
Abstract
Labor pain is a foremost concern for every pregnant woman since failure to relieve it might have a great impact on birth outcomes. Unrelieved labor pain affects a mother's clinical characteristics including her cardiac output, blood pressure, respiratory rate, oxygen consumption and catecholamine levels, all of which could be harmful for both the mother and infant. Labor pain could result in the loss of emotional control leading to mood disorders [1]. Labor pain is also accompanied by fear, which is related to a slower progress of labor, leading to increased rates of cesarean section [2,3]. It has been reported that 60% of primiparous and 40% of multiparous women had experienced extremely severe labor pains in the acute phase [4], and up to 40% of laboring women were not satisfied with pain relief after receiving analgesic drugs [5].
The intensity of labor pain and the individual responses of childbearing women to pain are widely varied. In the USA, 63% of women who delivered received an epidural analgesia that could be, in part, due to maternal attitudes before labor and a personal preference to escape from vaginal delivery pain [6].
It is necessary that women understand the advantages and disadvantages of different pain relief methods and make informed decisions. Nowadays, medical pain relief is the foremost accepted and used method of pain relief and will not be replaced by nonpharmacological methods. A majority of analgesic drugs for labor pain relief have serious side effects for mothers, including decreased cardiac output, bladder distention and a prolonged second phase of labor [7]. Alternatively, palliative drugless or behavioral procedures such as acupuncture, respiratory techniques and acupressure, as well as music, touch, massage and aqua therapies, are recommended.
Massage therapy affects surface skin, soft tissues, muscles, tendons, ligaments and fascia by manual systematic techniques. Using an endorphin-release mechanism, controlling nerve gates and stimulating sympathetic nerves, massage therapy could lead to muscular relaxation. The advantages of massage therapy for childbearing women, either physically (physical manipulation of soft body tissues) or psychologically (positive healing energy that is exuded during this manipulation), are extensive and have been well documented in Persian, Egyptian and Roman civilizations [8–11].
Music therapy, through sense distraction and reduction of the patient's concentration of stimuli, can decrease the anxiety and pain sensation. Relaxation is one of the psychological effects of music therapy that can decrease heart rate, respiratory rate and metabolism [12,13].
The present study aimed to compare the effects of massage and music therapies on the severity of labor pain.
Materials & methods
The present randomized clinical trial was conducted in 2007. Overall, 101 pregnant women who were hospitalized for delivery at the Mustafa Hospital in the Ilam Province of western Iran were randomly recruited. Randomization was completed using a computerized minimization program to assign participant women to either the massage (n = 51) or music (n = 50) group. Participants were primiparous singletons aged between 20 and 30 years with a cervix dilation of less than 4 cm, were at 37–42 weeks of gestation and were pregnant with babies of cephalic presentation and normal birthweight. Mothers who had received analgesic or antipsychotic medications or were labor-induced, and those with spontaneous rupture of the membrane for longer than 20 h, were excluded from the study. Mothers with hearing and visual difficulties, infectious diseases, inflammation and dermal sensitivities in the massage fields were also excluded. Overall, three samples were withdrawn from the study owing to either cervix dilation of more than 4 cm or rapid progress of labor.
Data were collected using a self-report questionnaire and the Visual Analog Scale (VAS) for pain intensity evaluation, which contained six different colored parts. Each participant chose one color based on her feeling of pain intensity before and after each intervention. The validity and reliability of the VAS has been evaluated with test–retest methods, examining properties of the method itself including the length and position of the line, the availability of previous ratings to participants and the psychomotor and visual ability of subjects [14–16]. A correlation coefficient of 0.89 has already been reported in a comparison between the VAS instrument and Faces Pain Scale [17,18]. The original VAS in the present study was slightly simplified since a majority of women in this area were illiterate and could not read the numbers properly, based on the experiences of the researchers (Figure 1).

Visual Analog Scale for pain intensity evaluation.
The sampling process was completed by trained midwives during either day or night shifts. Subjects were randomly stratified into either massage or music therapy groups. All subjects were matched for age, duration of the latent phase, weight, height and gestational age. Sample size was calculated using the StatCalc program under Epi-Infotrade; 2002 statistical software (CDC, GA, USA). Prior to the data collection process, the research goals and objectives were clearly explained to the participants and written consent was obtained to take part into the study.
As soon as the cervix was dilated by up to 3–4 cm, women in the massage therapy group were requested to close their eyes and take rhythmic breaths deeply. During uterus contractions, they were asked to take breaths more deeply and calmly by concentrating on the massage. Massage points were the lower area of the abdomen, shoulders, back and pressed pubic area. All patients in this group received 30 min of massage.
