
Abstract
Although multiple sclerosis (MS) affects both women and men, women are more susceptible to MS than men. Accumulating evidence indicates that the incidence and prevalence of MS is increasing, more so in women than in men. Owing to pregnancy, differing hormonal states and distinct social roles, the impact of MS differs between women and men. Since Patricia K Coyle published a review on gender issues in MS, multiple studies have added to the body of knowledge. This update will summarize the current thinking on gender-related issues in MS and we will address incidence and prevalence, hormonal factors, pregnancy and breastfeeding, genetics, course and prognosis, imaging, treatment and psychosocial aspects. Future progression within this field will help elucidate the cause of and define the treatment of MS.
Keywords
Gender issues in multiple sclerosis (MS) are at the forefront of current research since Patricia K Coyle authored a paper on the matter [1]. The reader is advised that this paper will be an update of that previous document. The most striking new data involves accumulating evidence for an increasing incidence and prevalence of MS over the last decades, particularly among women [2]. The ratio of women to men (hereafter designated as the sex ratio), during the course of the 20th century has increased from 1:1 to 3.5:1 according to Ebers [2]. Such a rapid rise cannot result from genetic mutations, which require time. It presumably reflects changes in the environment (internal or external), the identification of which should shed considerable light on the cause(s) of MS. We will also review new data on the sexual dimorphism of the brain (for humans and mammals), on the genetic underpinning of MS, on pregnancy and breastfeeding, on cognition, on imaging, on treatments and on psychosocial issues. The importance of the cross-talk between hormonal, immune and nervous systems is increasingly recognized.
Epidemiology
It is still unknown whether MS is a primary immune-mediated disorder. No critical auto-antigen target has ever been identified, and it remains possible that MS could represent a persistent infectious, metabolic or neurodegenerative process [3]. Nevertheless, as is usual for most autoimmune/immune-mediated disorders, MS is more common among women than among men.
Incidence
In 2008, a systematic review on the temporal trends in MS incidence (based on 38 studies published between 1966 and 2007) reported an overall incidence rate of 3.6 per 100,000 persons per year in women, versus 2.0 in men. The incidence of the sex ratio had increased over time, from 1.4 in 1955 to 2.3 in 2000 [4]. For each 5-year period the incidence of the sex ratio increased by 6%. The highest incidence was recorded in an Italian study (12.4 per 100,000 person-years in women and 7.0 in men). The age-adjusted rates used the world population as standard [4,5]. The highest sex ratios were obtained in Australia, European countries (Finland, Scotland, England, Italy, Spain and Yugoslavia) and in the USA. No Canadian study was included in that review [4]; however, the situation is similar in Canada [6]. Other studies also report an increasing incidence of MS in women, with either a lower increase [7–20], stabilization [21–25] or even decreased incidence in men [26]. Environmental factors would probably explain this change, since no new genetic input has been observed in these populations.
Prevalence
The overall prevalence of MS has also increased. A systematic review conducted in 2001 found 400 prevalence studies. The ability to compare prevalence studies depends on several factors, including the variability of the surveyed populations (e.g., size, age, structure, ethnic origin and composition), the thoroughness of case ascertainment, and the criteria used for diagnosis [27]. Greater survival will contribute to increasing prevalence [28]. Even when taking all of these factors into account, they are insufficient to explain the growing prevalence of MS cases worldwide, since initial studies in 1929. This increase has been attributed in large part to an increased incidence/prevalence in women [28].
From 1870 to 1910, opinions varied on whether men or women were more affected by MS [29]. In 1921, Wechsler analyzed 1970 patient records, and concluded that men were more frequently affected than women by a ratio of 3:2. By 1940, almost all studies agreed that women were more affected. A slightly higher incidence in women was reported by Schumacher in 1960 [29]. In a study published in 1980, women represented 60% of MS patients (n = 349) [30].
Most studies from Canada [13,28], the USA [22,31–33], Italy [9], the UK [23], France [24], Norway [10], Finland [12], Denmark [25], Australia [21,34], Japan [35] and South America [36,37] report an increase of MS prevalence solely, or predominantly among women, resulting in a higher sex ratio. Only one small study reported a decrease in sex ratio among MS patients

Evolution of women:men MS ratio over time.
The Canadian Collaborative Project on the Genetic Susceptibility to MS (CCPGSMS) reviewed a cohort of 29,478 MS patients (21,054 women and 8424 men) born between 1891 and 1993, and analyzed sex ratios by years of birth. It was found that with each year the sex ratio increased by a factor of 1.014, which corresponds to a 0.85% increase per year. The MS sex ratio changed from 1.90 to 3.21 in births between 1931–1935 and 1976–1980, and is now expected to exceed 3.5. Logistic regression analysis showed the year of birth to be a significant predictor for sex ratio [28]. The same group compared sex ratios by year of birth among immigrants versus Canadian-born individuals. The approximate overall percentage rate increase every 10 years was 3.13% for the former, and 2.82% years for the latter. Earlier age at migration resulted in a higher sex ratio, highlighting the impact of environmental factors on MS risk [6]. Two other groups used a similar methodology and reached concordant results.
In summary, accumulating data documents an increased incidence and prevalence of MS overall over the last 5 decades, especially in countries with a high prevalence. The increase seems mostly related to an increased susceptibility among women. These shifts supersede changes in diagnostic methods, access to care or referral patterns, and cannot be attributed to genetic factors. Understanding why these changes occurred would shed light on the causes of MS.
Latitudinal gradient
A latitudinal gradient has been widely reported for MS [41–47]. Recently, however, it has been questioned [4,22,27,32,48]. When looking at differences between sexes in this gradient, a review conducted in 2008 reported that before 1980 a 10° increment in latitude was associated with a 31% increase in MS incidence among women, and a 54% increase among men. After 1980, the corresponding numbers were 15% among women and 11% among men [4]. The latitudinal gradient parallels the degree of sun exposure, and has been attributed to vitamin D deficiency.
Basic biology
Sex hormones
Mammalian sexual differentiation was assumed to be initiated by the presence or absence of the testis-determining factor SRY, encoded on the Y chromosome. SRY induces the production of testes, which secrete the hormones responsible for male secondary sexual differentiation. However, female development is not only carried out by default, since recent studies suggest that both Y and X sex-chromosomal primary mechanisms of sex determination are involved. In addition, sex-chromosomal genes can influence not only the development of nongonadal secondary sexual organs, but also of other organs such as the brain.
Sex hormones are essential for neural circuit development [49]. Testosterone activates the androgen receptor. It is converted into estrogen in the brain via aromatase, or to dihydrotestosterone by 5α-reductase. Estradiol and dihydrotestosterone then act on estrogen and testosterone receptors respectively, to shape the brain. Extensive sexual dimorphism has been demonstrated in the number and projections of aromatase-expressing neurons. The masculinization of these cells is independent of androgen receptor, but can be induced in females by testosterone or estrogen, indicating a role for aromatase in sexual differentiation of these neurons. In addition to hormones from the gonads, both male and female adolescents (and adults) are exposed to androgens from the adrenals, such as dehydroepiandrosterone. While sex hormones undoubtedly play an important role in the sexual differentiation of the brain, other mechanisms may be involved in this phenomenon. Indeed, the identification of genes differentially expressed in male and female mouse brains, even before formation of the gonads, suggests that genetic factors may also influence the sexual differentiation of the brain. One example of this is the expression of several Y-linked genes (e.g., Usp9y) in the brain of male and XY female mice [50].
Gender differences in the hypothalamic–pituitary–adrenal axis (HPA) are recognized in animals and humans. In response to a psychological stressor, HPA responses are generally greater in males than females. The impregnation of the brain by gonadal hormones during the perinatal period helps shape the HPA sexual dimorphism, which is maintained in the adult by gonadal steroid hormone levels. It is recognized that stress and HPA, through release of catecholamines and glucocorticoids, affect major immune functions such as antigen presentation, leukocyte proliferation and trafficking, secretion of cytokines and antibodies [51]. Susceptibility to autoimmune disease may be related to an impaired responsiveness of the HPA axis. Stressors (e.g., an infection) are known to increase risk of MS relapse.
