
Abstract
Nonalcoholic fatty liver disease (NAFLD) is the leading cause of chronic liver disease in developed countries and is increasing in prevalence with the rise of diabetes and obesity. In addition to obesity and age, gender may also influence the prevalence and severity of NAFLD. However, mechanisms underlying gender-based differences in NAFLD have not been clearly defined. Furthermore, alterations in body composition, fat distribution and/or hormonal or metabolic changes that occur following menopause and in the setting of polycystic ovary syndrome may influence the development and progression of NAFLD. In this article, we will summarize known gender differences as well as the proposed mechanisms for gender differences in NAFLD, review two women-specific issues that may influence the prevalence and severity of NAFLD, menopause and polycystic ovary syndrome, and discuss potential therapeutic options for women with NAFLD who are postmenopausal or have polycystic ovary syndrome.
Keywords
Nonalcoholic fatty liver disease (NAFLD) is an emerging public health concern that parallels the rise in diabetes and obesity [1–5]. NAFLD is characterized as a condition of excess lipid accumulation in the liver (fatty liver or steatosis) not attributed to excessive alcohol consumption. NAFLD, a spectrum of liver damage, encompasses simple steatosis (>5% of liver weight), nonalcoholic steatohepatitis (NASH), an intermediate stage of liver disease, NASH with fibrosis and cirrhosis

Histologic stages of nonalcoholic fatty liver disease.
The reported prevalence of NAFLD in the US general population using the elevated serum aminotransferase is 2.8–13% [2], which is probably an underestimate of the true prevalence owing to the low sensitivity of serum aminotransferases. When more sensitive measures of hepatic fat content (e.g., magnetic resonance spectroscopy or liver histopathology) are used, the prevalence of NAFLD was reported to be as high as 34% in the US population [6,7]. NAFLD is more prevalent among subjects with obesity (especially central obesity), diabetes mellitus, impaired fasting glucose, hyperuricemia, hypertension and dyslipidemia [1]. Although NAFLD is observed to occur in both genders and spans a wide range of age groups, including children, unique age- and gender-related issues pertaining to women do exist. As with other forms of chronic liver disease, gender and hormone status may influence the risk for disease acquisition and progression. Such differences may be attributed to sex hormones and/or changes in hormone levels with aging or with health conditions unique to women such as polycystic ovary syndrome (PCOS). This article will specifically focus on two unique gender-specific conditions that influence NAFLD in women – the postmenopausal stage and PCOS. Furthermore, existing experimental, clinical and epidemiological data supporting the differences in NAFLD in men versus women, as well as the influence of sex hormones on NAFLD will be discussed. Such knowledge may help general practitioners, gynecologists as well as specialists to tailor their approach to the evaluation and management of women with NAFLD.
How do women & men with NAFLD differ?
Both the prevalence as well as the severity of NAFLD may be influenced by gender and/or hormonal state. First, the prevalence of NAFLD is significantly different between genders. Several population-based studies have demonstrated the prevalence of NAFLD to be higher in men than in women [8–14]. The calculated odds ratios (ORs) of NAFLD in men versus women from published literature are summarized in
Gender-specific prevalence of fatty liver/nonalcoholic fatty liver disease and unadjusted odds ratio in published literature.

Estimates were obtained or calculated based on data presented in the cited literature.
Study included subjects with both alcohol and nonalcoholic fatty liver.
In the study by Zhou et al., 87% of those with fatty liver were noted to have NAFLD.
ALT: Alanine aminotransferase; AST: Aspartate aminotransferase; CI: Confidence interval; NA: Not available; NAFLD: Nonalcoholic fatty liver disease; OR: Odds ratio.
Second, the disease progression of NAFLD may also be influenced by gender. In other forms of chronic liver disease (e.g., chronic hepatitis B [HBV] and C [HCV] infection), cirrhosis is more prevalent among men and postmenopausal women. Specifically, studies report that men with chronic hepatitis C are at increased risk of severe fibrosis and disease progression than women [21,22]. Other studies report a favorable role of estrogen in chronic viral hepatitis, suggesting a protective benefit of HRT in fibrosis progression [23–26]. Similarities to the beneficial effect of HRT in HCV may also be drawn with NAFLD, since HCV is also a steatogenic virus. Whether gender influences the progression of NAFLD and, if so, which gender and which physiologic mechanisms are associated with disease progression remain unknown. Some studies have suggested that older age and female gender are associated with severe fibrosis in NAFLD [27–29]. However, menopausal status was not taken into account in these studies. The influence that gender has on fibrosis stage may be impacted by menopausal status. Thus, without such data, the relation between stage of disease and gender alone is difficult to interpret. The influence of gender (or sex hormones) must be evaluated by taking menopausal status into account.
