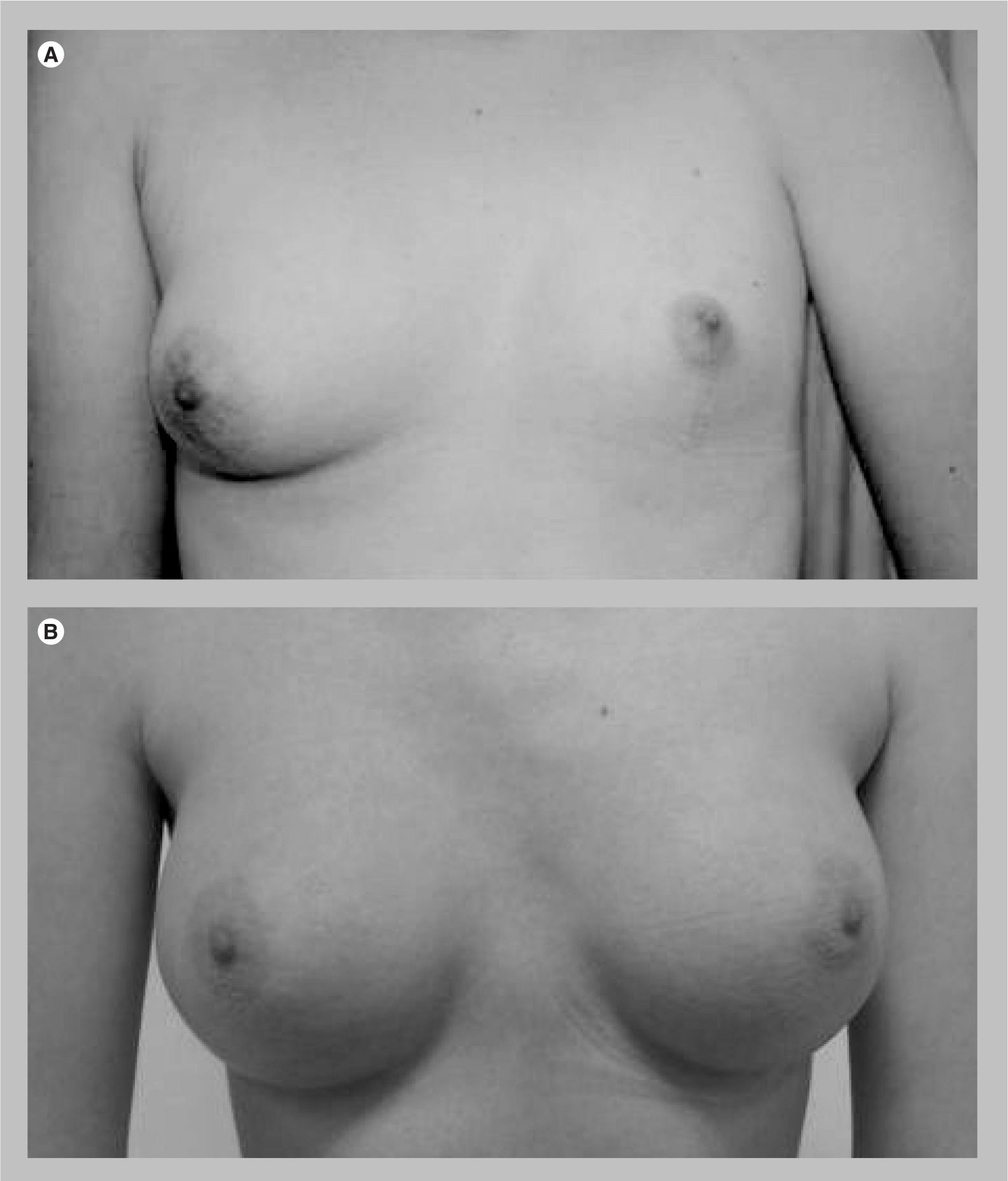
Asymmetry (aplasia & hypoplasia) of the breast
One breast can be hypoplastic or absent (aplasia) and this can occur in isolation or in association with a defect in (one or both) pectoral muscles. Some degree of breast asymmetry is common, but it is more pronounced in cases of hypoplasia (
This ‘true asymmetry’ can be treated with various treatment options, including augmentation of the smaller breast with implant, reduction and mastopexy of the larger breast, or a combination of both these options. Where there is asymmetry in the skin, the use of expanders prior to permanent implant replacement can improve symmetry. To get true symmetry, there is usually a need to operate on both breasts. The best age to perform surgery is when the breasts have fully developed – usually approximately at age 17 or 18 years. More than one operation may be required. Some hypoplastic breasts can also have a tubular element. Lipofilling (although controversial, its risks and benefits should be discussed with the patients) is useful to provide implant cover and improve contour to obtain a high degree of symmetry.
