
Abstract
Implantation failure is common in assisted reproduction techniques (ART). The role of low-molecular-weight heparin (LMWH) is a matter of debate as a potential factor to improve implantation.
Keywords
The failure of a single IVF procedure is expected in nearly 70% of cases, independently of the presence or absence of thrombophilia [1–3] or other underlying diseases. A potentially equivocal problem related to data on the frequency of IVF failures in thrombophilic compared with nonthrombophilic women concerns the relatively high frequency of IVF failure. Furthermore, most studies demonstrate a variety of inclusion and exclusion criteria, pointing also to differences in ethnic background and selection criteria of control subjects.
While the association between thrombophilia and recurrent pregnancy loss is well-documented both for inherited and acquired thrombophilia [4], an association between thrombophilia and unexplained female infertility is still a matter of debate, especially for women with repeated failures of IVF and embryo transfer (ET) procedures [5,6]. The rate of thrombophilia in women with repeated IVF failures is reported as 50% in selected studies. However, several reports did not find a statistical significance when comparing patients to control subjects. Simur et al. selected 51 women with three or more IVF ET failures, finding thrombophilic defects in 62% of cases, without a statistical significance if compared with the control group (women with at least one uneventful pregnancy and without personal history of miscarriage) [7]. Martinelli et al. analyzed the relationship between thrombophilia and repeated IVF-ET failures in 162 women and found nearly 27% of inherited thrombophilic defects without statistical significance when compared with the control group (women with spontaneous and natural conception) [6]. Vaquero et al. described thrombophilia in 24% of subjects with IVF failures compared with 20 nonpregnant healthy fertile females, again with no statistical significance [8]. Regarding acquired thrombophilia owing to antiphospholipid antibodies Martinelli et al. did not find an association between patients with IVF-ET failures compared with controls [6], while Vaquero et al. found that 19% of women with IVF-ET failure had positive antiphospholipid antibodies versus none in the control group [8]. Qublan et al. found a significant increase in the frequency of inherited thrombophilic defects in patients with at least three implantation failures compared with two control groups; one of the patients had a birth with the first IVF attempt and a second group with natural conception; similar results were found for combined thrombophilia (i.e., the presence of two or more thrombophilic defects) [9]. Azem et al. found a relevant and significant increase of inherited thrombophilic gene variant's in women with recurrent IVF (four or more failures) compared with healthy controls [10], while Coulam et al. reported, a relevant increase of the PAI 4G/5G gene variant in a small population of women with recurrent IVF failure compared with healthy subjects, suggesting a possible role of hypofibrinolysis in this clinical setting [5], according to data reported by Glueck et al. [11]. Emerging data are available on homocysteine and folate metabolism and unexplained female sterility [12] and regarding the MTHFR C677T gene polymorphism in women with IVF failures [13].
Antithrombotic treatment based on the administration of prophylactic doses of low-molecularweight heparin (LMWH) has been suggested in recent years, however, only small and inconclusive studies have actually evaluated this treatment. Differences in populations analyzed seem to be relevant if subjects with thrombophilia are included in this kind of study. In 1998 Sher et al. reported improved outcome of IVF in women with antiphospholipid antibodies treated with LMWH and aspirin versus women treated with aspirin alone [14], while recently Qublan et al. reported an improved outcome of IVF in subjects with any type of thrombophilia treated with prophylactic doses of LMWH versus thrombophilic women not treated with LMWH [15]. However, Stern et al. did not find any type of improvement in outcome of IVF cycles in women with antiphospholipid syndrome treated with LMWH or aspirin versus not treated subjects [16].
The aim of this article is to evaluate the pregnancy rates in patients with repeated implantation failures undergoing assisted reproductive techniques (ART) with or without LMWH administration. Second to this we shall compare pregnancy rates according to the women's age and the presence of thrombophilia.
Materials & methods
We performed a retrospective observational analysis of patients with at least two failed IVF or intracytoplasmic sperm injection cycles with failed embryo implantation, screened for inherited thrombophilia and submitted to further ART cycles with or without administration of LMWH. All cycles were performed during the period the Italian Law 40 was in force. The law imposed the use of only three oocytes if available and the transfer of all fertilized oocytes. We selected the period that started from 8 March 2004 to 8 March 2009.
For this reason and according to data available in the literature on the avoidance of thrombotic complication during ovarian stimulation for IVF and on the possible improvement in the expression and production of coagulation components that participate in placental vascular development and differentiation as well in women developing pregnancy, we attempted to improve outcomes in IVF using prophylactic dosages of LMWH [17].