Experimental studies evaluating gender and hormonal status as they relate to the progression of liver disease have been performed. In animal models of liver injury, estradiol – the most potent form of estrogen – has been shown to inhibit hepatic stellate cell proliferation and fibrogenesis [21,30]. Furthermore, estradiol reduces lipid peroxidation in the liver and, thus, is a strong endogenous antioxidant [26]. Since lipid peroxidation in the liver activates hepatic stellate cells and promotes fibrogenesis, reducing lipid peroxidation may be protective against progressive fibrosis in the setting of liver injury [26]. In addition, ovariectomized female rats showed decreased expression of PPAR-α and increased expression of SREBP-1 and SCD-1, which were reversed by the administration of estradiol [31]. Therefore, after menopause, the hepatic ability of fatty acid oxidation may decrease, while lipogenesis is enhanced. These changes further accelerate hepatic fat accumulation and may induce inflammation in the liver of postmenopausal women. Other inherent gender (i.e., sex chromosome) or metabolic (e.g., iron metabolism) differences and/or environmental factors (e.g., alcohol consumption or risk for toxin exposure) may also contribute to gender-differences in NAFLD. Further studies may help to delineate these various factors and their interactions on fibrosis progression with hormonal status and gender.
NAFLD in postmenopausal women
Drastic physiological and biological changes occur in women after menopause. Such changes include fat redistribution (i.e., more visceral fat accumulation) and unfavorable metabolic alterations (e.g., dyslipidemia and glucose intolerance), both of which are associated with increased insulin resistance, cardiovascular disease and NAFLD [17,32,33]. Therefore, a heightened awareness of complications of metabolic and hormonal changes and their association(s) with chronic disease is necessary in the evaluation and care of women who are peri-or postmenopausal. The underlying mechanisms that influence the increased risk for cardiovascular and chronic liver disease in postmenopausal women remain to be fully understood; therefore, interventions targeted at decreasing risk of disease progression are not yet defined. In this section, we will address the influence of menopause on fat distribution and associated metabolic alterations as well as the impact of menopause on the clinical characteristics of NAFLD. The influences of estrogen deficiency on various mechanisms that may be associated with the development of NAFLD are depicted in
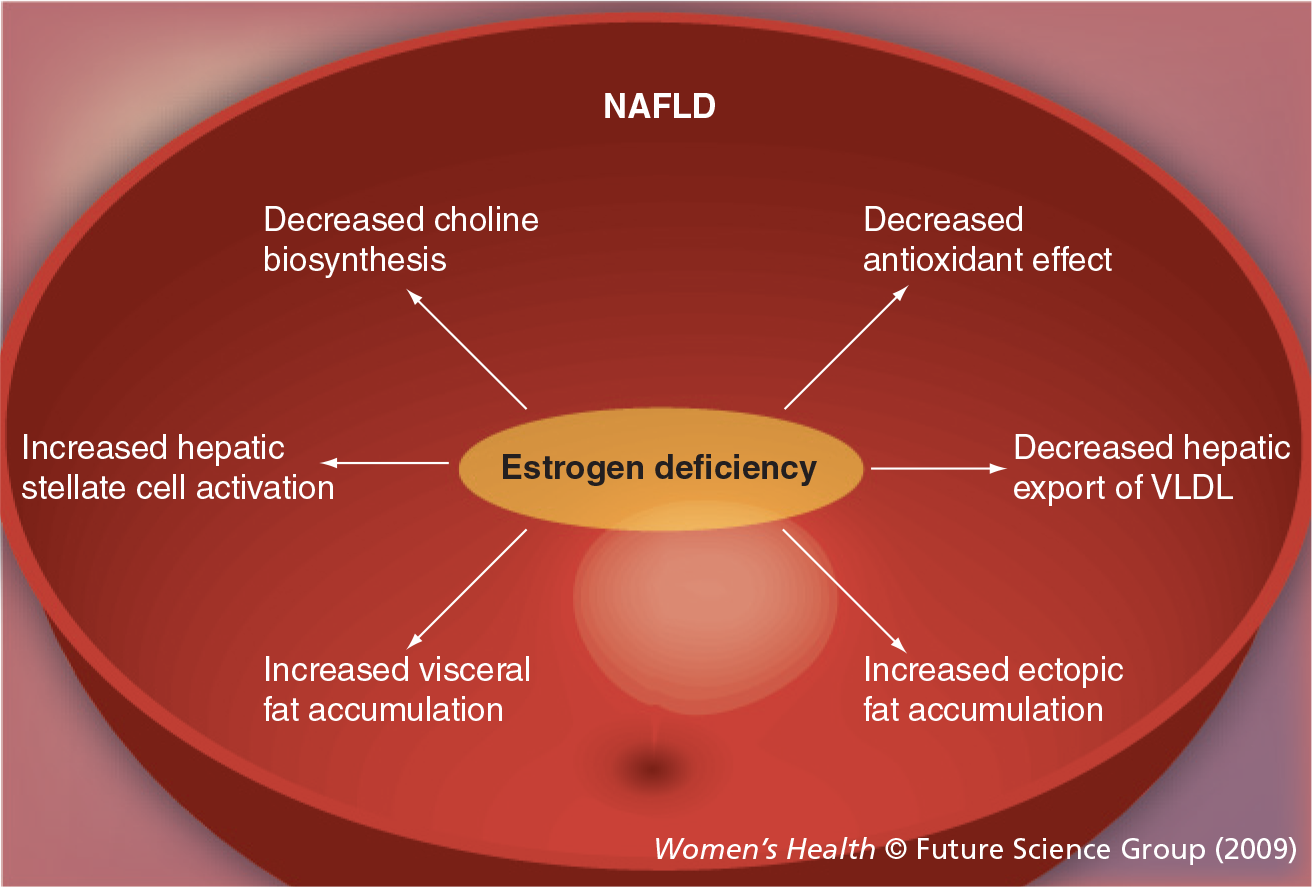
Impact of estrogen deficiency on potential mechanism underlying the development of NAFLD.
Influence of menopause on fat distribution & associated metabolic alterations
