
Abstract
Assisted reproductive technology (ART) is the most successful treatment for the 9% of people at reproductive age who suffer with infertility, but only a small percentage of those needing ART actually access it. Access varies greatly internationally owing to religious, cultural and political factors, probably the most important factor being each society's perspective on the moral status of the embryo. Economic factors, the nature of the healthcare system and public funding affect access both among and within countries. Regulations and guidelines are highly variable, but critical, in determining access and types of services. Cross-border travel for reproductive care is not uncommon. In the future, better public funding of ART, technological improvements, lower cost and slow international harmonization with fewer differences in ART services will probably increase access significantly.
Keywords
Among couples of reproductive age, 9% experience current infertility and 16% experience infertility at some point in their lives. These rates are consistent internationally [1]. On 25 July 1978, infertility treatment was changed forever when assisted reproductive technology (ART) burst onto the world with the birth of Louise Brown in England, UK. Since that time, ART has evolved extensively. It is now defined as all treatments or procedures that include the in vitro handling of both human oocytes and sperm or embryos for the purpose of establishing a pregnancy. This includes, but is not limited to, IVF and embryo transfer, intracytoplasmic sperm injection (ICSI), gamete intrafallopian transfer, zygote intrafallopian transfer, tubal embryo transfer, gamete and embryo cryopreservation, oocyte and embryo donation, and gestational surrogacy. ART does not include assisted insemination (artificial insemination) using sperm from either a woman's partner or a sperm donor [2]. (Since they are rarely performed, the terms gamete intrafallopian transfer, zygote intrafallopian transfer and tubal embryo transfer will be included in the term IVF unless otherwise stated.) ART has helped millions of infertile patients realize their dream of having a family, with the International Committee Monitoring Assisted Reproductive Technologies (ICMART) estimating that over 3.5 million babies have been born as a result of these technologies from 1978 to 2008 [3,4].
Nevertheless, the availability of ART services varies tremendously around the globe. European countries perform approximately 55% of all the ART cycles in the world, North America 20%, Asia 10%, Middle East 6%, Australia/New Zealand 6% and Latin America 3%. Access to ART ranges from a high of 3263 cycles performed per million inhabitants in Israel to two cycles per million inhabitants in Guatemala, and none available at all in many countries, especially those in Sub-Saharan Africa and other developing countries (see
Assisted reproductive technology cycles performed per million inhabitants in countries worldwide.
Many factors influence access to ART: religious, cultural and political characteristics; economics and relative cost of treatment; the nature of the healthcare system, the availability of high technology services and insurance coverage; government regulations and professional guidelines; and the availability of cross-border reproductive care. This report will review the current global situation with respect to these factors.
Religious, cultural & political factors
There are, of course, major religious differences among the different countries of the world and within individual countries. The primary reason why these religious differences affect access to care is that they have a divergence of opinion on the moral status of the embryo, and this can create societal conflict [5]. The moral and legal status of the embryo are interlinked and are often the key to the acceptability of many procedures that are made available by IVF technology. There can be great legal difficulty in dealing with an entity that is neither a thing nor a person, and on this issue there is great diversity of opinion. Countries with a very strict view of the embryo as a person commonly limit availability of ART services either through religious edict, social discouragement or even legislation. For example, Costa Rica is a strictly religious Roman Catholic country that has banned IVF. Some religions have a more permissive view of the moral status of the embryo, while others have a very restrictive and definitive view, for example, Roman Catholicism. There is a great degree of variation within some religions, such as different types of Protestantism. For example, some Episcopalians tend to be very liberal with regard to the embryo and others are very conservative, considering it to have the moral status of a person, similar to some southern US Baptists who can be extremely conservative. Some religions tend to be pragmatic, but with specific limitations (e.g., Islam). For example, some Muslims have utilized donor eggs, but only if the male takes the egg donor as a wife; subsequently, she may or may not be divorced. Among different countries of the same religion, there can be different interpretations of what is morally correct, possible or desirable. In addition, it is certainly true that individuals of the same socioeconomic level living in the same country and having the same religion can have dramatically different perspectives on the moral status of the embryo and, therefore, how they feel regarding ART and their desire to access it as a solution to infertility. However, overall, religion plays a central role in determining access to ART because it affects individual perspectives, social norms and availability of ART services.