The immune system is also powerfully modulated by gender both early in development and during the perinatal period, when sex steroid hormones may permanently alter the developmental pattern of the T-cell repertoire in the thymus. Indeed, the immune system of adult males and females exhibits differences in anatomy, cytology, immunoglobulin levels and responsiveness. In animal models, females have a greater resistance to tolerance induction, as well as more pronounced tumor allograft rejection [52]. Several immune genes are believed to be under the strong influence of sex hormones. The control of regulatory T-cell development can be considered as one of the key immune components of this sexual dimorphism.
Prolactin
Prolactin (PL) is a mammotropic neuropeptide, produced by the pituitary gland as well as extrapituitary tissues (e.g., the endometrium, and cells of the immune system). It belongs to the growth and lactogenic hormone family, which includes growth hormone and placental lactogens. Pituitary PL secretion is under hypothalamic control. The cytokines IL-1, IL-2 and IL-6 also stimulate PL production, while IFN-γ and endothelin-3 are inhibitory. The gene coding for PL is close to the MHC complex on the short arm of chromosome 6. PL regulates reproduction, osmoregulation, and behavior, and has potent immunomodulatory effects. PL increases the expression of costimulatory molecules, as well as cytokine secretion from T, B, natural killer and dendritic cells. The high circulating concentrations of estrogen during late pregnancy also promote prolactin secretion. As for sex steroid hormones, prolactin levels fall after birth but are restored during breastfeeding. Breastfeeding has been shown in one study to reduce relapse frequency, and this has been related to the duration of amenorrhea [53]. PL also promotes oligodendrocyte precursor proliferation and stimulates myelin repair in mice [54]. PL may then act to reduce disease activity by protecting myelin and enhancing repair [54], presenting a potential new therapeutic avenue. A case has been reported in which a man with optic neuritis was found to have a PL-secreting pituitary adenoma. Pharmacological treatment of the adenoma resulted in a 12-year remission. The ensuing clinical and MRI relapses were concomitant with a surge in the plasma levels of PL [55]. This case indicates that PL can have proinflammatory effects. Other factors during pregnancy, in addition to estriol, exhibit anti-inflammatory properties, namely pregnancy-specific glycoproteins, α-fetoprotein, early pregnancy factor and relaxin (an estradiol-binding protein with immunoregulatory functions).
Leptin
Leptin is a pleiotropic hormone produced primarily by adipocytes, T cells and neurons. Its serum levels are approximately three times higher in females than in males. Sex steroid hormones, testosterone in particular, are significant determinants of the sex difference in serum leptin levels. Leptin may contribute to experimental allergic encephalomyelitis (EAE)/MS pathogenesis by acting as a proinflammatory cytokine promoting regulatory T cell anergy and hyporesponsiveness, leading to increased Th1 and reduced Th2 cytokine production. In relapsing-remitting multiple sclerosis (RRMS) patients (men and women analyzed together), circulating leptin levels are increased, and the Treg population is decreased. Leptin plasma concentrations are proportional to the amount of fat tissue, so obese individuals produce higher levels of leptin. The increasing MS prevalence in women may partially be linked to the worldwide increasing prevalence of obesity [51]. Obesity at 18 years of age has been reported to double the risk of MS [56].
Protective effects
Testosterone
There is evidence for a protective effect of testosterone on the CNS (reviewed in [52]). Testosterone reduces the production of inflammatory cytokines such as TNF-α and IL-1β by human macrophages. Naive T cells stimulated in vitro with CNS autoantigens, in the presence of testosterone, produce higher levels of IL-5 and IL-10, but decreased levels of IFN-γ, indicating a Th2-like shift. Testosterone crosses the blood–brain barrier, and can directly influence neural cells. Testosterone can protect from glutamate toxicity, induce neuronal differentiation, increase neurite outgrowth and protect from oxidative stress in neuronal cell lines. Neuroprotective effects of testosterone might be mediated through an increase in the expression of neurotrophic factors such as brain derived neurotrophic factor. These neuroprotective effects have been reviewed previously [57].
Estrogens
Numerous reviews have described estrogen's neuroprotective effects [58,59]. Protective mechanisms of estrogen treatment (both estriol and estradiol) in EAE depend on anti-inflammatory mechanisms. Estrogen treatment has been shown to affect cytokines, chemokines, matrix metalloproteinase-9, antigen presentation and dendritic cell function. Estrogen treatment also induces Tregs in EAE. Studies using estrogen receptor (ER)-α deficient mouse strains have shown that clinical protection from EAE by estrogens depends on signaling through ERα. In vitro estrogens protect neurons in models of neurodegeneration, whether induced by excitotoxicity or by oxidative stress. Estrogens decrease glutamate-induced apoptosis, preserve electrophysiologic function in neurons, protect oligodendrocytes from cytotoxicity, accelerate oligodendrocyte process formation, and increase dendritic spine formation and synapses on CA1 pyramidal cells of the hippocampus in rats, resulting in improved memory. In vivo studies have shown that estrogen treatment can be neuroprotective in animal models of Parkinson's disease, cerebellar ataxia, late onset leukodystrophy, stroke and spinal cord injury, often acting to reduce apoptosis.
Estrogens also exert genetic effects by regulating gene transcription by nuclear receptors, ERbα, and ERbβ, which are expressed in both the immune system and the CNS. In addition to the nuclear ERs, plasma membrane-associated ERs mediate the nongenomic signaling pathway. Anti-inflammatory mechanisms of estrogens have been found to be mediated by ERα. Selective ERα ligand treatment also decreased CNS infiltration in EAE, whereas a selective ERβ ligand had no effect. Estriol treatment effects on metalloproteinase-9 bioactivity, and CNS infiltration by T cells and monocytes in EAE were also mediated via ERα.
Treatments with sex hormones
It has been suggested that sex steroid supplementation could be beneficial owing to their immunoregulatory, anti-inflammatory and neuroprotective properties. Treatment with testosterone in men with MS was associated with an improvement in cognitive performance and slowing of brain atrophy, but had no effect on gadolinium-enhancing lesion numbers. Treatment with estriol in women with MS did have an effect on enhancing lesions [60]. Further clinical trials are underway. Several new steroid hormone analogs and synthetic selective estrogen response modulators are being developed, such as selective ERα and ERβ agonists and ER modulators, lacking the undesired uterotropic activity. Such studies could result in the design of new sex steroid-based therapeutic approaches to MS.
Genetic aspects
Epigenetics
The phenotype of an individual results from complex interactions between genotype and current, past, and ancestral environmental events (reviewed in [60]). These events result in a lifelong remodeling of our epigenomes. The vast majority of common diseases (e.g., atherosclerosis, diabetes, osteoporosis, asthma, and neuropsychological and autoimmune diseases), which are often initiated in early development, display some degree of sex bias, which can be very pronounced. This bias could be explained by the role of sex chromosomes, the different regulatory pathways underlying sexual development of most organs and the lifelong fluctuating impact of sex hormones. A substantial proportion of dimorphic gene expression might be under the control of sex-specific epigenetic markers. Environmental factors such as social behavior, nutrition and chemical compounds can influence, in a gender-related manner, these flexible epigenetic marks. Unfavorable programming could lead to various defects, along with a differing susceptibility to diseases between males and females [60].
All human tissues contain the same 25,000 genes [61]. However, only a few of these genes are expressed in a given tissue, giving rise to the phenotype. To ensure proper gene expression, the epigenetic code comprises several codes: the DNA methylation code, the histone code (histone methylation, acetylation and phosphorylation), and the coregulator code, which ‘orchestrate’ the activity of the genome, together with RNA interference. Imprinting is one of the epigenetic mechanisms occurring in the gametes. In these cells the inherited imprints are erased and a new one, which is maternal or paternal specific, is established. Parental imprinting uses DNA methylation and histone modifications for monoallelic expression of certain genes. The expression of these imprinted genes is then determined according to their parent of origin. Imprinting affects between 90 and several hundred genes. Imprinted genes are particularly involved in embryonic development and metabolism, and imprinting deregulation is linked to cancer, obesity, diabetes and behavioral disorders, such as autism and bipolar disease. Recent studies suggest that this epigenetic programming could sometimes be transmitted to subsequent generations in a sex-specific manner and lead to transgenerational effects. The risk of developing complex disease in offspring often depends on the sex of the affected parent. There is a clear parent-of-origin effect in MS: the risk for maternal half-siblings is 2.35%; it is 1.31% for paternal half-siblings. A similar effect has been shown in avuncular pairs (uncles/aunts and nephews/nieces pairs).