In this retrospective study, owing to the fact that LMWH is not recommended by guidelines, LMWH treatment was administered according to decisions made by the physicians.
In our database we analyzed women with infertility (i.e., primary infertility or secondary infertility owing to repeated pregnancy loss) who had been investigated for inherited thrombophilia to look for the following gene variants: Factor V Leiden (FVL), prothrombin G20210A and methylenetetrahydrofolate reductase (MTHFR) C677T. In this study we considered MTHFR C677T gene variant as a marker of thrombophilia according to other data reported in the literature on this topic. Based on these points we did not check for homocysteinemia in our population.
We selected 481 women who underwent 1154 ART cycles in two centers (Istituto Clinico Humanitas, IRCCS, Milan, Italy and San Matteo Hospital, Pavia, Italy) from 8 March 2004 to 8 March 2009. Women with under two implantation failures or with positive antiphospholipid antibodies and/or with antiphospholipid syndrome and who were not studied for the three thrombophilic mutations (FVL, prothrombin G20210A and MTHFR C677T) were excluded.
We analyzed 569 new ART cycles in 265 women who satisfied all the inclusion/exclusion criteria. Of 265 selected patients, 149 (56%) had primary infertility and 116 (44%) secondary infertility: eight had a history of recurrent pregnancy loss.
Data were collected on smoking habits, BMI, basal FSH recorded before controlled ovarian hyperstimulation (COH), number of retrieved oocytes, transferred embryos, implantation rate, pregnancy rate and LMWH administration.
We divided candidates for ART into two groups, according to the administration or not of LMWH; moreover based on the fact that women ≥36 years have a worse ART prognosis, we performed a subgroup analysis in women aged under 36 years.
Low-molecular-weight heparin was administered at a prophylactic dosage (i.e., enoxaparin 40 mg daily or nadroparin 80/100 IU/kg or dalteparin 80/100 IU/kg once daily), starting the day before COH until the day of β-human chorionic gonadotrophin testing. Patients who were not treated with LMWH were also included in group A while patients who received LMWH were included in group B.
Blood samples were collected by venipuncture, DNA was extracted using an automated procedure (MagNA PURE, Roche, Italy) and PCR amplification was performed with specific primers and Light Cycler apparatus (Roche, Milan, Italy).
A clinical pregnancy was considered according to the WHO definition and the implantation rate was considered as the number of intrauterine gestational sacs/embryos transferred.
Statistical analysis
Data were described as a number and percentage or mean and standard deviation where appropriate. Differences between groups were explored with Student's t-test, or χ2 test with Fisher correction when necessary, or Wilcoxon rank-sum test where appropriate. P-values were considered significant if <0.05. Statistical analysis was performed with Stata 10 [101].
Results
In our study population of 265 women at least one thrombophilic condition with one or multiple significant gene variants was present in 87 subjects (32%). Heterozygous Leiden mutation of FVL was present in seven (2.64%) women, heterozygous mutation G20210A of Factor II was present in 16 (6.11%) women. Homozygous mutation C677T of MTHFR was present in 61 (25.21%) women. We also found one homozygous Leiden mutation of FVL and two (G20210A) homozygous mutations of Factor II. One patient had a heterozygous mutation for both Factor V and Factor II, while three subjects were carriers of heterozygosity for FVL and homozygosity for mutation C677T of MTHFR; two subjects were carriers of heterozygosity for prothrombin A20210G and homozygosity for mutation C677T of MTHFR. Data are reported in
Incidence of inherited thrombophilia in selected women with two or more assisted reproductive techniques failures.

In a total of 569 ART cycles, 57 (10%) were performed in women with LMWH and 512 in women without LMWH. Mean age was 36.3 ± 3.4. All patients were divided into two subgroups, according to their age (with a cut-off point at 36 years).
Furthermore, no significant differences were found for other basic characteristics: FSH levels, smoking habits and BMI were similar in all groups.
Female age and the number of retrieved oocytes were statistically lower in cycles treated with LMWH, but the mean number of transferred embryos and the implantation rate was not significantly different between the two groups. Data are summarized in
Women undergoing assisted reproductive techniques with and without administration of low-molecular-weight heparin.

ART: Assisted reproduction techniques; LMWH: Low-molecular-weight heparin.