Other cultural forces can either reinforce or counter-balance the effect religions have on the availability of ART. Saudi Arabia and Turkey are both Muslim countries, but Saudi Arabia is very conservative and performs a small number of cycles (<1000 reported in 2002) compared with Turkey, a far more liberal Muslim country, which performed tens of thousands of ART cycles [6]. Therefore, cultural factors can reinforce or mitigate the religious perspective on the moral status of the embryo and the availability of ART services. Political factors can also affect policy. For example, Turkey's desire to join the European Union has led to closer communication between Turkey and European countries regarding the provision of ART services in a manner that is harmonious with that of Europe. A symposium on ‘Data Collection and Prevention of Multiples in ART’ was organized by Turkish professional and government representatives and involved the European IVF Monitoring (EIM) consortium and ICMART and held in Istanbul on 20–21 March 2009. The purpose was to develop improvements that could be implemented in documenting IVF services through a Turkish registry. Even though Turkey has reasonably accessible and very successful IVF services, Turkish leaders expressed their desire to meet the standards found in many European Union countries.
Economic factors
Major economic disparities exist around the world. North America, Europe, Australia/New Zealand, some Middle East countries, Japan and some other Asian countries have very high standards of living and economic prosperity, with annual per capita income in these countries nearing US$40,000 and higher. Many other countries in Sub-Saharan Africa, Latin America, India, China and Asia have annual per capita incomes of less than US$5,000. Since ART involves multiple types of highly specialized health professionals, expensive medications, surgical procedure facilities and sophisticated endocrinology, andrology and embryology laboratories, it is not surprising that ART is a relatively expensive treatment. Wealthy countries can provide more ART services than those less prosperous. Furthermore, poorer countries often have other social and health problems of greater priority than ART.
The number of ART cycles according to public/private health expenditure is much higher in countries with higher gross domestic product per capita [7]. Indeed, some of the poorest countries have high birth rates and it is difficult for some to justify, on a social basis, the need for ART. This, of course, does not mitigate the suffering of the infertile patient. It has been demonstrated that ART is less utilized in countries with higher birth rates (
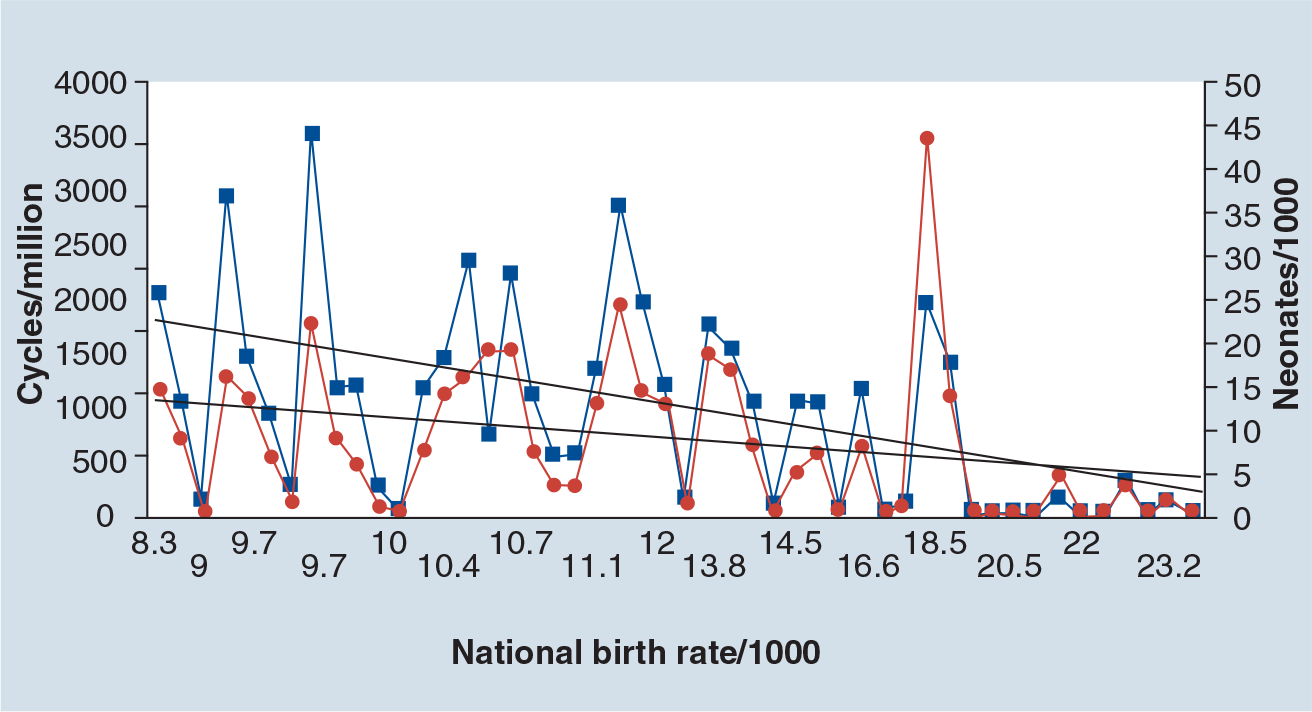
Utilization of assisted reproductive technologies according to national birth rate.
