
Abstract
General awareness of cardiovascular disease (CVD) as the leading cause of death for women and knowledge of CVD risk factors have increased in the last 10 years. Whether this greater general awareness and knowledge leads to improved risk assessment on a personal level remains uncertain. Therefore, the purpose of this study was to measure the knowledge of CVD risk factors and determine the level of personal CVD risk-factor awareness among female public employees of North Dakota, ND, USA. A 30-item, pretested, standardized questionnaire was adapted from previous American Heart Association (AHA) nationwide surveys to measure awareness of the AHA's Go Red For Women movement and cardiovascular health. The online survey was completed by 1044 women, with most of the participants (∼90%) reported as being aware that heart disease was the leading cause of death for women in the USA, which is much higher than the national average. Nearly all the participants (97.3%) correctly recognized the Go Red ‘Red Dress’ symbol, and knew that it relates to women and heart disease. The prevalence of individual CVD risk awareness was high for blood pressure (82.2%) and moderately high for cholesterol (67%). Much lower rates of CVD awareness were reported for blood glucose (40.8%) and BMI (29.4%). Along with age and certain socioeconomic factors, awareness of any one CVD risk factor was strongly associated with awareness of other CVD risk factors. It is worth mentioning that the participants with favorable demographics and background characteristics and with a high general awareness may also have low personal awareness of certain CVD risk factors. This low personal awareness lessens one's perceived susceptibility to CVD, which in turn reduces the likelihood of adopting preventive action to decrease personal risk of CVD. Future awareness programs should concentrate on improving individual risk awareness, particularly of blood glucose and BMI, as a means of improving behavior towards better cardiovascular health.
Worldwide, heart disease and stroke kills more women each year than cancer, tuberculosis, HIV/AIDS and malaria combined [1]. While there is a persistent belief that men suffer from cardiovascular disease (CVD) more frequently than women, it is the contrary that is true. Since 1979, CVD mortality records in US show a sharp decrease for men, while rates for women have increased, especially since 2000 [2]. However, the evidence shows that women are more likely than men to be underdiagnosed and undertreated for heart disease [3]. Although approximately one in three US women has at least one form of CVD, close to three in five are aware that CVD is the leading cause of death (LCOD) in the USA [4].
The importance of awareness for preventive action by adopting a healthy lifestyle can be explained through the ‘health belief model’ (HBM) [5]. The basic postulate of the HBM is that for an individual to take preventive action, they must perceive themselves to be both susceptible to an underlying potential health risk, and that this risk is severe enough to threaten their wellbeing. Preventive action can be a health checkup to confirm his/her belief, or a behavior change towards a healthier lifestyle. Evidence from earlier studies demonstrated that awareness of CVD risk factors is associated with carrying out prevention-seeking behaviors [6–8]. The study by Mosca et al. demonstrated that awareness of CVD as the LCOD was enough to direct women to take action towards lowering their own risk of CVD and also to take action for someone in their family [9].
Realizing the importance of awareness of CVD, the Go Red For Women (GRFW) international campaign was launched by the World Heart Federation (WHF), and encouraged member countries to recognize CVD as the LCOD among women by building global attention and fostering positive behavior change [101]. In 2004, the American Heart Association (AHA) initiated its nationwide GRFW campaign, with one of the basic aims being to increase awareness among US women that CVD is not just men's LCOD, but also their own. This is to be accomplished by educating women about their personal CVD risk through the ‘knowing your numbers’ campaign line, and encouraging primary CVD prevention through behavior change related to a healthy diet, physical activity and smoking cessation [102].
In 2004, the AHA adopted the ‘Red Dress’ symbol for its GRFW campaign. The National Heart, Lung and Blood Institute (NHLBI) originally developed the ‘Red Dress’ symbol in 2002 for their The Heart Truth campaign, which was the first federally sponsored national campaign to increase awareness among women about their risk of heart disease. The NHLBI took a traditional social marketing strategy that included audience analysis, formative research, materials testing and production and partnership development before launching the ‘Red Dress’ as the national symbol for women and heart disease awareness.