The Carter effect stipulates that the sex with the lesser susceptibility transmits the disease more frequently, because of an increased genetic load. Some studies support this concept [62–64], however, evaluation of disease transmission according to sex in the large cohort of the CCPGSMS concluded that MS is transmitted mostly through women [65].
Genetic markers
Several genome scans have been published in MS cohorts. The strongest association is with the following extended MHC-susceptibility haplotype: HLA-DRB5*0101-HLA-DRB*1501-HLA-DQA1*0102-HLA-DQB1*0602. With this haplotype, the risk is increased by three for heterozygotes, and by six for homozygotes. There is a gender imbalance: 63% of women with MS carry this halotype, compared with only 53% of men with MS [65]. This implies that genetic susceptibility factors are sexually dimorphic. A study associated this haplotype to a more severe phenotype of MS, including: reduction in N-acetyl-aspartate within normal appearing white matter on MR spectroscopy (an index of neuronal degeneration); increase in volume of white matter lesions; reduction in normalized brain parenchymal volume; impairment in cognition; and a younger age at onset [66]. The HLA-DR2DQ6 haplotype has been recognized to confer susceptibility to MS, and is more common in women than in men [67].
Two CD95 polymorphisms (which participate in the apoptosis process, thus regulating clonal expansion of T cells outside the thymus) may account for 28% of the risk among homozygote women; by contrast, they do not increase the risk of MS in men [68].
The SNP rs2069727, adjacent to the 3′UTR region of the IFN-γ gene, is associated with MS in men only; this effect is stronger in homozygotes than in heterozygotes. Women with MS have higher IFN-γ expression and lower IL-5 levels in response to in vitro proteolipid protein stimulation than men with MS or women controls. This IFN-γ SNP is then associated with sex bias in MS susceptibility and with expression of IFN-γ in MS. Among its pleiotropic effects, IFN-γ induces dendritic retraction and inhibits synapse formation. In a variety of physiologic and disease states, IFN-γ levels vary by sex. A common sex-dependent mechanism may influence a variety of disorders characterized by chronic inflammation in which IFN-γ plays a pivotal role [69]. Despite the marked female predominance in MS, no genetic marker has yet been identified on the X chromosome [65].
The gender gap in MS may be due to the effects of sex hormones, genetic differences, or a combination of the two. A nonmutually exclusive alternative hypothesis includes a direct genetic effect on the immune system and/or the CNS. Specific gene products, which are not induced by gonadal hormones but are expressed in a sexually dimorphic manner, could induce gender differences in MS pathogenesis and progression.
Microchimerism
Microchimerism had been suggested as a possible mechanism in MS. More recent studies, however, have not reproduced the earlier findings of an increased frequency of chimeric cells in MS patients [70].
Genetic counseling
Genetic counseling can now be approached in a systematic manner. When considering pregnancy, MS patients and their spouse should consider factors enumerated in
Considerations for parenthood in patients with multiple sclerosis.

MS: Multiple sclerosis.
Among Caucasian populations, the rate of acquiring MS varies from 1–2 in 1000 people. A total of 20% of MS patients will have another affected individual among their family members. MS is not transmitted in a Mendelian pattern, although the risk is proportional to the degree of gene-sharing. Children from families with a bilinear history of MS have the maximum risk of MS. The risk then gradually decreases in the case of the homozygotic twin (although the risk is higher if the twins are female), then in the case of children born to consanguineous parents, then the heterozygotic twin, and continues to decrease in the cases of first-, second- and third-degree relatives of the affected individual (see
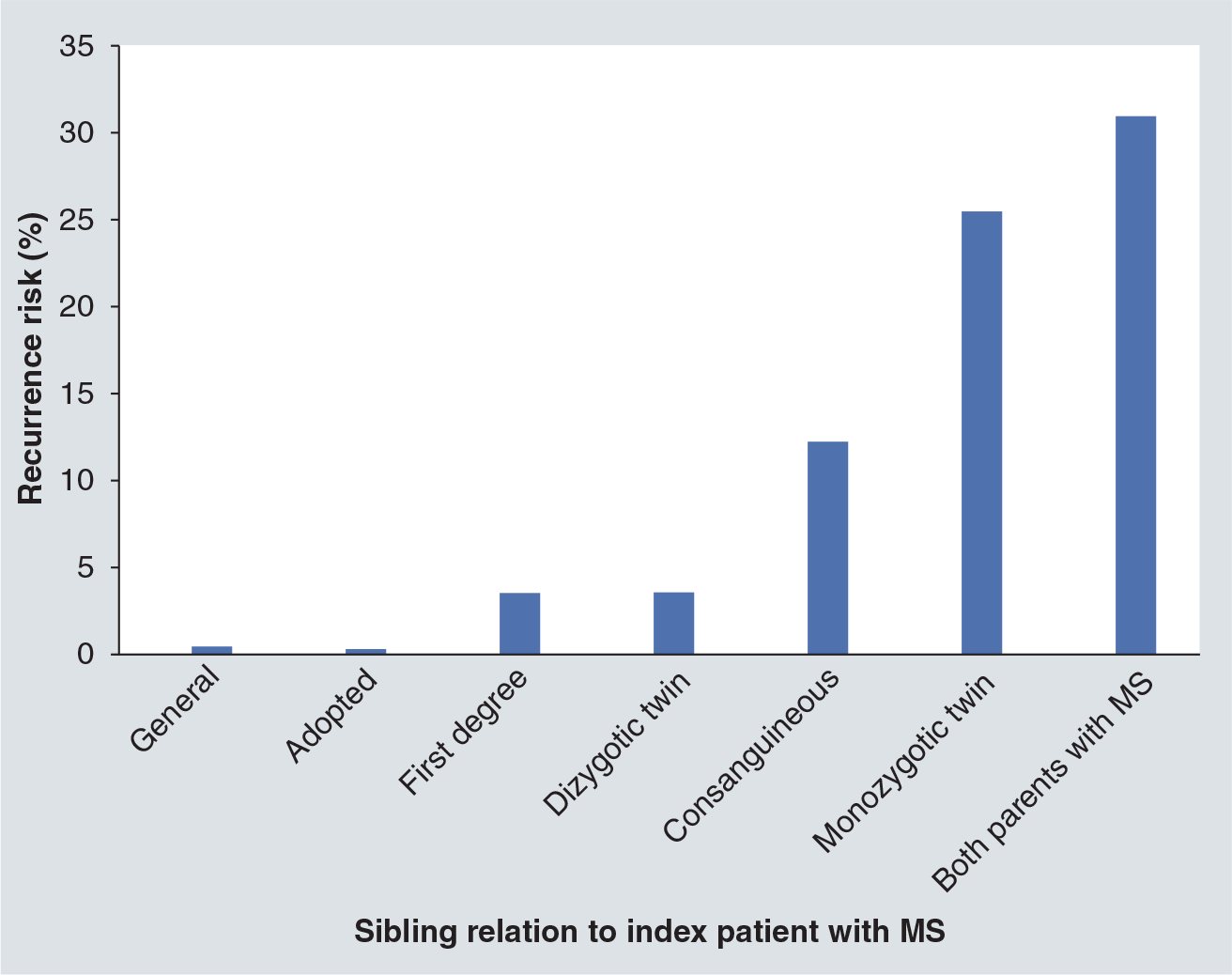
Risk transmission.
It is uncommon (estimated at 20%) for MS patients to renounce having children because of the risk of disease transmission; some would rather consider adoption. Pregnancy issues are discussed later in a separate section. Documentation on the possible consequences of MS therapies on children born to parents with MS does not exist at present. A prospective MS pregnancy registry is currently in preparation.