One major review of the health economics of IVF and ICSI involved assessments of utilization, cost, cost–effectiveness and ability to pay. In 48 countries, utilization averaged 289 IVF/ICSI cycles per million of population per annum, ranging from two in Kazakhstan to 1657 in Israel. Higher national utilization of IVF/ICSI was associated with higher quality of health services, as indicated by lower infant mortality rates. IVF and ICSI are scientifically demanding and personnel-intensive, and are therefore expensive procedures. The average cost per IVF/ICSI cycle in 2002 was US$9547 in the USA and US$3518 in 25 other countries. Price elasticity estimates suggested that a 10% decrease in IVF/ICSI cost would generate a 30% increase in utilization. The average cost–effectiveness ratios in 2002 were US$58,394 per live birth in the USA, and US$22,048 in other countries. In three randomized, controlled trials, incremental costs per additional live birth with IVF compared with conventional therapy were US$26,586, US$79,472 and US$47,749, respectively. The national costs of IVF/ICSI treatment were US$1.00 per capita in one model, but the costs to individual couples ranged from 10% of annual household expenditures in European countries to 25% in Canada and the USA [9].
More recent data demonstrate that even in developed countries, great differences in the utilization of ART continue to be evident. This occurs because the cost of ART relative to income can vary relative to the income of the country per capita. The cost of an IVF cycle after government subsidy ranges from 50% of annual disposable income in the USA to 6% in Australia. The cost of treatment reflects the costliness of the underlying healthcare system rather than the regulatory or funding environment [10]. In 2006, the cost of a standard IVF cycle ranged from US$12,513 in the USA to US$3,956 in Japan. The cost per live birth was highest in the USA and the UK at US$41,132 and US$40,364, respectively, and lowest in Scandinavia and Japan at US$24,485 and US$24,329, respectively. The cost of ART treatment does not exceed 0.25% of the total healthcare expenditure in many developed countries. Australia and Scandinavia have levels of utilization that approximates demand, whereas North America only meets 24% of estimated demand. Therefore, ART is expensive from a patient's perspective but not from a societal perspective. Only countries with funding arrangements that minimize out-of-pocket expenses meet expected demand. Demand displays variable price elasticity [10]. The price elasticity of demand (PED) for ART was calculated from the average consumer price of a standard IVF cycle and ART utilization for the countries surveyed. This measure allows the changes in demand and the revenue of the product to be predicted with changes in the consumer price. The formula for the PED is:
% change in quantity demanded ÷ % change in the price of the product.