The AHA periodically conducts nationwide surveys to assess how aware women are of CVD as their LCOD. In 2006, 57% of women were aware that CVD is their LCOD, which is a prominent increase from 1997 when only 30% of women were aware of CVD being their LCOD [4]. This increase in awareness occurred simultaneously with an increase of awareness of the ‘Red Dress’ symbol. In 2005, shortly after the AHA adopted the Red Dress symbol, awareness was only 25%. By 2008, awareness of the Red Dress symbol had more than doubled to 61% [10]. Furthermore, awareness levels appear to be strongly related to socioeconomic factors including ethnic background, education level and health insurance. Women who are Caucasian, have attained a high level of education or income, or have adequate health insurance coverage tend to be more acutely aware of CVD risk [4].
To date, the majority of CVD awareness studies have tried to examine whether or not the presence of knowledge is associated with preventive health behavior. For example, if a women knows that a blood cholesterol level of greater than 200 mg/dl is considered ‘at-risk’, then she is considered to have good general awareness of cholesterol risk. General awareness is important in order to raise understanding of the severity of CVD. However, the basic postulate of the HBM is that an individual who perceives his/her own health to be at risk, or susceptible to risk, should also take preventive action. Therefore, the general awareness of CVD as the LCOD or awareness of the cut-off values of certain CVD risk factors may not be enough to assume that the individual is aware of his/her own risk status. As Mosca et al. noted, simply assessing general knowledge of CVD risk factors may not be enough to create change; instead, it may be important to assess and target those with low levels of personal risk awareness [9]. Therefore, general awareness of CVD risk factors may not necessarily increase the likelihood of taking preventive action without a concomitant increase in perceived personal susceptibility. A recent review article showed that 70% of Americans were aware of their risk of hypertension, yet only 59% were being treated and only 34% had their blood pressure under control [8]. Building on this idea, Go Red has a primary campaign line of ‘know your numbers’. If each woman knows her own CVD risk factors, she can better per-ceive her CVD risk status. A proper perception of CVD susceptibility is more likely to lead women to assess potential benefits from engaging in recommended health behaviors. Figure 1 presents the theoretical framework discussed herein.

Theoretical framework explaining the importance of personal cardiovascular disease risk awareness in fulfilling the basic postulates of the health belief model and to motivate an individual towards a heart-healthy lifestyle.
In the light of the GRFW campaign, it is important to measure whether women ‘know their numbers’ (i.e., to measure the awareness level of personal CVD risk and to examine the effectiveness of the program at leading women to adopt an improved heart-healthy lifestyle). The purpose of this study was to measure the knowledge of CVD risk factors and the level of personal CVD risk-factor awareness in a large sample of female public employees of North Dakota, ND, USA, and to investigate the sociodemographic correlates of awareness of CVD risk factors.
Materials & methods
Participants & design
A statewide online survey measuring the awareness of the AHA's GRFW movement and cardiovascular health among female public employees of ND was conducted in November 2008. The questionnaire for the survey was posted on an online survey webpage. Through a generous partnership with the North Dakota Public Employees Retirement System (NDPERS), e-mails were sent in early November 2008 to approximately 7500 employees through their worksite wellness coordinators. The NDPERS list is updated at least once per year, and no retired persons were included. The statewide employees were predominantly Caucasian, which is representative of the state of ND. Potential participants were asked to complete the health survey, and by doing so gave their consent to use their data for research purposes, in accordance with Institutional Review Board guidelines of North Dakota State University. The survey was available for 2 weeks from the date of the original e-mail, although the vast majority of responses were received during the first 4 days. No follow-up e-mails were sent. A total of 1044 women participated in the survey, approximately 14% of the eligible population.