Estrogen plays a major role in regulating adipose development and deposition in women. Estrogen may preferentially promote subcutaneous adipose deposition, thus contributing to the increased subcutaneous fat as well as total body fat in women as compared with men [34]. Before menopause, the accumulation of visceral fat among women appears to be inhibited, while men tend to accumulate abdominal fat. However, fat distribution among women significantly changes with aging as well as menopause [33]. With increased age, women gain subcutaneous abdominal fat. Following menopause, total body fat as well as visceral fat increase while energy expenditure and physical activity decrease [33]. The increase in visceral fat accumulation is associated with increased health risks, including insulin resistance, glucose intolerance, dyslipidemia, hypertension, cardiovascular disease and fatty liver disease.
Influence of menopause on NAFLD
As previously mentioned, a higher prevalence of NAFLD has been observed in men than women [8–14]. Interestingly, following menopause, the prevalence of NAFLD in women exceeds that of men [11,12,14,16]. In a population-based study from Japan, the prevalence of fatty liver disease as assessed by ultrasound imaging, increased among women aged above 60 years and exceeded the age-specific prevalence of men [11,16]. The NHANES study, which utilized the presence of serologic-negative elevation of liver aminotransferases to define the presence of presumed NAFLD, demonstrated similar results [17]. The increase in prevalence of NAFLD following menopause suggests that estrogen may be protective against NAFLD and/or its associated risk factors. The NHANES study also demonstrated that the prevalence of NAFLD is higher in postmenopausal women compared with premenopausal women (OR: 2.05; 95% CI: 1.43, 2.94) and is lower in postmenopausal women taking HRT compared with postmenopausal women who did not use HRT (OR: 0.69; 95% CI: 0.48, 0.99) [17].
At present, insufficient data exist regarding the influence of menopause and/or hormonal status on the progression of NAFLD. However, with chronic viral hepatitis, the progression of hepatic fibrosis in women appears to accelerate following menopause and the prevalence of advanced fibrosis is decreased with use of HRT [23,24]. Given the protective effects of estrogen against fibrogenesis, oxidative stress, visceral fat accumulation and its associated metabolic derangements [21,23–26,31], one may presume that postmenopausal women with NAFLD may be at increased risk for advanced fibrosis or cirrhosis. Further studies are needed to evaluate the influence of menopause and the associated change(s) in hormone status not only on the prevalence of NAFLD, but also on the risk of the NAFLD progression.