The general rule is that if a PED is elastic, a rise in price will lead to less spending by consumers, while a fall in price will lead to more spending by consumers. The opposite is true for PEDs that are inelastic. For ART, demand was price elastic in the mid-range of prices but inelastic at the high and low ranges [10].
Healthcare system
The availability of ART can vary greatly from one healthcare system to another. Publicly funded healthcare systems often provide some type of ART coverage, whereas countries with no publicly funded system clearly cannot do this. Generally, the most comprehensive coverage is in Europe; this is reflected in the much higher percentage of ART cycles performed there than in other parts of the world – more than half of all cycles. The USA, with approximately the same population as Europe, performs only a third as many cycles [6].
In publicly funded healthcare systems, different amounts of money are spent in different countries, which will affect how much money might be available for ART. In addition, ART can be given a higher priority as a healthcare service in some countries compared with others. For example, England, UK, has a publicly funded healthcare system, yet only a small proportion of ART cycles are funded by the local healthcare agencies. Other countries, which are substantially less wealthy, such as Turkey, provide coverage for up to two cycles of ART. Australia and Sweden have both public and private sectors to their healthcare systems. In Australia almost all patients receive treatment through the public system, while in Sweden substantial numbers of patients use the private system owing to fewer restrictions and shorter waiting times. Therefore, even among countries providing public funding, different levels of funding can result in extremely variable degrees of access and utilization.
In countries with no publicly funded healthcare system, there can be even wider differences. In the USA there is no national universal healthcare system. However, some states do provide comprehensive care, such as Massachusetts. ART is included in this publicly funded care, so that most Massachusetts residents can receive ART services with very few limitations and good availability. Approximately 14 states have legislation that affects the provision of ART services, some mandating essentially complete coverage (e.g., Massachusetts), others mandating limited coverage (e.g., Illinois and Virginia) and others only mandating that insurance companies offer coverage, but not that employers pay for it; as a result most employers do not offer ART coverage to their employees (e.g., California) [101]. Therefore, ART accessibility is excellent in some states, and poorer in others. Furthermore, the economic status of each state can influence the decision to provide ART coverage.
Regulations & guidelines
Regulations and guidelines have a major impact on access to ART services [5]. Regulations are created by federal or state authorities and are associated with formal state sanctions, such as loss of medical license, fines or prison sentences; guidelines are developed by professional organizations and are usually only associated with professional sanctions, such as requirement for participation in a quality assurance program or loss of membership in the professional organization. Such sanctions do not carry the weight of the state. Blended models with regulations based on professionally developed guidelines are also present in some federal, state and provincial jurisdictions. Furthermore, some countries have federally developed guidelines without legislation, but these guidelines are universally adopted. The different models seem to have the potential for both success and failure; success being defined as a model that enjoys generally wide support of patients, professionals and the public. Some regulatory models appear to be generally successful and some do not, and some guideline models have been generally successful whereas others have not.