Measures
A 30-item, pretested, standardized questionnaire (Appendix 1) was adapted from the AHA national survey used to collect data on CVD risk and LCOD awareness. To date, validity studies for the AHA survey have yet to be published. The survey used for this study collected data on demography, general awareness for CVD in women, awareness of the specific CVD risk factors, medication use and personal and family history of CVD. The questions on the demographic information of the participants asked them their age, ethnicity, annual household income, marital status and whether they were living with any child under 18 years of age. The participants were also asked about their medication use for lowering blood pressure, cholesterol or blood glucose. The personal and familial history of heart disease, stroke, high blood pressure, high cholesterol, high blood glucose and obesity were recorded for each participant. The questions on general awareness of CVD in women consisted of questions addressing the LCOD for US women, awareness of the GRFW program and exposure to and recognition of the Red Dress symbol.
The awareness for specific CVD risk factors for each participant was assessed by a set of three similar questions related to each cardiovascular risk factor (i.e., blood pressure, cholesterol, blood glucose and BMI). Each participant was asked whether she had checked her blood pressure and blood glucose in last 12 months, cholesterol in last 5 years and whether or not she knew her BMI. Next, she was asked to report whether she was diagnosed with having the specific CVD risk factor or not in her most recent checkup, and then asked to recall the result of that last checkup in numbers. For example, the set of questions for the blood pressure was, “In the past 12 months, have you had your blood pressure checked?” If the answer of the question was “yes” then the participant answered the following two follow-up questions. The first follow-up question was: “When you had it checked last, were you told the result was: too low/normal/high/too high?” An answer of “high” or “too high” was considered as having the risk factor of hypertension. The participants were then classified as ‘risk factor present’ or ‘risk factor absent’ based on the reported result of the last diagnosis for each CVD trait. In the second follow-up question, the participants were asked to remember and report the number of the last diagnosis. For example, the question for blood pressure was: “When you had it checked last, were: both the numbers below 140/90 mmHg/either of the numbers between 140/90 mmHg and 160/100 mmHg/either of the numbers above 160/100 mmHg?” Responses to this question were matched with the answer of the previous question. If a participant diagnosed with hypertension (or ‘risk factor present’ for blood pressure) answered that the result of the last checkup was “both the numbers below 140/90 mmHg”, then it was considered a case of a lack of personal blood pressure awareness. However, if the participant answered that the result was “either of the numbers between 140/90 mmHg and 160/100 mmHg” or “either of the numbers above 160/100 mmHg” then it was a case of personal blood pressure awareness. Moreover, if the participants diagnosed without hypertension (‘risk factor absent’) answered that the result of the last checkup was below 140/90 mmHg then it was also a case of personal blood pressure awareness. Therefore, any time there was a match between follow-up question 1 and 2, the participant was considered as being aware. If the answers to the questions did not match, then the participants were categorized as being unaware. In addition, participants who did not answer either of the questions regarding the result of the last checkup was considered ‘unaware’ for that particular CVD risk factor.
Participants who answered “no” to any of the initial risk-factor questions (i.e., did you check your blood pressure and glucose in the last 12 months?, cholesterol in the last 5 years?, and; do you know your BMI?) then skipped follow-up questions 1 and 2, and instead were redirected to questions pertaining to the next risk factor. Since these women had not recently checked a given risk factor, it was assumed they had no current personal awareness of the respective risk factor.
Analysis
The background characteristics of the participants, including demography, medication use and familial and personal history of CVD, have been presented in Table 1. The general awareness level for heart disease as the LCOD among US women, and the exposure and recognition rate of the Red Dress symbol of GRFW, are presented for different age groups in Table 2.
Background characteristics of participants (n = 1044).

Awareness of leading cause of death for US women and recognition of the ‘Red Dress’ symbol by age groups.

All values are in %.