Amastia
The total absence of breast tissue and nipple–areola complex is called amastia (

Bilateral absence of breasts: amastia.
In amastia, the mammary ridge disappears completely or fails to develop. There is often evidence of associated ectodermal defects such as cleft palate, isolated pectoral muscle and upper limb deformities, urological abnormalities, and even Poland's syndrome. Familial cases have been reported with an autosomal dominant trait [6]. New breasts can be reconstructed using expanders and implants or using myocutaneous flaps such as the latissimus dorsi myocutaneous flap.
Abnormalities of the shape of the breast
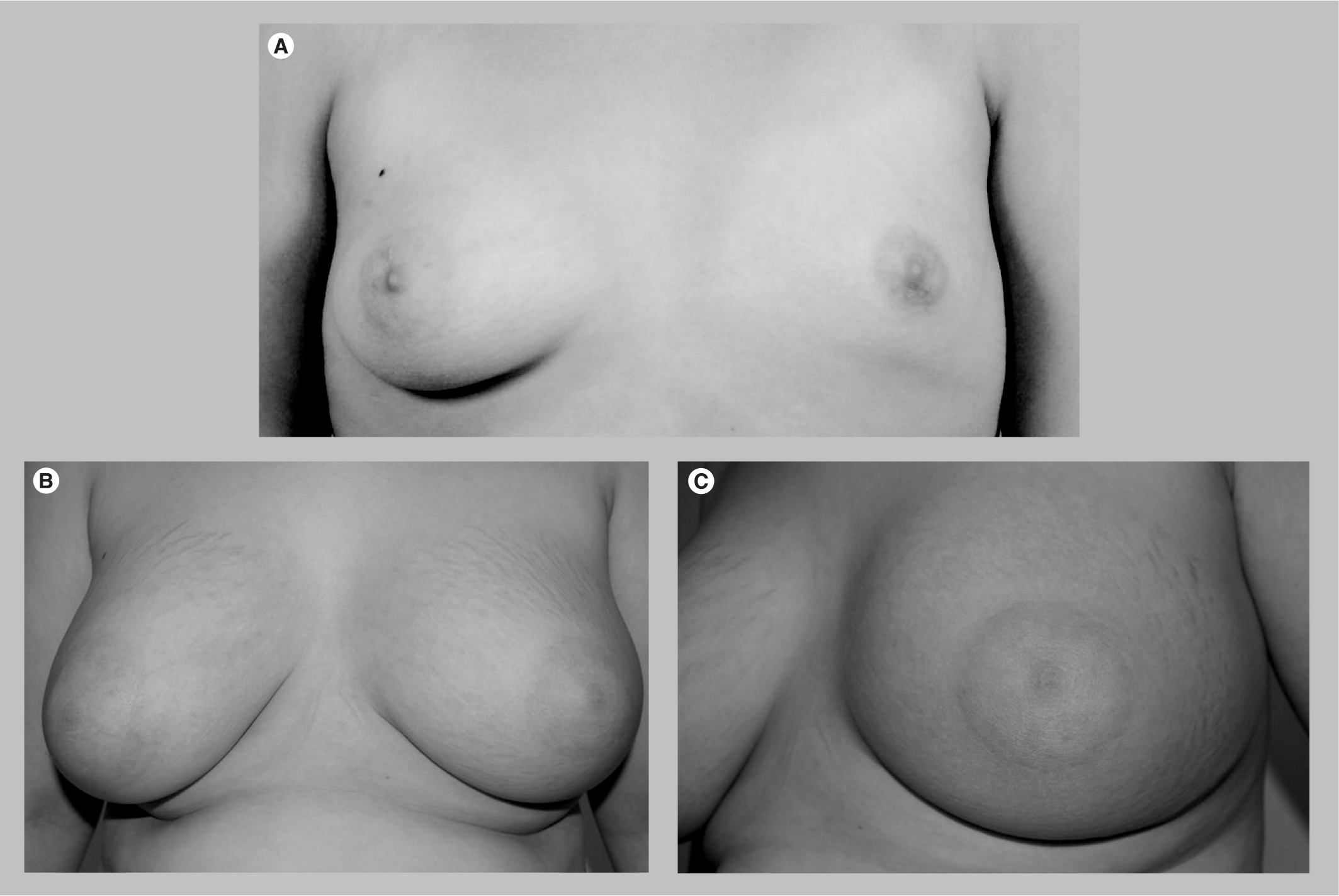
Tubular breasts
Tubular breasts are characterized by normal function/physiology of the breast tissue, but abnormal anatomical shape. It can be unilateral or bilateral, and the classical features include some or all of: lack of breast skin; breast hypoplasia and asymmetry; conical breasts; herniated nipple–areolar complex; large areola and a constricted breast base (

The first correction technique for tuberous breasts was described by Rees and Aston in 1976 [10]. They suggested widening of the constricted ring at the base of the breast tissue by radial scoring, essentially making cuts at the base of the breast from the centre, similar to the hands of a clock. Several similar techniques to expand the base width have been described since.
Standard treatment includes placement of expanders through an inframammary fold incision following radial scoring and later replacement with implants. These procedures do not correct the ‘herniated nipple and areola complex‘, and a second procedure is often required to correct this deformity, such as reducing the size by circular periareolar round block mastopexy (this could also be performed at the time of primary surgery in select cases).