Many countries have neither regulations nor guidelines. This appears to be the least successful model, a major reason being that very little is known regarding ART activity in such jurisdictions. If it is not possible to measure a healthcare activity, it is not possible to improve it [11]. Some countries have very restrictive regulations. For example, Italy and Germany severely restrict the creation and cryopreservation of embryos. Donor sperm is allowed in 23 countries and is not allowed in five, with many regulations surrounding its use. Posthumous insemination is controversial, being allowed in 11 countries and not in 19. Donor embryos are not permitted in 13 countries, 15 of 54 countries require identifying information regarding gamete donors if requested, and three require nonidentifying information. Many countries have laws concerning the right to information regarding the donor if necessary for the health of the child. In France, anonymity is protected. Lack of anonymity is a major problem for recruitment in countries such as Australia and the UK and lack of compensation severely limits availability (e.g., in Canada). Fetal reduction is not allowed in eight countries. Preimplantation genetic diagnosis for known genetic conditions is allowed in 20 of 29 regulated countries and 12 of 17 countries with guidelines. Preimplantation genetic screening to identify ‘normal’ embryos is not allowed in six countries with regulations and three with guidelines. IVF surrogacy is performed infrequently, with limitations in many countries, including the need for a panel or court to approve it, availability only in altruistic situations and/or with serious medical conditions, and with restrictions on the marital status of the surrogate and others involved [5].
Although some have hoped that international comparison of regulations and guidelines might lead to standardization of the provision of ART services, it has become clear that this is highly unlikely [5,12]. Indeed, at most international meetings it has now become recognized that different societies, religions and cultures need to have their values respected, and that the best approach is to try to understand what works and does not work in different settings, as well as why this is the case. In this way, each society can develop approaches that are most consistent with its own cultural and socioeconomic settings. When countries are developing regulations or guidelines, it is important to include all the stakeholders in the process. This includes not only policymakers, ethicists and lawyers, but physicians, embryologists, their professional organizations and, most importantly, patients [13].
Overall, approximately 50% of the 57 countries in the International Federation of Fertility Societies Surveillance 2007 regulate and control ART. The laws and guidelines are highly divergent [5]. Only three countries – Belgium, Latvia and the UK – are satisfied with their regulatory environment. Three countries – Germany, Italy and Switzerland – feel the situation is ‘disastrou’ for patients, physicians and biologists. Three countries – Bulgaria, Brazil and Chile – want laws or guidelines. There is no consensus owing to religion, traditions, political situations and medical practices. The authors of the International Federation of Fertility Societies Surveillance 2007 state that international consensus would be ‘the lowest common denominator’ and that the ‘actual situation is illogical, unfair to couples and difficult for doctors and scientist’, but still allows solutions for patients [5].
Cross-border reproductive care
The first international meeting on cross-border reproductive care was sponsored by the Government of Canada in Ottawa in January, 2009 [12]. This meeting brought together a broad range of international stakeholders. It was recognized that respect for the very diverse approaches to reproductive care and its regulation was essential for discourse and progress on this important topic. It was also noted that very few good data exist on this important area of reproductive healthcare. No countries have actual cross- border data in their registries. Some data were available from the USA and some from Europe, but these were very incomplete. An approximate estimate of the amount of cross-border reproductive care was that approximately 3–5% of USA cycles were performed on European, Canadian, Asian and other nationals. In Europe, approximately 7–10% of care was provided to foreign nationals, mainly from other European countries.
It would appear that most patients seek cross-border care in order to avoid restrictive regulations in their own country that limit the general availability of services (e.g., payment to gamete donors and sex selection issues), prevent their own access to services (e.g., age limitations and long waiting times) or intrude on their confidentiality and anonymity (e.g., need to participate in a gamete donor registry). Patients also traveled to access what is perceived as higher quality care (e.g., higher efficacy or safety, more personal and/or convenient care) and/or to access less expensive treatment [14]. Patients often go to countries in which they have relatives. Geographical proximity of services seemed to be important in at least some cross-border travel situations; for example, Swedish women traveling to Denmark for egg donor services. In other cases, cross-border traveling involving long distances did not seem to deter patients; for example, North Americans and Europeans traveling to India for surrogate services. The conclusions from this meeting were that better consent forms and patient information were needed so that physicians could enhance the quality and safety of cross-border care; much better data were needed regarding the type of care for which patients crossed borders, and; the number of patients traveling from and to specific countries needed to be determined. Mechanisms to promote further progress in the understanding of cross-border reproductive care were also needed, such as a database of interested stakeholders, enhanced electronic communication and a biannual meeting of international stakeholders. There is concern that high patient motivation levels, poor information, limited informed consent, unfamiliar cultural and healthcare systems, travel and language difficulties increase the possibility of less efficacious and safe reproductive care in foreign countries.