The prevalence of each CVD risk factor was calculated based on the result of the last checkup. In this context, it is worth mentioning that the participants who did not check their blood pressure and blood glucose in the last 12 months, cholesterol in the last 5 years or did not know their BMI, were not included in the calculation of prevalence of CVD risk factors (Table 3). As mentioned previously, if a woman has not checked the numbers pertaining to her risk factors recently, then it was assumed that she is unaware of her personal risk. This may present some limitations for interpreting the prevalence of risk awareness related to BMI, since so few women reported knowing their BMI.
Prevalence of different cardiovascular disease risk factors based on recent cardiovascular disease risk-factor checkup.
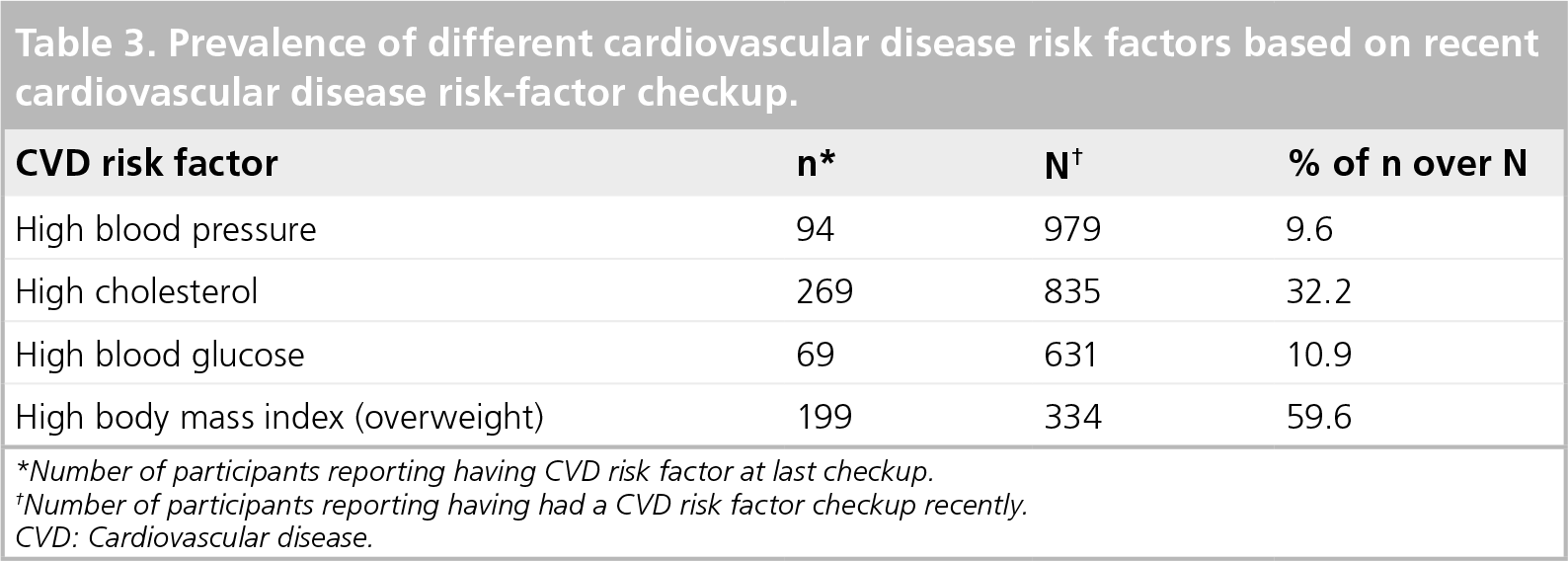
Number of participants reporting having CVD risk factor at last checkup.
Number of participants reporting having had a CVD risk factor checkup recently. CVD: Cardiovascular disease.
The personal awareness for each CVD risk factor (i.e, blood pressure, cholesterol, blood glucose and BMI) for each participant was calculated. The distribution of the participants (as a percentage) was cross-tabulated to examine whether those participants with or without a CVD risk factor can correctly recall the relevant numbers from their last checkup. The participants who were able to recall the numbers pertaining to their risk factors such that they matched their risk status were considered ‘aware’ for that CVD risk factor. The prevalence of personal awareness for each CVD risk factor was then calculated (Table 4).