In women without LMWH pregnancy rate was 17.19 versus 29.82% in the group treated with LMWH (p = 0.020). For patients younger than 36 years the pregnancy rate was 20.00% (38/190) in the group without LMWH versus 24.14% (7/29) in the group with LMWH (p = 0.624). Among patients older or equal than 36 years pregnancy rate was 35.71% (10/28) if treated with LMWH versus 15.53% (50/322) if not treated with LMWH (p = 0.007) with a relevant significant difference between the two groups. Data are summarized in
Pregnancy rate according to age, thrombophilia and low-molecular-weight heparin.
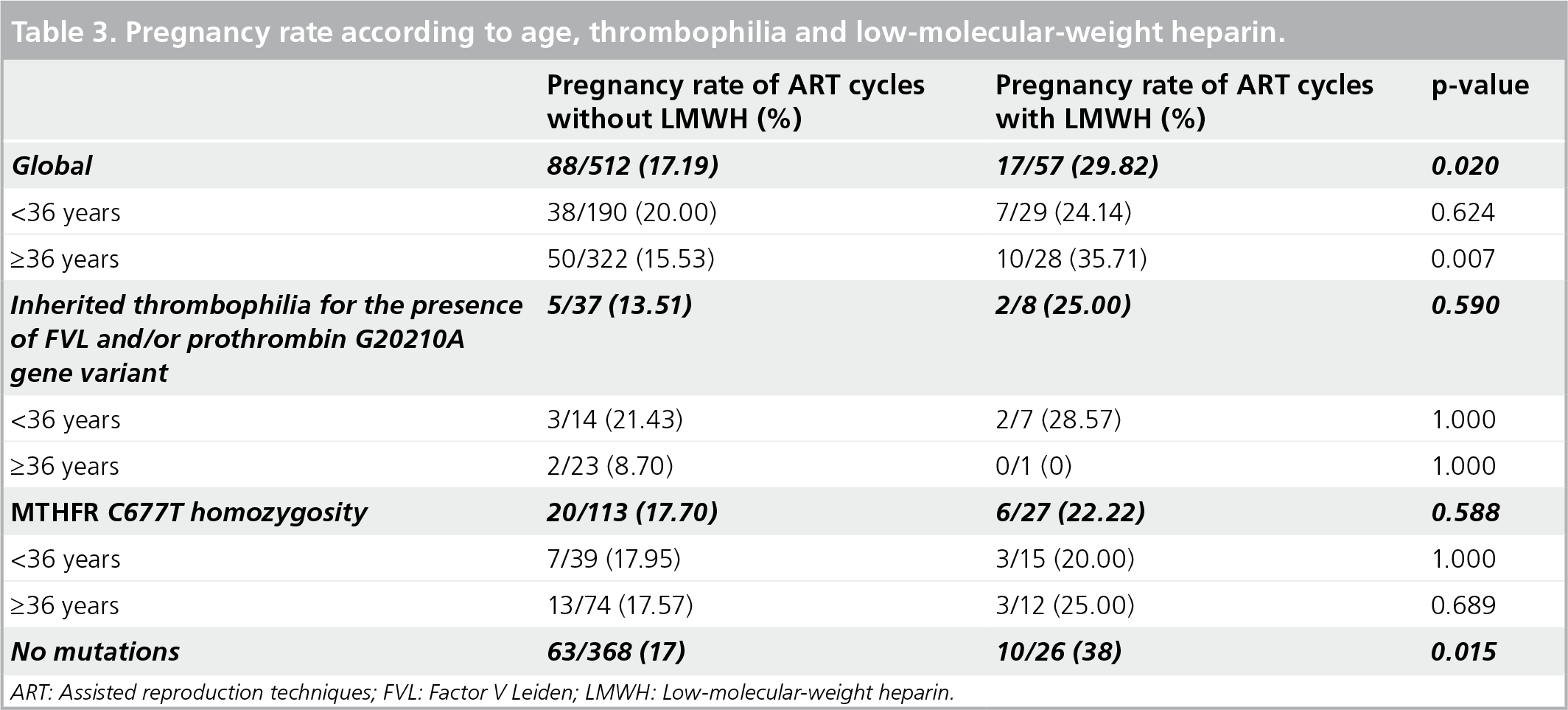
ART: Assisted reproduction techniques; FVL: Factor V Leiden; LMWH: Low-molecular-weight heparin.
Another subgroup analysis was performed according to the presence of one or more thrombophilic gene polymorphism. In the subgroup with the presence of FVL and/or prothrombin G20210A gene variant, pregnancy rate in patients without LMWH versus patients with LMWH was 13.51% (5/37) and 25.00% (2/8), not reaching statistical significance (p = 0.590). The presence of MTHFR C677T homozygosity resulted in no significant difference in the pregnancy rate in treated versus nontreated cycles. The pregnancy rate was 17.70% (20/113) in the group without LMWH and 22.22% (6/27) in the LMWH group (p = 0.588).