Cross-border care can also create ethical dilemmas for physicians who have patients desiring services that cannot be provided for legal or other reasons in their country of origin, or who have unrealistic requests in the country of destination, such as requests for social sex selection or replacement of an excessive number of embryos. There is the potential conflict in following national regulations and/or guidelines or social norms versus a physician's professional obligation to their patients. Clearly, laws must be followed. However, the involvement of the physician in providing information, referral services or supportive medical care before or after foreign treatment can be problematic. It would also be ethically and otherwise difficult for a country to forbid travel of its citizens to another country for care, but the country in question might limit funding for services for those who did require subsequent healthcare upon their return; for example, obstetrical care following egg donation. In addition, it would not be unusual for a country to limit access to public funding for foreign patients accessing reproductive services in that country; for example, France currently requires heterosexual cohabitation for unmarried couples for 2 years before permitting access to IVF. Although cross-border reproductive travel can act as a safety valve for a country with many patients leaving for care in other countries, it can also signal a need for individual countries to evaluate their own health policies to ensure that they reflect the needs and desires of their citizens.
Conclusion & future perspective
It is likely that national registries will continue to improve in both number and quality, as ICMART continues to fulfill its mission to have high-quality data on all ART cycles performed globally. However, progress will be slow and will probably be measured in years if not decades, especially in some of the poorer countries of the world. However, constantly improving data will enable policymakers to develop better fertility programs in their own countries and to improve access to services.
The international trend is to improve coverage for ART services. Countries that currently have some types of coverage are tending to increase coverage but are also insisting on more regulation of the services; for example, Belgium currently provides payment when national guidelines regarding the number of embryos to transfer are followed. The determination by the WHO that infertility is a condition that is a public health issue is bringing more legitimacy and attention to this area and is likely to result in more support for better financial coverage and, therefore, more access. There will also be an increased focus on quality, safety and efficacy of services, especially the avoidance of multiple pregnancies. Increased public demand will probably lead to more access as ART becomes more widely accepted socially, is associated with higher pregnancy rates and lower complication rates, and can assist with other medical conditions, such as genetic disorders.
Technological improvements are likely to lead to some reduction in the cost of ART, although the cost of highly trained personnel and facilities will prevent immediate major cost reductions, especially in the private sector where demand for service as well as quality is a contributing cost factor. More automation of embryology services, for example fertilization and incubation techniques, and simpler ovarian stimulation protocols, which are possibly associated with less intensive monitoring, could potentially lead to cost reductions. Serious efforts are now underway within several organizations under the leadership of the WHO to develop infertility services for low resource settings [15]. Furthermore, increased utilization of ART services would lead to lower marginal costs for IVF and would further increase access.
We have seen, and should continue to see, the gradual harmonizing of regulations, guidelines and standards. This will occur as more international sharing of ART experiences occurs through ICMART, the WHO and other international meetings. Continuing international communication and co-operation is furthering cultural harmonization, especially in scientific and medical endeavors. This, along with a reduction in economic disparities between the developed and developing world, should lead to further international standardization of ART services and greater access.
Increased cross-border care would be expected as information regarding ART becomes more accurate, sophisticated and available through the Internet and other sources. Nevertheless, religious, cultural, political and other differences will almost certainly result in some services continuing to be unavailable in some countries compared with others. Newer technologies and research opportunities, particularly in stem cell research, will probably lead to cross-border reproductive travel as sophisticated technologies become more widely available internationally. Differences in quality of care will probably lessen over time, but some differences will undoubtedly remain and cause some cross-border travel. Cost differences will almost certainly remain a factor driving cross-border care in the foreseeable future.