Cross-tabulation of the results versus recalled numbers for most recent checkups and the prevalence of awareness for cardiovascular risk factors (n = 1044).

Percentage of participants that are ‘aware’ of cardiovascular disease risk, the sum of which appears in the final row of each section.
The associations between personal awareness for each CVD risk factor and the background characteristics, medication use, personal and family history of CVD and the awareness of other CVD risk factors were assessed using binary logistic regression. The odds ratio and 95% CI for each association are presented in Table 5. The presence or absence of awareness for a particular CVD risk factor was considered as the dependent variable, while the background characteristics, medication use, personal and family history of CVD and awareness of other CVD risk factors were the independent variables. All of the independent variables were dichotomous except for participant age, which was used as a continuous variable in the analyses. All descriptive and inferential statistics were calculated using SPSS 16.0 for Windows.
Association of personal awareness of specific cardiovascular disease risk factors with various correlates as quantified by odds ratios (95% CI) using logistic regression.
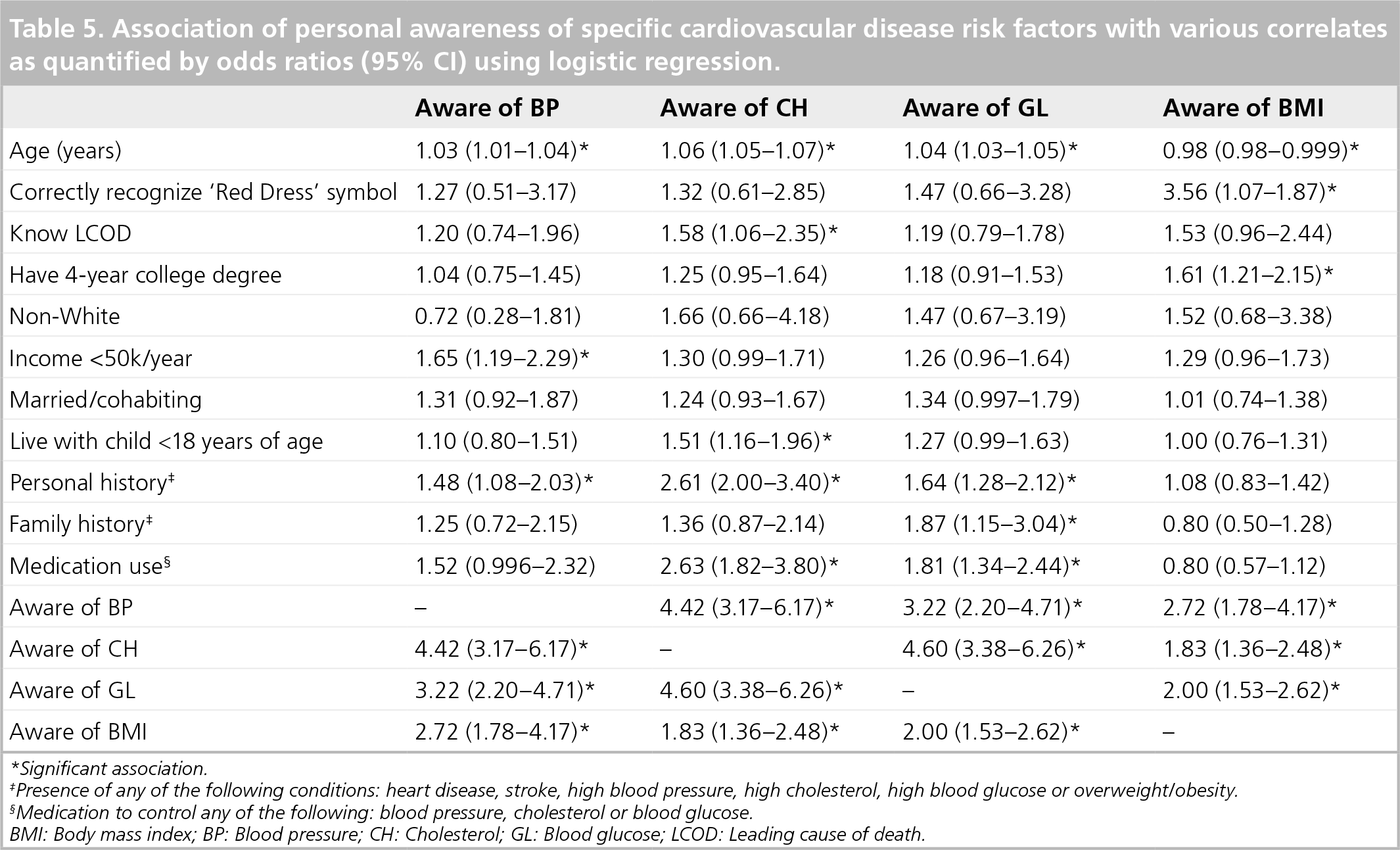
Significant association.
Presence of any of the following conditions: heart disease, stroke, high blood pressure, high cholesterol, high blood glucose or overweight/obesity.
Medication to control any of the following: blood pressure, cholesterol or blood glucose.
BMi: Body mass index; BP: Blood pressure; CH: Cholesterol; GL: Blood glucose; LCOD: Leading cause of death.
Results
The majority of women in this study were middle aged (35–54 years), Caucasian, married or cohabitating, possessed a 4-year college degree and had no children younger than 18 years of age living at home (Table 1). Approximately half of the women were from middle-income households (US$ 35,000–75,000 annually). The reported prevalence of CVD risk factors in this sample of women was 44% obese, 24% high cholesterol, 17% high blood pressure and 5% diabetic. Very few women reported a personal history of heart disease and/or stroke. However, more