For an individual with MS, parenthood must be considered thoughtfully. We advise patients to wait a few years after disease onset, allowing time to gauge prognosis, and to make sure that their marital situation is favorable. In women with active disease before or during pregnancy, it is probably advisable to start treatment right after delivery. For further discussion on this aspect, the reader is referred to the ‘Impact of pregnancy on MS’ section.
Environmental factors
Vitamin D deficiency is endemic in cities in northen Canada [9]. No direct evidence from affected adults implicates early-life vitamin D exposure in susceptibility to MS. The increased prevalence of MS among people born in May, might reflect maternal end-of-winter deficiencies in vitamin D. A model integrating vitamin D into genetic and environmental susceptibility in MS postulates that vitamin D epigenetically modifies genes important in the development of the brain, immune system, or development of axonal resilience or immunological tolerance [2]. Vitamin D deficiency has been implicated in the likelihood of developing autoimmune diseases. Autoimmune diseases are more prevalent in women, raising the possibility that women have lower vitamin D availability, or that gender differences in the physiological responses to vitamin D may be present. Interestingly, gender-specific differences in vitamin D metabolism are reported. Besides its calcium homeostatic role and antineoplastic properties, vitamin D is involved in the development and the maturation of immunity [72].
Several studies have established that smoking increases the risk of MS [73]; in some, smoking worsens disease course. Rodriguez Regal et al. conducted a study on 138 MS patients and found that smokers and ex-smokers had a 27% increased risk of developing MS [74]. The relation was found to be significant for women but not for men.
Clinical presentation
Diagnosis delay
The mean duration between clinical onset and diagnosis of MS in Canada is the same for men and women, with a mean of 3 years in each group [28]. These data are based on a cohort of more than 26,000 patients (from CCPGSMS), with a mean age at onset of 30 years [75]. In a group from Sicily, Italy, the mean time from onset to diagnosis was 4.0 ± 4.6 years – almost the same for men and women – in a population of 288 patients with a mean age at onset of 31.4 years [19].
Age at disease onset
Approximately 70% of patients experience MS onset between the ages of 20 and 40 years [76], and 90% experience onset between the ages of 15 and 50 years [1]. The mean age at onset is approximately 28–30 years [77], with a mean age earlier in women than in men. In recent Canadian data [65], age at onset is approximately 32 years in women and 33.5 in men. Onset in men coincides with declining levels of testosterone [77,78]. Onset in primary progressive multiple sclerosis (PPMS) occurs approximately 10 years later than RRMS [77], at approximately 38–41 years of age, compared with 28–30 years of age for RRMS [1].
Course of the disease
Gender influences MS course (see Coyle [1]). In concordant parent–child pairs with MS, male offspring of affected fathers are more likely to have PPMS (odds ratio [OR]: 1.92) [79].
Two large cohort studies observed that 80–87% of MS patients have the RRMS course initially [80–82]. RRMS is characterized by female preponderance with a sex ratio of 3:1 [78,83–85]. A relapsing course is followed by secondary progression in some 70–80% of cases over a 2-decade period [80,82]. The sex ratio in secondary progressive multiple sclerosis (SPMS) is 3.2:1 [84,86]. Time from onset to SPMS was found to be twice as long as previously described [87,88]. Despite this result, male gender has been associated with a greater risk of developing SPMS [89]. Evidence differs on whether gender can influence the timing of secondary progression. Two studies found no influence [87,90], while another showed that men reached SPMS earlier (mean time from onset to SPMS was 9.6 years for men and 12.8 years for women), and with a higher expanded disability status scale (EDSS) score [91].
A review of nine studies assessing prognostic factors for benign MS concluded that 26.7% of MS patients had a benign course and female sex gave an OR of 1.28 (95% CI: 0.94–1.73) for this course [92]. A benign course is more often associated with female gender [89,93–97], although it may not be a predictive factor [98,99]. Women are less represented in late-onset MS [97] in which the sex ratio is 1.73 :1 [100]. Perimenopausal onset of MS in women is associated with PPMS [95].
Symptoms at onset & during the course of the disease
In PPMS there is no difference between the sexes in terms of onset symptoms, except for a trend for men to present more often with cerebellar or brainstem symptoms [85]. In RRMS, onset symptoms are more frequently sensory for women, and cerebellar or brainstem for men [85]. Optic neuritis and motor symptoms at onset have been shown to have the same frequency among men and women [85]. In concordant parent–child pairs with MS, offspring with affected fathers tended to present more often with cerebellar and cognitive symptoms in comparison with those with affected mothers [79].
Some studies report that pain is more commonly experienced by women, or is more severe [101–103], while others found no difference [104–106]. One study demonstrated greater pain intensity among women [101]. Pain types can differ between men and women. Among patients reporting trigeminal neuralgia and pain related to spasticity, 72 and 33% were women [102]. By contrast, women and men experience disabling fatigue with the same frequency [107–109].
Cognitive decline is greater among men with MS [77,110,111]. The performance of men in verbal and nonverbal delayed memory, visuospatial construction and executive function tests, was worse even after adjustments were made for sex differences among normal controls [110]. Among men, risk factors for severe cognitive decline included older age, longer disease duration, higher EDSS score, lower education level and APO-∊4 allele. None of these have been associated with cognitive impairment for women [111]. However, not all studies have found cognitive impairment differences between sexes [112,113]. Cognitive fatigue is similar for both genders [114].
Imaging
Normal brain
Several differences in brain morphology between women and men have been documented among healthy adults [115]. The main differences are shown in
Gender differences in brain volumes in patients with multiple sclerosis.
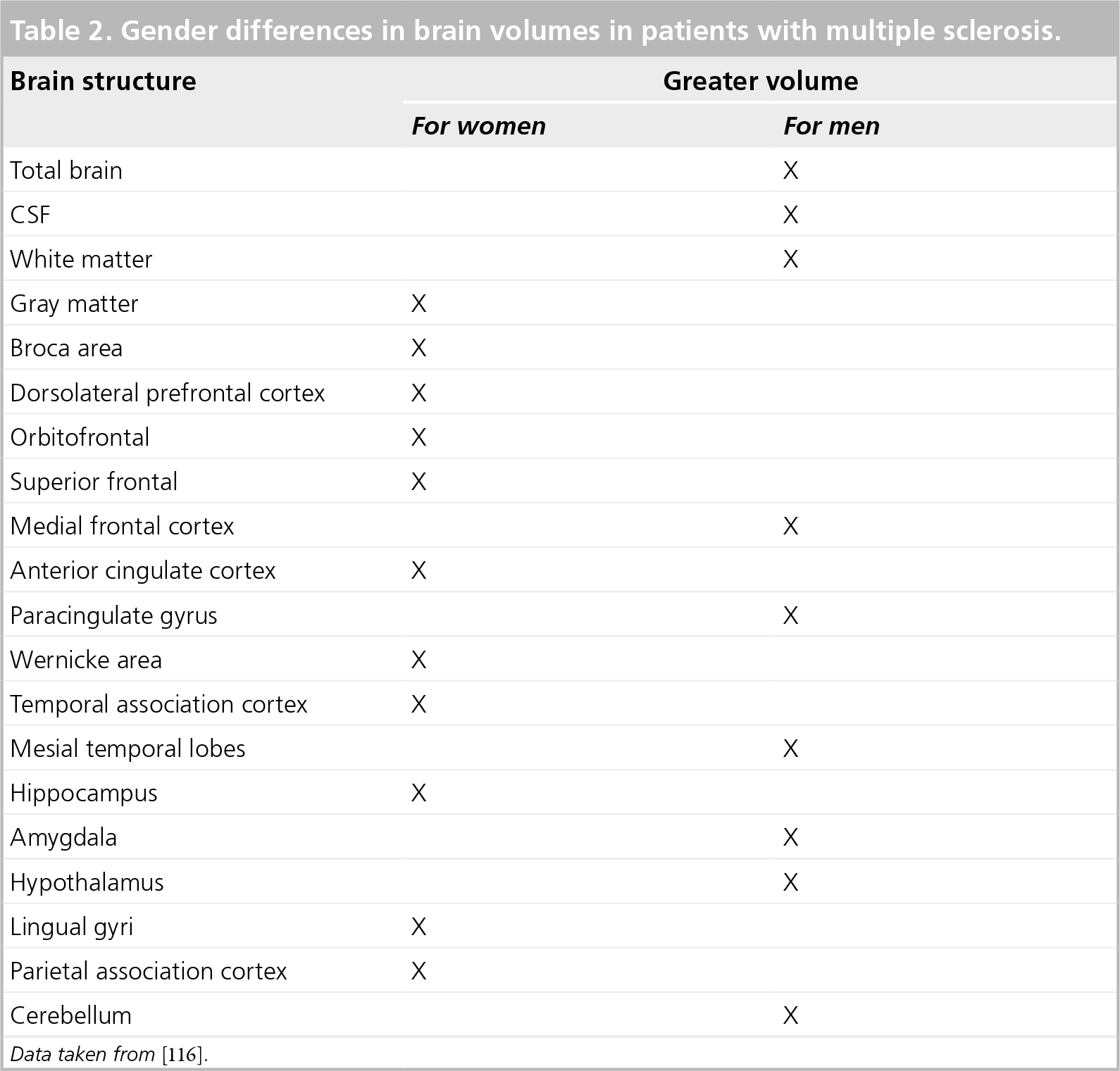
Data taken from [116].