Women in the music therapy group were requested to listen to soft traditional music (one of five optional types) without lyrics using headphones for 30 min, starting early in the active phase of labor.
Following the interventions, a clinical status form was completed for each patient, in order to check her sensed pain intensity based on the VAS, by research colleagues who were not aware of the assignment of participants to two groups. Patients did not ask for or receive any other pain relievers while they were receiving either the massage or music therapy treatments in the present study.
Data were analyzed by nonparametric statistical tests including Manvitny and Wilcoxon. The population attributable risks were also calculated [19,20]. The study was approved by the Local Ethical Committees.
Results
The mean age ± standard deviations were 21.3 ± 2.9 years and 21.5 ± 3.1 years for the massage and music therapy groups, respectively, with no significant difference. None of the participants had an academic degree and the maximum level of education in the two groups was completion of high school (diploma). There was no significant difference between the two groups in terms of educational level. The mean weight ± standard deviations were 63.2 ± 6.3 kg and 65.1 ± 7.4 kg for the massage and music therapy groups, respectively (p > 0.05). The other demographic characteristics such as jobs, duration of latent phase and gestational age were almost identical, with no significant differences between the two groups. Overall, 12 patients in the music therapy group (24%) and five patients in the massage therapy group (10%) expressed a need for some other pain relief methods after the interventions.
There was a significant difference between the two groups in terms of severity of labor pain after (p = 0.011), but not prior to (p = 0.613), the interventions. Mothers in the massage therapy group had the lowest level of pain compared with those in the music therapy group (p = 0.009). The most significant difference between the two groups of massage and music therapies before and after interventions was observed in the agonizing phase (most severe pain), with a main difference of 36.3 (95% CI: 13.6–41.4; p = 0.001) (Table 1). In addition, there was a significant difference between the two groups in terms of pain severity after the interventions (p = 0.01) (Table 2).
Pain intensity before and after interventions.
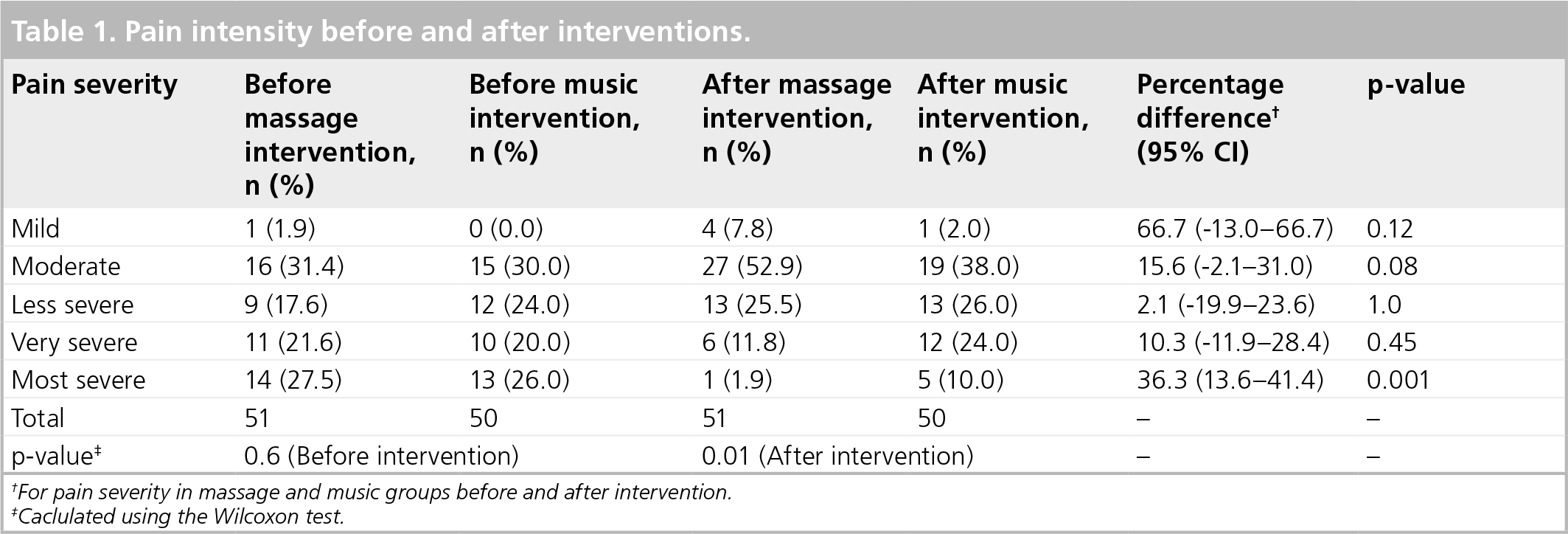
For pain severity in massage and music groups before and after intervention.