than half of the participants reported a family history of heart disease, diabetes, high blood pressure, high cholesterol or obesity. Medication use was reported for blood pressure (15% of women), cholesterol (10%) and blood glucose (3%). The majority of the women reported checking their blood pressure (94%) and blood glucose (60%) within the last 12 months, as well as their cholesterol (80%) within the last 5 years. Although 98% of the participants reported their own height and weight, only 32% of the participants reported knowing their own BMI.
More than 89% of all women surveyed perceived heart disease and heart attack as the number one killer of women in the USA, or as their LCOD (Table 2). General cancer (5.1%), breast cancer (3.6%) and lung cancer (0.8%) were the next most common responses. The awareness of heart disease as the LCOD among women of the USA was highest for women below 34 years of age (92%) compared with older age groups. A very high percentage (98%) of participants reported that they had been exposed to the Red Dress symbol, and, of those exposed, virtually all (97%) could correctly identify that the symbol related to women and heart disease. Women in the less than 34 years of age group also showed higher exposure and recognition for the Red Dress symbol than any other age group.
Only 9.6% of the participants reported that the result of their last blood pressure checkup was “high” or “too high” (Table 3). Similarly, 32% reported “high cholesterol”, 10% reported “high blood glucose”, and 59% reported “high BMI or overweight” from their last checkup.
More than 82% of the participants recalled a blood pressure value that correctly matched their risk status, or were considered ‘aware’ (Table 4), with 6.6% reporting high blood pressure and 76% reporting normal blood pressure. Awareness rates for cholesterol (67%), blood glucose (40%) and BMI (29%) were as high as for blood pressure. Participants who reported a high risk in the last checkup, yet were found to be unaware, were considered to be at an even greater risk for CVD (Table 4). This increased risk was noted in 6% of the participants for high blood pressure, 7.4% for cholesterol, 11% for blood glucose and 2% for BMI.