Current & future preventions/treatments of postmenopausal NAFLD
Following menopause, women are at increased risk of truncal obesity, visceral adiposity, insulin resistance and dyslipidemia [33]. In addition, after menopause, women no longer benefit from the antifibrogenic effects of estrogen [21,25,26]. The increased frequency of steatosis and unexplained elevation of liver enzymes, suggesting underlying steatohepatitis, following menopause may further increase the risk of fibrosis progression. Therefore, the early treatment of the metabolic complications of menopause that may contribute to NAFLD (i.e., insulin resistance, diabetes mellitus, dyslipidemia and obesity) is important [35]. Furthermore, evaluation of postmenopausal women for NAFLD, particularly those with mild elevations of liver aminotransferases, is important since the presence of steatohepatitis as well as complications of insulin resistance increase the risk for advanced liver disease [21]. By targeting pathophysiologic pathways known to be influenced by estrogen, tailored therapeutic interventions may be considered in unique patient subgroups (i.e., postmenopausal women) with NAFLD. Currently, there is no approved pharmacologic therapy for NAFLD. Therefore, lifestyle modification, including diet and exercise, is generally recommended as the first step in the prevention and treatment of patients with this condition. Specific recommendations regarding weight reduction, exercise and dietary choline as well as the role of HRT and melanin concentrating hormone receptor (MCHR)1 antagonists as potential pharmacologic modalities for postmenopausal women with NAFLD will be discussed below.
Weight reduction & exercise among postmenopausal women
In general, weight reduction is beneficial for complications of insulin resistance, including NAFLD [36]. Weight reduction improves plasma lipid profiles, glucose intolerance, high blood pressure and reduces intrahepatic fat [36–38]. Therefore, weight reduction for postmenopausal women who have metabolic alterations and risk factors for NAFLD should be strongly recommended. However, the approach to weight reduction among older women requires special attention. Significant weight reduction could accelerate the loss of lean tissues, both skeletal muscle and bone mass among older subjects [37], which may facilitate osteoporosis, bone fracture and, thus, promote a decline in physical function. Furthermore, the required weight loss necessary to achieve beneficial health outcomes among older subjects may be different from younger subjects [37]. Modest (3–4 kg), sustained weight loss may be sufficient and has been associated with improvements in the metabolic abnormalities associated with menopause and insulin resistance. In order to avoid adverse loss of lean mass, integrating dietary modification with routine exercise is important. Previous studies suggest that both aerobic and resistance training are beneficial in preventing bone loss during weight loss [39–41]. Interestingly, a recent animal study suggested that the addition of resistance training to restricted diets totally prevents hepatic and intra-abdominal fat accumulation caused by ovariectomy [42]. Thus, resistance training could prevent the unfavorable fat redistribution and its associated adverse health effects, including hepatic steatosis, following menopause in women. No consensus regarding the type of exercise that would offer the maximum health benefit for postmenopausal women currently exits. Further studies are necessary to better define the ideal form of lifestyle modifications that should be recommended to postmenopausal women with NAFLD. Furthermore, there are insufficient data on the role of bariatric surgery for older morbidly obese women with NAFLD. Comorbidities (e.g., hypertension, diabetes mellitus, dyslipidemia and cardiovascular disease) may increase surgical risk and complications in older adults. Although antiobesity surgery can be performed safely in unselected populations of obese patients with low rates of early mortality, bariatric procedures in older patients may be associated with a higher complication and reoperation rate [43].
Dietary choline
Several recent studies emphasized the significance of dietary choline as an essential nutrient and cellular constituent [44,45]. Choline functions as a methyl donor in cellular metabolism and is a precursor of phosphatidylcholine, an indispensable component of cell membranes and very low-density lipoprotein, which are required for exporting triglycerides from the liver. Therefore, depletion of choline inhibits hepatic triglyceride export and induces fatty liver in methionine–choline and choline-deficient mouse models of fatty liver disease [46]. Choline can also be derived from the de novo synthesis of phosphatidylcholine via phosphatidyletha-nolamine-N-methyltransferase (PEMT) using S-adenosylmethionine (SAM) as a methyl donor. The activity of PEMT is upregulated by estrogen and differs between genders with woman having higher PEMT activity than men [47,48]. Based on this gender difference, the recommended adequate intake of choline is 550 mg choline/day for men and 425 mg choline/day for women [49.] However, following menopause the endogenous supply of choline decreases owing to estrogen deficiency; therefore, the daily requirement of choline is increased. When compared with premenopausal women, postmenopausal women were more likely to develop hepatic steatosis with short-term depletion of choline from their diets [44]. Whether dietary supplementation of choline helps to prevent and/or ameliorate fatty infiltration of the liver in patients with NAFLD remains unknown. Further studies are required to determine preventive/therapeutic efficacy of choline in postmenopausal NAFLD.