The dual plane technique for tubular breast is now very popular. This technique differs from the subglandular position, in that the implant is placed in the subpectoral plane. The upper two thirds of the implant is covered by muscle and the lower third is covered by breast tissue. A short scar correction of the tuberous breast has also been described [11].
Lipofilling in the periphery of the breast (not recommended within the breast) helps to achieve a final better contour and adds volume along with the expander.
The long-term outcome from surgery is not always satisfactory with loss of sensation, scar issues and asymmetry being common complications.
Congenital chest wall deformity
Poland's syndrome
Unilateral chest wall hypoplasia with ipsilateral upper limb deformity is called Poland's syndrome (

Poland's syndrome in a man.
Poland's syndrome consists of some or all of: absence or hypoplasia of the breast; absence of pectoralis major or minor; absence of nipple; absence of adjacent muscles and sometimes costal cartilage; rib abnormalities; and upper limb deformities (e.g., syndactyly, micromelia or brachydactyly). Familial cases have been reported [13]. Poland's syndrome is three-times more common in males, with an incidence of one in 7000 to one in 1,000,000 in the general population. Pectus excavatum and Poland's syndrome, that include defects of the chest wall are the commonest forms of congenital chest wall defects. These defects can be corrected surgically [14].
Hypoplasia of the subclavian artery and its branches is thought to interrupt blood supply to the day 46 embryo and result in Poland's syndrome. Some evidence indicates a correlation between Poland's syndrome and carcinoma of underdeveloped breast and leukemia, but the frequency of this is not clear. Repair should be considered as a single-stage procedure in adults and two stages in children. Aplastic ribs can be reconstructed using bone grafts or prosthetic mesh. Muscle flaps and breast implants can be used to correct muscle and breast hypoplasia [15,16].