Witte et al. observed a positive correlation between 17β-estradiol and the gray matter (GM) volume in the left superior parietal gyrus for both sexes [115]. They also demonstrated a strong inverse correlation for men, and a trend for women, between progesterone and the GM volume in right middle temporal pole. The correlation was not convincing between testosterone levels and sectorial GM volumes.
MS
Several MRI studies demonstrate that men with RRMS or SPMS have a significantly lower number of enhancing lesions [116–118], but have a higher number of lesions evolving into ‘black holes’, which makes them more prone to less inflammatory but more destructive lesions than women [116]. Women seem to have more frequent disruption of the blood–brain barrier, consistent with a more inflammatory profile. This is consistent with a hormonal influence, since high estrogen/progesterone levels in women are associated with more gadolinium-enhancing lesions [119]. However, two studies failed to show more enhancing lesions among women with MS [120,121]. Li et al. observed a slightly greater T2 burden for men [122]. Two studies found no correlation between gender and either T1 and T2 lesion volumes, or T1:T2 lesion ratio [121,123].
Two studies found no influence of gender on atrophy [124,125]. A study of 763 MS patients showed lower normalized peripheral and total GM volumes for men, and a lower normalized GM volume for women. Men appeared to have more cerebral atrophy [121]. The same authors reported that the magnetization transfer ratio and measures of diffusivity were similar for men and women [121]. Cortical lesions, as evaluated by double inversion recovery, were more frequently reported in men than in women (79 and 51%, respectively), both in the early and in the late stages of the disease [126]. The overall effect of sex hormones on MRI activity remains to be established in larger studies.
MRI & sex hormones in MS
Magnetic resonance imaging activity is linked to different sex hormones (testosterone, estradiol and progesterone) as exemplified by variations throughout the menstrual cycle [127] and pregnancy [128]. We refer readers to the original article from Coyle [1] for details. The overall influence is towards greater MRI activity when estradiol levels are high [119,127,129] and, progesterone [119,127] and testosterone [129] levels are low.
Comorbidities
Autoimmune diseases
Most autoimmune diseases show women preponderance [78,130]. Co-occurrence of MS and other autoimmune diseases has been widely reported [131–138]. These associations have recently been challenged. Ramagopalan et al. conducted a study on 5031 MS patients, 30,259 first-degree relatives and 2707 spousal controls, and concluded that there was only a correlation between MS and autoimmune thyroid disease and pernicious anemia (they looked at ten different autoimmune diseases) with no gender effect [135].
Only a few gender-specific considerations have been reported between MS and other autoimmune diseases, but they are not uniformly supported. The association of autoimmune thyroiditis and MS is stronger for women [136]. This may also apply to MS patients taking immunomodulatory drugs [139], but some evidence against this exists [140]. Somers et al. observed an inverse relation between MS and rheumatoid arthritis, which is stronger for men [136]. There is conflicting evidence on the gender predisposition to develop MS in Type 1 diabetes. One study reported a greater risk for men (relative risk [RR]: 4.36) than for women (RR: 2.69) [137]; another observed that nearly all the patients with both diseases were women [131]. Uveitis usually occurs in women aged 20–50 years old [141] and has been associated with MS. In a large retrospective study of patients with uveitis, 1.3% had MS, 88% of which were women [142]. In another study, 83% of patients with uveitis and MS were women [143].
Sleep disorders: restless legs syndrome
Sleep disorders in MS have been reviewed previously [144]. Numerous studies find restless leg syndrome more frequent in MS, affecting women more than men [144–147]. Other studies did not observe this gender difference [148–151]. Restless legs syndrome is related to iron deficiency, which is more common in women during their reproductive years.
Psychiatric comorbidities
Most studies report that the risk of depression is greater for women [109,152–155] with MS (OR: 1.85; 95% CI: 1.16–2.93 for women compared with men) [109]. However, some studies did not find this gender influence [156–160]. Women are more likely to use antidepressant drugs [161,162]. The predominance of women with MS suffering from depression is an important issue, since depression is the main determinant for quality-of-life (QoL) perception in MS [163].
There is also an association between MS and bipolar affective disorder, which can be 13-times more frequent among MS patients than in the general population. The sex ratio for bipolar affective disorder within a MS cohort was 1.17:1 [159].
Women with MS are at an increased risk of anxiety disorders (mainly generalized anxiety disorder, obsessive compulsive disorder and panic disorder) [164].
The rate of suicide is reported to be increased as much as sevenfold in MS patients [165,166] in comparison to the general population, without gender predominance [167–171]. The risk factors and characteristics of suicide in MS can differ according to gender. Men tend to commit suicide in the fifth decade of life, generally show moderate disability, and have often experienced a recent deterioration. Mental disorders and previous suicidal attempts are more frequent among men [168,172], and they more commonly use violent suicidal methods [172]. The characteristics of women who commit suicide are less distinct [172]. More often, women with MS tend to commit suicide in the first year of onset [168]. A previous study showed that MS onset before the age of 30 years is associated with greater risk of suicide for men [170].
Cancer
Most studies with large numbers of patients conclude that the risk of cancer is decreased in MS patients [173–176]. Two studies [177,178] reported an excess of breast cancers, which could be biased in part by the low parity of women with MS. Nielsen et al. observed that the increase of breast cancers in MS does not change according to age at first pregnancy [173]. The risk of cancer is still decreased for MS patients under immunomodulatory treatment, but breast cancers tended to be more frequent for glatiramer acetate users, although this frequency is not significant [174,175]. Lebrun et al. observed a threefold higher risk of cancer for patients treated with immunosuppressant drugs [174]. Bahmanyar et al. observed an increase in the number of small intestine cancers among men, and of urinary organs and nonmelanoma skin cancers among women with MS [176]. One study reported a significant excess of nasopharyngeal carcinomas and brain tumors among women with MS [178]. This increased frequency of tumors could be related to the frequent MRIs performed in MS patients.
Response to treatments (disease modifying)
Gender differences in the effectiveness of disease-modifying therapies (DMTs) in RRMS are either not observed, or not explored in large trials [179]. In a postmarketing study of 2570 RRMS patients, men were at greater risk of disability progression than women at 1 year [180] and at 7 years. Men had a lesser risk of a second relapse [181].
The effectiveness of natalizumab in AFFIRM and SENTINEL trials was analyzed in prespecified subgroups. The response in terms of progressive disability was significantly favorable for women, with only a favorable trend for men. The effect on relapse rate was similar for men and women [182].
One post hoc analysis of PPMS patients on glatiramer acetate (GA) suggested that men had less disability progression when treated, compared with the placebo. This effect was not observed for women [179]. Moreover, radiological outcomes were not dependent on gender in PPMS under GA treatment, nor was the response of women and men to GA in RRMS [179].
A trial of IFNβ-1a in SPMS failed to demonstrate a change over disability progression, but the response was better in women. The relapse rate did not depend upon gender, but the imaging results were slightly more favorable for women [183].