Caclulated using the Wilcoxon test.
Pain intensity before and after interventions.

Calculated using the Manvitny test.
IQR: interquartile range.
Discussion & future perspective
The participation rate was 94.5%, which is positively representative. The present study demonstrated a significant difference between the massage and music therapies in terms of labor pain relief after the interventions. Agonizing, or most severe, labor pain was significantly relieved after massage therapy (p = 0.001). These findings are consistent with the results of the latest research in which the effect of massage and muscle relaxation techniques in the latent phase of labor until 1 h after delivery was studied, and it was indicated that the intervention group sensed less pain and experienced more relaxation throughout the whole labor process compared with the control group [8].
The palliative effect of music therapy, which is demonstrated in the present study, is also consistent with the literature [21]. A recent study evaluating the effect of music therapy on decreasing pain sensation and distress in labor indicated that the intervention group sensed less pain than the control group [1]. There is also evidence demonstrating increased pain relief effects by up to threefold with music therapy after cesarean section compared with control groups [22,23].
In agreement with the previous reports, both massage and music therapies in the present study were found to be effective as nonpharmacological techniques. Therefore, these methods can be used as an alternative for pain relief, especially during the initial hours of the active phase in the labor room. However, massage therapy is more effective and improves more relationships and encourages kindness between mothers and healthcare workers, which is important in decreasing the anxiety of laboring women. Extensive physical and psychological advantages of massage therapy for childbearing women have been documented in Persian, Egyptian and Roman civilizations (physical manipulation of soft body tissues and the positive healing energy that is exuded during manipulation) [22,24].
The present study was limited to only looking at the effects of massage and music therapies on the process of labor pain relief independently. Further studies are required to investigate the effects of combined music and massage therapies on labor pain. Measuring fatigue levels in labor and using other pain relievers such as muscle relaxation, warm water bathing and using a low-dose analgesic in combination with massage and music therapies are also recommended. In the present study, patients were recommended to use deep, rhythmic breathing along with massage and this might be a confounding variable, since breathing is also used to decrease pain or distract from pain in labor. The study was also confounded by using five optional music types in which patients were only allowed to choose one of them. Further randomized clinical trials with control groups are recommended in order to generalize the findings in the present study.
In conclusion, massage therapy was an effective method to reduce and relieve labor pain compared with music therapy and can be clinically recommended as an alternative, safe and affordable method of relieving pain in which using either pharmacological or nonpharmacological methods are optional.
Executive summary
Labor pain is a foremost concern for every pregnant woman. Labor pain relief has a great impact on birth outcomes. The intensity of labor pain and the individual responses of pregnant women to pain vary widely. It is necessary that women understand the advantages and disadvantages of different pain relief methods and make informed decisions.
The ideal labor pain relief should be safe for both the mother and baby, easy to administer, predictable and constant in its effects, and reversible if necessary. Labor pain relievers should not interfere with uterine contractions or with mobility.
There are pharmacological and nonpharmacological options for pain relief in labor. Hypnosis, acupuncture, transcoetaneous electric nerve stimulation, hydrotherapy, music and massage therapies are recommended as nonpharmacological methods.
The advantages of massage therapy for childbearing women, either physically (i.e., physical manipulation of soft body tissues) or psychologically (i.e., positive healing energy that is exuded during this manipulation), are extensive and have been well documented in Persian, Egyptian and Roman civilizations.
Music therapy through sense distraction and reduction of patient's concentration on stimuli can decrease anxiety and pain sensation. Relaxation is one of the psychological effects of music therapy that can decrease heart rate, respiratory rate and metabolism.
Massage therapy was an effective method to reduce and relieve labor pain compared with music therapy and can be clinically recommended as an alternative, safe and affordable method of pain relief in cases for which using either pharmacological or nonpharmacological methods are optional.
Footnotes
Acknowledgements
The cooperation of participants in the present study and the assistance of midwives, nurses and healthcare assistants at the Mustafa Hospital (Ilam, Iran) are appreciated. The authors also thank Mr Mostafa Delpisheh who kindly edited the manuscript.
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.