Executive summary
Among couples of reproductive age, 9% experience current infertility and 16% experience infertility at some point in their lives. Assisted reproductive technology (ART) includes effective treatments, but most people needing treatment cannot access care owing to a wide range of complex societal limitations.
Religious, cultural and political characteristics, especially society's perspective of the moral status of the embryo, are the primary factors affecting the availability of ART services.
Access to ART ranges from a high of over 3000 cycles performed per million inhabitants in Israel, where social policy strongly promotes ART, to not being available at all in some countries; for example, in Costa Rica the government has banned ART for religious reasons.
Europe performs approximately 55% of the world's ART cycles, the USA performs approximately 20%.
Economic status of the country is an important factor in determining availability of IVF and access to care, in particular income per capita and the cost of ART relative to income. Very little ART is performed in the world's poorest countries (e.g., Sub-Saharan Africa).
The average cost per IVF/intracytoplasmic sperm injection cycle in 2002 was US$9,547 in the USA and US$3,518 in 25 other countries. Price appears to be elastic in the mid-range but less so at the high end of the range, for example in the USA.
Australia and Scandinavia have levels of utilization approximating demand, whereas North America only meets 24% of estimated demand, despite similar overall economic prosperity.
The availability of public funding in the healthcare system has a major positive impact on the proportion of patients needing ART who actually access it.
Even among countries with publicly funded healthcare, coverage for ART services is highly variable, with lower subsidies being generally associated with less access.
Among countries without publicly funded healthcare, some jurisdictions have chosen to provide coverage (e.g., Massachusetts, USA), which has resulted in markedly increased access.
Regulations are determined by the state and are associated with state sanctions, such as loss of medical license, fines or imprisonment. Guidelines are created by professional organizations and are associated with professional sanctions, such as loss of membership, involvement in quality assessment programs or further education. Many countries have both regulations and guidelines, and many have neither.
Regulations tend to limit or prevent some services from being accessible; for example, donor egg, payment for egg donors, preimplantation genetic diagnosis, posthumous gamete donation and/or require services to be performed in specific ways to protect perceived patient interests (e.g., disclosure rules with gamete donation).
Regulations and guidelines are highly variable internationally, tend to promote safer care and are generally associated with better public funding of ART, but result in many patients not having access to specific ART services that they desire.
Cross-border reproductive care functions as a safety valve for countries with strict ART regulations by allowing patients to obtain desired treatment that is not allowed in their own country. Approximately 3–5% of ART cycles in USA and 7–10% in Europe are provided to patients from outside of the country of service.
Little is known regarding this phenomenon, including accurate numbers of patients involved, types of services sought and specific reasons for individual patient travel.
Concerns exist regarding informed consent, quality and safety of care, and ethical issues for both patients and providers.
Religious, cultural and socioeconomic differences will continue to exist, but slow harmonization of ART services internationally should gradually improve patient access to more effective, safer and less costly care.
National registries will continue to improve in both number and quality and improve our ability to monitor access, efficacy and safety of ART.
Improved public funding subsidies and enhanced insurance coverage for ART services is likely to occur, but will be associated with increased government regulation.
Technological improvements will probably lead to some reduction in the cost of ART, but the cost of private services and sophisticated new technology will remain as barriers to care for many.
Some harmonizing and standardizing of international regulations and guidelines will occur, but religious, cultural and socioeconomic differences will remain, so that ART's unique and challenging ethical issues will continue to be managed differently among countries.
More ART services will be provided in almost all countries but cross-border care for prohibited, new, higher quality or less costly ART services will also probably expand.
However, overall, increased access to ART services should continue as ART services become more accepted in all cultures and more new and potent technologies in diagnosis and treatment become available through ART. Increased volume, technology and competition should drive costs and prices lower. Improved registries, standards and regulation should result in better coverage by governments. Access should continue to improve in most countries, although wide discrepancies will remain.
Footnotes
The author has no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.