The awareness of CVD risk factors is significantly related to the age of the participants (Table 5). A personal history of CVD risk also had a significant association with awareness of blood pressure, cholesterol and blood glucose, but not with BMI awareness. The awareness of one CVD risk factor had a significant association with awareness of other CVD risk factors. For example, blood pressure awareness had a significant and positive association with the awareness of cholesterol, blood glucose and BMI. Blood pressure awareness also had significant associations with income level and personal history of CVD risk. Apart from associations with age, awareness of blood pressure, blood glucose and BMI, cholesterol awareness also had significant associations with knowledge of heart disease as the LCOD, living with a child younger than 18 years of age, personal history of CVD risk and medication use to control CVD risk factors. Awareness of blood glucose was associated with age, personal history of CVD risk, family history of CVD risk, medication use to control CVD risk factors and awareness of blood pressure, cholesterol and BMI. Awareness of BMI, unlike blood pressure, cholesterol and blood glucose, had a significantly negative association with age. The other characteristics that were associated with BMI awareness were correct recognition of the Red Dress symbol, having a 4-year college degree and awareness of blood pressure, cholesterol and blood glucose.
Discussion
The purpose of the present study was to measure the awareness of general and personal CVD risk among female public employees in ND. This study showed that a very high percentage of par-ticipants perceived heart disease as the LCOD for women in the USA. This percentage is considerably higher than the recent nationwide AHA survey in which 68% of white women perceived heart disease as the LCOD [4]. In this study population, all of the women were employed and had some form of health insurance. Furthermore, a large percentage of the women were Caucasian and had at least a 4-year college degree. These have been consistently cited as key factors in possessing awareness [9] and, given that this population had virtually all of the risk factors, it is a reasonable explanation for the high level of awareness. Another important finding of this study, largely for the same reasons cited previously, was the higher awareness for heart disease as the LCOD among younger women, which is in contrast to previous studies based on national samples [4].
In addition to the demographic factors predictive of high awareness, Go Red North Dakota (GRND) has been providing ongoing CVD health promotion programs in this region since 2007 [103]. GRND runs advertising campaigns for CVD in the mass media (through posters and billboards), print media (through local newspapers, magazines, etc.), electronic media (through radio and television) and digital media (through websites and e-mails). GRND also provides statewide CVD education by organizing Go Red events in the local community, which may include exhibitions, fashion shows, inspirational talks, group physical exercise and promotion of heart-healthy dietary habits. GRND also partners with worksite wellness programs in various small and large, private and public businesses, to encourage people to ‘join the movement’ and sign up for Go Red websites and events, along with other AHA programs. Therefore, the participants in this study are exposed to a variety of messages and events throughout the year regarding heart health, which is supported by results indicating that almost all women surveyed said they had “seen, heard, or read about the Red Dress symbol”, and correctly recognized it as relating to women and heart disease. The exposure and recognition rate of the Red Dress symbol was also much higher than the results of the AHA's national study [10]. The strong co-occurrence of high awareness of LOCD in women and high recognition rates of the Red Dress symbol validates the social marketing strategy for awareness of heart disease in women employed in ND.
Of all CVD risk factors regularly checked, blood pressure checks were by far the most common for women of this study. Cholesterol, blood glucose and BMI were assessed far less often, relative to standard clinical practice guidelines [11]. The apparent inequity of CVD riskfactor checkups in women may be attributed to time, cost, access and logistics; all these elements can serve as either barriers or enablers. Blood pressure checks are frequently offered free of charge and are convenient in most communities, with results available immediately. This makes checking blood pressure cost effective, easily accessible and very quick. Conversely, blood glucose and blood cholesterol checks require scheduling an appointment; they are typically carried out in a hospital or clinic, require a provider's prescription and a co-pay, and the results may take a few days to come through. Therefore, these CVD screenings are not timely, accessible or cost effective when compared with blood pressure checks.