Data on women aged 36 years or over with thrombophilia undergoing ART with or without LMWH did not show statistical difference (16 vs 25%; p = 0.428), although these data may be influenced by the small number of selected patients. Data on women younger than 36 years with thrombophilia undergoing ART with or without LMWH did not show statistical significance (19.6 vs 21.0%; p = 1.000). In patients with no mutations, the pregnancy rate without LMWH was 17.11% (63/368) and 38.46% (10/26) with LMWH, reaching statistical significance (p = 0.015).
Discussion
Repeated implantation failures in infertile patients submitted to ART cycles is a complex problem owing to the different factors involved in embryo development and implantation. Nearly 85% of human embryos [18] and over 50% of pregnancies ending in a spontaneous abortion after an IVF procedure [19] present a chromosomal abnormality, although several other cofactors might play a significant role [20,21]. Thrombophilia has long been suspected to be one of them. Yet, according to recent data, failure of IVF seems not to be influenced by the presence of inherited thrombophilia and our data seem to confirm this role
Furthermore, heparin can alter the hemostatic response to controlled ovarian stimulation and modify the risk of thrombosis in women, with or without inherited thrombophilia, undergoing ART cycles with pharmacological ovarian stimulation. Heparin may modulate some of the fundamental physiological processes required for blastocyst apposition, adherence and implantation as well as trophoblast differentiation after an ART cycle owing to its similarities to heparan sulfates, and heparin has the potential to improve pregnancy rates and outcomes although this concept is not yet supported by prospective randomized trials.
No guideline suggests a type of pharmacological nonhormonal support for women who have experienced several ART failures and even in recurrent miscarriage, a recent randomized trial reported no positive effect of heparin administration [27]. Our retrospective analysis was performed on selected women who had experienced at least two ART failures, and who were candidates for a new ART cycle. There was no increase in the rate of inherited thrombophilia in the patients studied and this observation confirmed the result obtained in unexplained infertility [28].
A marked difference was found between women who underwent ART and who are over 36 years old, although the number of retrieved oocytes was reduced in patients who underwent ART with LMWH. Interestingly, although the reduced number of retrieved oocytes was significantly lower in women who underwent ART with LMWH, we found a better outcome in ART. A prophylactic dosage of LMWH (i.e., enoxaparin 40 mg daily or nadroparin 80/100 IU/kg or dalteparin 80/100 IU/kg once daily), improved the outcome in women over 36 years, with previous repeated ART failures. Moreover, this improved outcome seems to be independent of the presence of inherited thrombophilia, thus pointing to the potential role of LMWH for ART in this group of patients or even in all ART [29,30] if the suggestions of a possible role in normal placentation and positive embryo–fetal development will be confirmed.
LMWH use could improve the invasion of maternal vessels by syncytiotrophoblasts thereby reducing local microthrombosis at the site of implantation leading to the implantation failure more common in older women.
The present study points to a potential role of antithrombotic treatment in women over 36 years of age scheduled for ART. A prospective randomized trial on LMWH in this group of patients is highly recommended and would support scientific evidence for future clinical applications, initially studying randomized groups based on age and then examining clinical subsettings such as thrombophilia.
Future perspective
Antithrombotic treatment to improve the outcome of ART is frequently a matter of discussion. The role of aspirin and LMWH in this clinical setting should be better evaluated. Our experience with a retrospective analysis in fact demonstrated an improvement of pregnancy rate in patients treated with LMWH. The use of LMWH for ART cycles should be tested in randomized trials in order to establish if it may improve the outcome of ART per se.
Executive summary
Antithrombotic treatments have been suggested to improve the outcome of assisted reproductive techniques (ART).
Thrombophilia has been suggested as a possible cause of ART failure.
A retrospective study designed to establish the efficacy of low-molecular-weight heparin (LMWH) to improve ART.
A retrospective observational analysis of patients with at least two in vitro fertilization/intracytoplasmic sperm injection cycles with implantation failure.
The outcome of ART performed with or without administration of LMWH was observed.
Inherited thrombophilia was investigated by looking at for several gene abnormalities.
LMWH seems to improve the outcome of ART in women with advanced age.
LMWH does improve the outcome of ART in thrombophilic women.
No thrombotic events have been associated during ART procedure in patients treated with LMWH.
Footnotes
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.