Childhood MS
Less than 1% of MS patients experience onset of symptoms prior to puberty [1,77,184], and only 2–5% before the age of 16 years [1,77,184–189]. Most pediatric MS cohorts describe female predominance, with sex ratios between 1.3 and 3.0 [186]. This ratio is also a function of age, with girls being proportionally more affected by MS after puberty [185,187,190], with a sex ratio of 1:1 before the age of 12, and of 2:1 thereafter [191]. Another study reported a sex ratio of 1:1 at 10 years, 2.2:1 at 15 years and 2.8:1 at 20 years [192].
Clinically isolated syndrome presenting before the age of 16 is usually a monofocal event with a female predominance. Multifocal events are not influenced by gender [184,191,193]. Onset symptoms vary according to gender, with more girls presenting with sensory disturbances or brainstem dysfunction, and more boys with motor or gait disorders [193]. The risk of developing MS for children who experienced optic neuritis is not different according to gender [194,195]; neither is the risk of a second demyelinating attack after acute disseminated encephalomyelitis [191,196].
In pediatric MS, most studies reveal no gender influence on prognosis [186,193]. One study found that the female gender was related to a higher rate of severity (68% with at least three attacks, or an EDSS ≥4.0) [197]. Duquette et al. found somewhat better outcomes for girls than boys when MS progression started before the age of 16 years, with a more complete recovery from the initial episode, a remitting course and lower disability scores [185].
Prognosis
Prognosis in MS depends upon several factors including gender, age, initial symptoms and course, degree of recovery from the first relapse, time from onset to the second neurological episode, number of relapses in the first 5 years of the disease, and time from onset to EDSS score of four [80,81,89].
In most studies assessing the prognosis in MS, the progression of EDSS score is worse for men than for women when including all disease courses [1,31,77,81,87,89,95,165,198–201]. In concordant parent–child pairs with MS, the highest mean EDSS score was observed in male offspring of affected fathers [79]. The onset of MS by cerebral or urinary symptoms in women was associated with greater progression of disability, while onset with sensory symptoms was related to a better prognosis [202].
Primary progressive multiple sclerosis carries a poorer prognosis [80,81]. Moreover, some studies showed that men among PPMS patients had a worse prognosis than women [81,179,203] but the majority of studies found no difference [85,204–207].
After optic neuritis, the risk of developing MS after 10 years in adults is related to the MRI findings, with a 22% risk if the MRI is normal, and a 56% risk if one or more lesions are present. In the normal MRI group, male gender is associated with a three-times lower risk of conversion to MS (hazard ratio: 0.35; 95% CI: 0.12–0.98) [208]. When MRI was not taken into account, MS developed in 74% of women and 34% of men 15 years after optic neuritis [209]. Some studies reported that women have an increased risk of developing MS [192,208,210–213] although not always significantly [214,215].
In a cohort followed for 20 years after the initial episode, MS developed in 67 out of 107 patients (63%). MS developed in 35 out of 54 patients (65%) who initially presented with optic neuritis, 15 out of 25 (60%) with a brainstem syndrome, and 17 out of 28 (61%) with a spinal cord syndrome [216]. Data was not analyzed by gender.
Survival is mildly decreased in MS. In some studies male gender is a risk factor for earlier death [20,217–220] while other studies show equal survival for both genders [169,202,221–224]. One study revealed higher relative mortality among women with MS in comparison to the general population [225]. Temporal trends in mortality support a decrease in the rates, possibly better for men than for women [220]. Symptoms at onset can interact with the survival differently according to gender. One study showed that men with sensory symptoms at onset had a greater survival, while optic neuritis onset in women showed a tendency towards greater life expectancy [220].
Women issues
Puberty/menarche
A recent study indicates that age at puberty plays a role in the likelihood of developing MS in women but not in men [226], but the extent to which the average age of puberty differed between women developing MS and controls was minute (12.4 vs 12.6 years). According to that study, the relative risk of MS decreases by 0.9 per year with increased age at puberty.
Previous studies reported conflicting results when examining the influence of age at menarche on the likelihood of developing MS. One small study showed that the risk of developing MS was not associated with menarcheal age [227], while a second showed a lower menarcheal age for MS cases than for controls [228]. A more recent Canadian study found an association between age at onset of MS and age at menarche, with age at first symptoms increasing by 1.16 years for each year increase at menarche [229].
Menstrual cycle
Coyle has already reviewed the influences of the menstrual cycle on the symptoms in MS [1]. Relapses can be associated with the premenstrual phase of the cycle [230]. Zorgdrager and De Keyser reported that 42% of premenopausal women had relapses in the premenstrual phase, and, within this group, 45% of the relapses occurred during that phase [231].
Pregnancy
Impact of pregnancy on MS
Pregnancy can cause exacerbation of some autoimmune diseases, and both autoimmune diseases and immunosuppressive drugs can threaten the baby's health [70]. Therefore, pregnancy had historically been regarded as hazardous for women with MS. This is now recognized as incorrect. The pregnancy and multiple sclerosis (PRIMS) study, and many others from different countries, have convincingly demonstrated that MS relapses are significantly less frequent during pregnancy, especially during the second and third trimesters, when compared with the prepartum relapse rate [70,232–237].
A surge of relapses paralleled by increased MRI activity is observed in the first trimester following delivery, but the relapse rate falls back to the prepartum rate by the end of the first postpartum year [70,128,232–235,237–239]. Moreover, only 30% of patients will experience relapses during the first trimester postpartum; most relapses observed are mild and may not require treatment [duquette P, Unpublished Data] [233,240].
At a biological level, variable results in studies are probably due to small study numbers and different methods used to measure cytokine production and identify immune cell subsets. Some studies report that pregnancy in MS is associated with lower IFN-γ production by peripheral blood lymphocytes during pregnancy, which results in an increased Th2:Th1 ratio during pregnancy as compared with the postpartum period [237,241–243]. One study has reported stable levels of IFN-γ throughout pregnancy and in the postpartum period in MS women showing no disease activity, and increased levels during the third trimester and the postpartum period in women with MS experiencing disease activity clinically or on MRI [238]. Another study with minimal variations in IFN-γ levels has reported contradictory results [244]. IL-17 production has been reported as stable [245] or decreased [246] during pregnancy in healthy women. According to one study, IL-17 was decreased during the first and second trimesters in all MS pregnancies studied, but higher levels were observed during the third trimester and the postpartum period in women experiencing a relapse or MRI activity [238]. An increase in the Treg compartment with suppressive activity was reported in healthy pregnancy [246,247] and in MS pregnancy [248]. According to recent studies, Treg expansion is seen only in the first and second trimesters of MS pregnancy compared with prepregnancy levels, and no difference is observed between levels in late MS pregnancy compared with postpartum levels [237,238]. Pregnancy in MS is associated with an increased percentage of CD56 bright regulatory natural killer cells [237].
Late pregnancy is associated with a rise in serum leptin levels in MS but not healthy pregnancy, followed by a greater decrease after delivery in MS patients compared with healthy controls. The relative decrease in serum leptin levels after delivery could correlate with pospartum relapses [249]. Higher prolactin levels in pregnancy could be associated with an increased proliferation of oligodendrocyte precursor cells, and increased remyelination [54].
At a transcriptional level, gene expression for several inflammation-related transcripts has been reported to revert to healthy control levels during early pregnancy in MS patients, and a delay to do so could correlate with relapses during pregnancy [250].