Similar to blood pressure, BMI is relatively easy to check; it is free, can be done almost anywhere (particularly at the same places blood pressure checks occur) and the results are immediate. However, in this present study, only 32% of the women were currently aware of their BMI, although in the answers to a separate question it was revealed that more than 98% of women reported both their height and weight. This low level of BMI awareness may be due to a lack of knowledge in calculating and interpreting individual BMI values, as previously noted [6], or simply that women (and men) are aware of their own bodyweight and do not feel the need to calculate their own BMI.
A high percentage of participants in this study were determined to be personally aware of their blood pressure. However, from a public health perspective, it is the group of women who are unaware of their blood pressure that are most at risk, especially those already at risk and unaware. Although the percentage of such participants is relatively low for blood pressure (5.9%), it is almost twice as high for blood glucose (11%). Interestingly, only 2% of the participants reported a high BMI but were unaware of their specific BMI. However, it is important to remember that BMI was reported by only 32% of all women. Therefore, even with a general unawareness for BMI, those women who report knowing their BMI also have a very high rate of general personal awareness.
The personal awareness of different CVD risk factors was found to be similar across the different risk factors, as awareness of one CVD risk factor is often strongly associated with awareness of other CVD risk factors. Age, socioeconomic status and personal and family history of CVD risk were also associated with personal awareness of CVD risk factors. In addition, knowledge of heart disease as the LCOD or recognition of the Red Dress symbol were associated with personal awareness of particular CVD risk factors.
Future perspective
The participants of this survey were virtually all Caucasian, employed, had some level of healthcare coverage and most had a college degree. These demographics make women more likely to ‘know their numbers’, be aware of heart disease as the LCOD and schedule regular health visits. However, even with these favorable demographics, a considerable unawareness still exists regarding certain CVD risk factors. The unawareness rate of women with less favorable demographics is likely to be even higher. Given these results, and compared to the AHA national data, it seems apparent that continued educational campaigns regarding cardiovascular health risk is important to overall public health. The next logical step, however, is to raise personal awareness of CVD factors, especially for blood glucose and BMI. This may in turn prompt women to recognize both their personal susceptibility to and the severity of CVD, and therefore take action and engage in meaningful behavior change towards reducing their CVD risk.
Executive summary
Women and men have an equal chance of dying from a cardiovascular disease (CVD). In older age, CVD mortality is even higher for women than men. In the past 30 years in the USA, mortality from CVD decreased considerably for men but not for women.
Although one in three women in the USA dies from heart disease, almost two in five women do not consider heart disease as the leading cause of death for women. This unawareness regarding heart disease may lead to less awareness of personal CVD risk factors, and therefore less effort to engage in heart-healthy behaviors.
The World Heart Federation launched Go Red, and encouraged member nations to do the same. The American Heart Association launched Go Red For Women in the USA in 2004, with the aim of raising the general awareness level of the severity and susceptibility of CVD in women.
Increasing general awareness of CVD helps raise the perceived severity of CVD. However, personal awareness of individual CVD risk factors is necessary for increasing perceived susceptibility. When an individual believes that he/she is susceptible to certain CVD risk factors, he/she is more likely to take the recommended action for improving cardiovascular health.
In this study population, the general awareness of CVD was much higher than the national average. Personal awareness of CVD risk factors was also high for hypertension and high cholesterol, although much lower for blood glucose and BMI.
The general awareness on the severity of CVD is quite high in populations with favorable demographics. Personal awareness of CVD risk factors is also high, although not so for blood glucose and BMI. High personal awareness of CVD risk is necessary to raise individual perveived susceptibility to CVD. Refined public health messages will help to educate individuals about their personal CVD risk, such that it will prompt women to make the recommended behavioral changes needed for improved cardiovascular health.
Footnotes
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Appendix 1: The questionnaire for data collection of the ‘Go Red North Dakota’ awareness study
Please choose the appropriate answer corresponding to the following questions. The number of questions you are going to answer may vary depending on your answers.