*Classification of Poland's syndrome
The classification described by Hartrampf in the 1980s does not consider upper extremity abnormalities; however, it is useful in deciding the type of reconstruction for correction (
Classification of hypoplastic breast abnormalities.
The aim of the treatment should be to achieve symmetry. Surgical procedures usually involve a combination of replaceable expanders (subsequently replaced by permanent implants), Becker expander/pros theses implants (shaped or round), placement of these devices in a dual plane (if the pectoral muscle is normal), and autologous muscle flaps such as latissimus dorsi flaps. The latissimus dorsi flap harvest can be performed endoscopically. The other more complicated procedures of autologous tissue reconstruction such as abdominal (i.e., transverse rectus abdominis myocutaneous and deep inferior epigastric perforators) or buttock (i.e., superior gluteal artery perforator or inferior gluteal artery perforator) flaps are usually reserved for more challenging cases.
Another option is to use rectus abdominus transverse rectus abdominis myocutaneous flap (free or pedicled). A two-flap technique including free and pedicled transverse rectus abdominis myocutaneous flaps for chest and breast reconstruction has been described [18].
Use of lipofilling and contralateral reduction/mas top exy improves long-term cosmetic results. The best time for operation is in the late teens, but operations can be performed from 11–12 years onwards to help with self esteem and normal psychological, social and sexual growth.
The management of these patients requires a multidisciplinary team approach, including pediatrician and plastic surgeon, to decide the optimum age for reconstruction. The future growth of the child should be considered in treatment planning [15].
*Anterior thoracic hypoplasia
Anterior thoracic hypoplasia is rare. It includes posterior displacement of ribs, anteriorly sunken chest wall, hypoplasia of the ipsilateral breast (always present), and a superiorly placed nipple and areola. The sternum and pectoralis major are normal. Treatment consists of augmentation mammoplasty using anatomical implants. The latissimus dorsi muscle flap is not usually considered, since the pectoralis major is present and normal.
Conclusion
Congenital abnormalities of the breast and chest wall are seen frequently in breast, pediatric and plastic surgery clinics. These cases often require a multidisciplinary team approach in their management. The spectrum covers a wide range of abnormalities from aplasia, asymmetry, underdeveloped breasts and abnormal shapes to accessory breasts/nipples [19]. The treatment for many of these conditions includes surgical correction, and considering the fact that the child is still growing, treatment timing is crucial, and many of the surgical corrective procedures require more than one operative procedure.
Although these deformities have less impact on functional capacity, the psychological consequences can be serious in adolescent patients. These patients can experience embarrassment, social isolation, and complexities in relationships and sexual development. The majority of these patients are young, healthy individuals, and the psychological and social impact of these conditions is significant.
The key steps in successful management are diagnosis, appropriate referral, avoidance of unnecessary investigations, a multidisciplinary team approach, psychological support, optimum timing of surgery and avoiding unnecessary surgery.
Congenital abnormalities can be corrected at a single surgical setting; however, a multidisciplinary approach and staged treatment is required for more complex deformities [4]. Timing of procedures is crucial as the development continues.
Scars, changes in the opposite breast and breast feeding are all related issues that need to be considered. Recent new technology and a better understanding of these conditions have brought subtle but important changes in the methods used to treat these abnormalities.
There has been a paradigm shift using anatomical implants rather than round implants and use of textured or polyurethane foam implants (not approved by the US FDA) rather than the smooth variety.
Liposuction for accessory axillary breast tissue is now an available mode of treatment for smaller sized tissues with a mainly fatty element. Even in larger accessory breasts it can be combined with excision and makes identification of the plane between normal and accessory breast tissue easier to find.
Lipofilling for hypoplasia and asymmetry achieves better shape and contour of the treated breast. This technique can be used in conjunction with implant surgery or as a primary treatment for a relatively small asymmetry. The trend is also to place expanders followed by anatomical/round implant for asymmetry, rather than using silicone gel implants alone as there is often less skin on the hypoplastic breast. The use of adjustable expanders/implants allows adjustment in the volume of the reconstructed breast.