The prevention of relapses following delivery has been a matter of debate, since no clinical data can predict accurately which women are at an increased risk [240]. Even if PRIMS reported that higher prepregnancy attack rate, greater disability, or relapse during pregnancy indicated increased risk, these criteria would identify only a small subset of women with a 50% relapse risk, and would fail to predict 85% of all relapses occurring during the first postpartum trimester. Biological markers possibly predictive of a higher susceptibility to postpartum relapses are under study; for example, the level of IL-8 during first trimester [251], or the levels of IFN-γ, IL-17, Tbet, pSTAT1, pSTAT3 [238] and serum leptin [249] in late pregnancy and postpartum. The ongoing Prevention of Post Partum Relapses With Progestin and Estradiol in Multiple Sclerosis (POPART'MUS) trial will address the potential of hormone therapy (high-dose progestin in combination with endometrial protective doses of estradiol) following delivery to prevent the postpartum surge of relapses [252]. A beneficial effect of intravenous immunoglobulin (IVIg) administration on postpartum relapses was observed in a nonrandomized study, especially when started before delivery [253]. Another study reported no significant reduction in postpartum relapses with higher versus lower IVIg doses given after delivery, especially among breastfeeding women [254]. Thus, further studies are needed, since IVIg administration comes with potential side-effects and a significant socioeconomic burden. The ideal timing for reinstatement of DMTs following pregnancy is still unknown, especially for women wishing to breastfeed. Indeed, current DMTs are not considered safe during breastfeeding, however, recent studies suggest that exclusive breastfeeding for at least 2 months is associated with a significant decrease in postpartum relapses [236,255,256], although other studies have reported no significant effect of breastfeeding on MS activity postpartum [233,240,257,258].
Since no randomized controlled trial can be performed regarding pregnancy, evaluation of the long-term effect of pregnancy on MS course is a challenge. The reasons for avoiding pregnancy can be related to disease severity for some women. However, observational studies have shown no effect, or a trend toward a beneficial effect of pregnancies on time to reach an EDSS score of 6.0 or more, or to convert to a secondary progressive course [233,240,259–262].
Effect of MS on pregnancy & delivery
Spontaneous abortion could be more frequent in women exposed to IFN-β although the number of pregnancies studied is small [263–265]. No increased risk for premature delivery was reported in a Norwegian and a US study [266,267], although, a Taiwanese study reported a 2.25-fold increase in premature delivery among MS women [268]. Premature delivery has not been associated with exposure to DMTs [263–265].
Women with MS present a marginal increase in the risk for prenatal hospitalization, labor induction, slow progression of labor, need of instrumental assistance at delivery and cesarean-section delivery, but are otherwise no more likely to experience other pregnancy complications such as preeclampsia, postpartum hemorrhage or premature rupture of membranes [53,266]. There has been reluctance from the medical community to offer epidural analgesia to women with MS at time of delivery. This attitude is not supported by scientific data. Epidural analgesia is safe in MS patients and it does not induce MS relapses [dahan B, Unpublished Data] [233,240].
Effect of MS on the baby
A slight increase in intrauterine growth restriction and lower birth weight with normal head circumference has been observed in children of women with MS, probably more frequently when exposed to interferon in utero [53,234,264–266,268,269]. Birth defects do not seem to be more frequent following pregnancy in MS [233,266,267]. Even among fetuses exposed to immunomodulatory agents, no significant increase in birth defects is reported by most studies [232,263–265,270], although numbers are small. A retrospective study reported an increased malformation rate among newborns exposed in utero to immunomodulatory agents [271]. Exposure to interferon in utero does not seem to alter early development of children [269]. Ideally, immunomodulatory agents should be stopped before pregnancy since safety has not been clearly demonstrated. A non-negligible proportion of pregnancies in women with MS are, however, unplanned.
Menopause
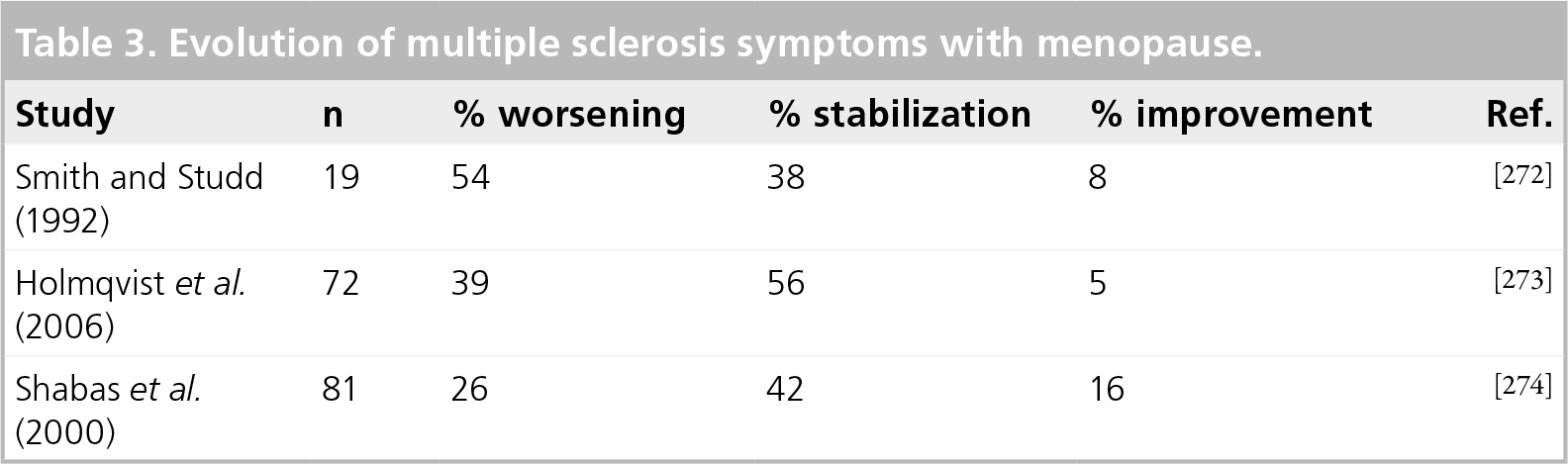
The risk of developing RRMS symptoms declines with and beyond menopause [1]. PPMS often begins around menopause, and the transition from RRMS to SPMS is also associated with this period of life [1].
Three studies investigated changes in MS symptoms in association with the menopause, but these reports are based on a total of 172 patients
Evolution of multiple sclerosis symptoms with menopause.
Oral contraceptives & hormone replacement therapies
A large prospective study from two cohorts in the USA, the Nurse's Health Study (NHS; 1976–1994) and the Nurse's Health Study II (NHSII; 1989–1995) did not support a lasting protective effect of oral contraceptives (OCs) on MS incidence, in accordance with previous studies issued from smaller British cohorts. A recent case–control study performed on the large British General Practice Research Database, analyzed MS incidence in women with at least 3 years of continuous information before the date of first symptoms. The incidence of MS was found to be 40% lower in recent users of OCs compared with nonusers. Another study suggested that OC use is associated with a decreased severity of MS symptoms. Taken together, these observations suggest that OCs may be beneficial for MS patients [275].
Psychosocial issues
Social support
In MS, as for other chronic diseases, there is an increased need for social support to overcome the difficulties accompanying the physical and social consequences of the disease. Gender and marital status may influence social support. Wineman et al. found that women had greater networks than men [276]. Two studies observed similar social support for both genders [277,278]. Gulick et al. reported that men perceived greater social support, in terms of affect, affirmation and aid support, than women [279]. The authors also noticed that men without spouses (compared with those with spouses) felt a higher loss of support. Women report more available resources, perceived social support and perceived availability of friends than male caregivers [280].
Moving to a nursing home usually occurs when social support fails to meet the needs of chronically ill patient. Buchanan et al. observed that men in nursing homes were more likely to be totally dependant in activities of daily living and have greater motor impairment, while women tended to have better communication skills and cognitive performance [162]. Women more commonly experienced pain and were more frequently depressed or anxious than men [162]. The decreased functional status of men in nursing homes may underlie their greater social support, which allows them to live in the community with a greater disability level.
Coping
Patients cope differently with MS according to their gender. Women tend to cope better than men [281]. Strategies to cope with MS are similar for both genders, but, compared with women men use more planning strategies, which are problem-focused plans than women [282]. There are gender differences in the ability to cope with a parent affected by MS within families. Daughters tend to cope better than sons, independently of the gender of the affected parent. A younger age for daughters at MS onset is associated with better coping. Healthy mothers and daughters tend to cope better than fathers and sons with the increasing disability of the father [281].
Conjugal life
Literature on gender differences in conjugal life in MS is limited. There is no consensus on whether divorce in MS is more frequent among men or women. Three studies described similar marital and relationship habits among both genders [278,283,284]. Glantz et al. followed a cohort of 108 MS patients married at the time of diagnosis, for 5 years: the woman was the affected partner in 96% of the 23 divorces observed [285].
Harrison et al. investigated the different benefits that women and men with MS could get from marriage [286]. They observed that for men being married was associated with a better acceptance of disability and less perceived impairment.
According to McCabe et al., relationship satisfaction was similar for men and women with MS and correlated with sexual activity and sexual satisfaction for both, although this association was stronger for women than for men [283,287]. The same author observed that cognitive functioning, quality of sleep and rest predicted the relationship quality for women [283].
Sexuality & sexual dysfunction
Sexual dysfunction is a prevalent and major symptom in MS that severely affects QoL. Its evaluation requires insight into the primary changes that directly affect libido (i.e., sexual response and orgasm due to direct damage to the nervous system); the secondary changes (i.e., complaints that are related to the physical disability of MS, such as fatigue, muscle rigidity, weakness and spasms); and the tertiary changes (emotional, social and cultural) aspects of MS. The components of MS-associated sexual dysfunction are reviewed in [288].
Impact of MS on the caregiver
Certain characteristics of MS burden differentially affect satisfaction with life, based on the gender of the caregiver. Increasing severity of disability, and duration of caregiving have a stronger adverse effect on women. Surprisingly, the authors found a positive correlation between duration of illness and satisfaction with life for male caregivers, suggesting that men's well-being adjusts over time, while women may be more likely to experience negative cumulative effects [289]. Greater social support has a more positive influence on satisfaction with life for women than for men [289]. Patti et al. found that female sex was a predictive factor for poor QoL among caregivers [290]. Male and female caregivers have different socioeconomic stature; since men receive a higher income than women [289].
Employment
There is conflicting data regarding the influence of gender on employment for MS patients. Some studies have reported that gender has no effect [291,292], while others found that men are more likely to be employed [284,293–295]. Hakim et al. reported that most patients who change their employment status from full-time to part-time are women [296]. This could be explained by the more frequent progressive course for men, which does not allow such a change. However, another study failed to report this difference [291].
Rumrill et al. assessed discrimination at work towards men and women with MS [295]. They found both genders were victims of discrimination related to discharge and reasonable accommodations, but women were more frequently reported harassment and men alleged more hiring and reinstatement discrimination.
Financial problems
In a study from Hakim et al. financial problems related to MS were reported by 46% of men, compared with 26% of women [296].
Health maintenance
The prior review by Coyle indicated that health maintenance was often neglected in MS patients, and proposed a preventive healthcare plan [1].
Healthcare costs
An American study found that cost for healthcare utilization in MS was affected by gender. Men with MS had higher annual medical charges in comparison with healthy men, but this was not the case for women, who already have higher healthcare costs when healthy [297]. This is the only study that analyzed the gender effect specifically. In other studies, healthcare cost increased with disease progression and with use of disease-modifying drugs, without gender influence [298].
Self-assessment of health & QoL
A recent abstract reviewed self-rated health status in MS patients by means of the SF-36 questionnaire (eight studies), and acknowledged similar results for men and women [299]; this is concordant with others studies [300–306]. A few studies report that women [298,307–309] or men [310–313] have a better QoL. Casetta et al. observed a marked reduction in QoL as the EDSS increases for men, while the correlation was less striking for women, especially after an EDSS of 5 [309].
End of life
Multiple sclerosis rarely culminates in early death. Occasionally, the patient ends up in a chronic care institution in a vegetative state, sometimes for years, with no hope of recovering any kind of autonomy. To avoid these situations, it is advisable to have open discussions, in appropriate circumstances, about the degree of intervention wished by the individual, should severe, irreversible worsening occur. Most patients are willing to consider autopsy for scientific purposes.
Assisted suicide is legalized in some European countries (e.g., The Netherlands, Switzerland and Belgium). A Swiss group has reported on 421 assisted suicides over a 3-year period. They report an increased proportion of younger patients and of women. They offer no other explanation, than to say that women are more expressive of their feelings than men [314].
Conclusion
Research in neurobiology, immunology and endocrinology is converging. Many of the key molecules in one system are known to play important roles in the other systems. Molecules can assume different roles according to the milieu. As we better understand the cross-talk between these systems, we will be in a better position to unravel the etiopathogenesis of many common diseases, such as MS.
We have updated a previous review of gender issues in MS. In addition to the increasing susceptibility of women to MS, the complexities of the interaction between the nervous, genetic and immune systems are increasingly understood. These advances will contribute to more rational treatments of the disease. Sex hormones might have a role in neuroprotective and restorative therapies. Although deficiencies in vitamin D are well documented, it is not yet known whether their correction would be beneficial. A preventive trial with vitamin D in at-risk populations would be worthwhile, but results would be accrued only after long time periods. With the current state of knowledge, it is impossible to predict whether someone will or will not have MS. Gene therapy, given the number of genes involved and their small contribution, is unlikely to ever be possible. Pregnancies can now be envisaged with a realistic optimism. Withholding DMTs is counterbalanced by the decrease in disease activity during pregnancy. Postpartum relapses are generally mild; breastfeeding may have a protective effect in this regard. The uncovering of the mechanisms underpinning the frequent cognitive problems will help in keeping patients personally and socially active. Understanding the impacts of a chronic illness such as MS will help patients and their families in coping with its often devastating effects. The increased attention MS has received in the last 3 decades will help in attaining a long awaited cure.
Future perspective
Advances in immunology, genetics, neurobiology and their interconnections with the endocrine system, coupled with the refinement of epidemiological methods, should lead to explanations for the tremendous increase in MS susceptibility among women. Meanwhile, a better understanding of the different impacts of MS on women and men will help in tailoring treatments; in this regard, female and male hormones may become part of the treatment strategies. Pregnancy will become better integrated in the life course of women with MS, as the impact of breastfeeding is better defined. A prospective pregnancy register for MS, currently in the planning stages, could generate needed data on the influence of treatments of MS on the course and outcome of pregnancies.
Executive summary
The incidence and prevalence of multiple sclerosis (MS) has increased over the last decades, with a disproportionate increase in women, especially in countries with a high basic prevalence in MS. Unraveling the mechanisms underlying this conspicuous finding will help in finding the cause(s) of MS.
Sex hormones have an increasingly recognized role in the development of the CNS and immune system. The importance of cross-talk between the hormonal, nervous and immune systems is being addressed.
Estrogens and testosterone have protective effects on the nervous tissue. They are currently undergoing testing in therapeutic trials in MS patients.
Leptin, a hormone produced by adipocytes, has an anti-inflammatory effect on the immune response; it could have a therapeutic potential.
Several MS susceptibility genes have been identified, the most important ones being part of the MHC; others are involved in the immune response. All have a small effect on susceptibility, but could be important in uncovering new therapeutic avenues.
Vitamin D could explain the latitudinal gradient observed in the prevalence of MS. Vitamin D supplementation may possibly have a protective effect on MS susceptibility and course.
There are some differences between women and men in disease course, prognosis, MRI and response to treatment.
Pregnancy is now encouraged in women with MS, when circumstances are favorable. The frequency of relapses decreases in the last two trimesters of pregnancy, with a brief surge of relapses during the postpartum first trimester.
Some data indicate that breastfeeding has a protective effect on MS course. This could be related to a beneficial effect of prolactin on myelin repair.
Depression is frequent in MS, especially among women. Patients and caregivers need help in dealing with emotional problems. End of life issues must be addressed adequately to avoid undue stress.
Footnotes
Pierre Duquette has served on advisory boards, given lectures, run clinical trials, received research support and financial support to attend meetings from the following companies: Bayer-Schering, Biogen-Idec, EMD Serono, Novartis, TEVA Neuroscience. Pierre Duquette is funded by the following peer-reviewed agencies: Canadian Institutes for Health Research, Multiple Sclerosis Society of Canada. Patricia K Coyle has received honoraria for teaching and educational activities from Acorda, Bayer, Biogen-Idec, EMD Serono, Novartis, Pfizer, Sanofi Aventis and Teva Neurosciences, and current funding from Novartis and Sanof Aventis. Céline Jobin has received honoraria for educational activities from Teva, Biogen-Idec and EMD Serono. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.