The dual plane technique (placement of subglandular expander and then submuscular implant as a second-stage procedure) for tubular breast appears to give better results. It ensures that the expander stretches the breast tissue to widen the breast base. The permanent implant can then be camouflaged by placing it under the chest wall muscle. The pectoralis muscle is released, allowing for enhanced projection, shape and position.
A combination of implants and muscle or myocutaneous flaps are used in the reconstruction of chest wall deformities such as Poland's syndrome. The correction of unilateral chest wall deformities by perforator flaps (deep inferior epigastric perforators, superficial inferior epigastric artery and gluteal artery perforator) is an acceptable surgical procedure for reconstruction, with minimal donor site morbidity [20]. Endoscopic latissimus dorsi flap harvest for Poland's syndrome has been described and gives better cosmetic results and less scar tissue.
Mastopexy is sometimes needed and usually effective to correct breast contour without any volume change. This technique is used in the correction of tuberous breasts in Poland's syndrome following expansion and replacement with implants [18]. Mastopexy is also required in correcting hypoplasia; the skin of the normal breast is tightened, while that of the hypoplastic breast is expanded.
In summary, careful assessment of congenital abnormalities of the breast and chest wall is vital in a multidisciplinary setup. A thorough workup is recommended since many of these conditions are associated with other ectodermal defects. In the absence of any other abnormalities, selection of an appropriate corrective procedure is vital. These conditions often require multiple procedures, and the timing of treatment delivery is crucial. Many of these patients present at a very young age and need psychological support during the long course of treatment. With effective surgery, symmetry can be achieved and this can have a dramatic effect on these patients' lives. Given that most will live a normal life and live over 60 years, it is important to invest time and effort to get the surgery right to produce a good cosmetic result.
Future perspective
The advances in technology, such as implants and expanders, and application of new procedures, such as liposuction and lipofilling, to correct congenital abnormalities of the breast and chest wall has improved the outcome in recent years. There has been a paradigm shift using anatomical implants rather than round implants, and use of textured and polyurethane foam implants rather than the smooth variety. New operative procedures such as dual plane technique for tubular breast are being developed. These techniques appear to give better results.
These changes will continue to impact the way breast abnormalities are treated in the future.
Executive summary
Congenital abnormalities of the breast and chest wall are seen frequently in breast, pediatric and plastic surgery clinics. The spectrum covers a wide range of abnormalities from aplasia, asymmetry, underdeveloped breasts and abnormal shapes to accessory breasts/nipples.
Although breast deformities have less impact on functional capacity, the psychological consequences can be serious in adolescent patients. These patients can experience embarrassment, social isolation and complexities in relationships and sexual development. There are also functional problems encountered later in life with lactation and breastfeeding.
A thorough workup is recommended since many of these conditions are associated with other ectodermal defects. These cases often require a multidisciplinary team approach in their management.
The treatment for many of these conditions includes surgical correction, and considering the fact that the child is still growing, treatment timing is crucial, and many of the surgical corrective procedures require more than one operative procedure.
The key steps in successful management are diagnosis, appropriate referral, avoidance of unnecessary investigations, a multidisciplinary team approach, psychological support, optimum timing of surgery and avoiding unnecessary surgery,
Footnotes
Congenital abnormalities of the breast
To obtain credit, you should first read the journal article. After reading the article, you should be able to answer the following, related, multiple-choice questions. To complete the questions (with a minimum 70% passing score) and earn continuing medical education (CME) credit, please go to www.medscape.org/journal/wh. Credit cannot be obtained for tests completed on paper, although you may use the worksheet below to keep a record of your answers. You must be a registered user on Medscape.org. If you are not registered on Medscape.org, please click on the New Users: Free Registration link on the left hand side of the website to register. Only one answer is correct for each question. Once you successfully answer all post-test questions you will be able to view and/or print your certificate. For questions regarding the content of this activity, contact the accredited provider,