HRT
Considering the above-mentioned protective effects of estrogen, the replacement of estrogen in postmenopausal women might be one consideration for the prevention and/or treatment of NAFLD. In fact, a randomized, controlled trial of women with diabetes mellitus demonstrated 6 months therapy with low-dose continuous combined HRT (17β-estradiol 1 mg and norethisterone acetate 0.5 mg) was beneficial for presumed NAFLD as defined by liver enzyme elevation. Relative to placebo recipients (n = 23), women randomized and compliant to HRT (n = 19) demonstrated statistically significant reductions in liver aminotransferases [50]. The Women's Health Initiative Trial, a large randomized, controlled, primary-prevention trial of postmenopausal women aged 50–79 years, designed to assess the major health benefits and risks of the most commonly used combined hormone preparation in the USA, demonstrated a detrimental effect of HRT on cardiovascular events, and ended with an early termination of the trial [51]. However, HRT was associated with decreased incidence of diabetes mellitus even after adjusting for BMI or waist circumference [52]. Since diabetes mellitus is a well-known risk factor for advanced NAFLD, the prevention of diabetes is a logical preventive modality for the development and progression of NAFLD. Nevertheless, treatment of postmenopausal women with NAFLD with long-term HRT may cause a doubling of the rate of breast cancer [53] and cardiovascular disease and stroke [54.] These complications dampen the enthusiasm for use of HRT for postmenopausal estrogens. Future studies may help to delineate whether a unique population of postmenopausal women with NAFLD may derive beneficial health effects from HRT.
Novel pharmacologic approaches to treatment of NAFLD in postmenopausal women
Melanin concentrating hormone (MCH) is a cyclic neuropeptide that is expressed in the lateral hypothalamic area, an area regulating energy metabolism in the brain. Overexpression of MCH [55] or chronic intracerebroventricular infusion of MCH [56] in mice induces weight gain and insulin resistance, through increasing food intake and decreasing energy expenditure. By contrast, mice that received a MCH1 antagonist [57] and MCH1 receptor-knockout mice [58] have normal body-weights, yet are lean, have reduced fat mass and are less susceptible to diet-induced obesity. The MCH1 receptor has received significant attention as a potential target for antiobesity treatment. Recent animal studies suggest that estrogen directly modulates MCH production and release from the hypothalamus. Estrogen influences gene expression of MCH [59], and hyperestrogenemia inhibits MCH mRNA expression in the hypothalamus [60]. Furthermore, chronic administration of MCH1 antagonist ameliorates ovariectomy-induced obesity and the development of fatty liver [61]. MCH1 antagonist also alleviates histological findings of high-fat diet-induced steatohepatitis [62]. Considering the physiologic effects of MCH1 antagonists, these agents may play a future therapeutic role in the treatment of NAFLD in postmenopausal women. A few MCH1 antagonists are currently under investigation in early phase clinical studies.
Summary
Data from experimental, clinical and epidemiological studies suggest that postmenopausal women are at increased risk of NAFLD. Whether postmenopausal women are at increased risk of advanced NAFLD remains unclear. Further investigation of the influence of sex hormones (i.e., estrogens and androgens) are important areas for future research so that the role of individualized prevention and treatment strategies for postmenopausal women with NAFLD may be better defined.
Polycystic ovary syndrome
Polycystic ovary syndrome is a common endocrine disorder, affecting 5–11% of reproductive age women [63,64]. This disorder is characterized by irregular menstrual cycles and laboratory and/or clinical evidence of hyperandrogenism, such as hirsutism, acne, male pattern scalp hair loss and polycystic ovaries [65]. Although not part of the diagnostic criteria, significant metabolic abnormalities have been associated with PCOS, including insulin resistance [66], Type 2 diabetes mellitus [67,68], dyslipidemia [69], hypertension [70] and, possibly, cardiovascular disease [71–73]
Prevalence of NAFLD in women with polycystic ovary syndrome
Several small studies have recently suggested that women with PCOS may be at an increased risk for NAFLD [66,74–77]. A retrospective study of 70 women with PCOS evaluated in an infertility clinic found abnormal alanine aminotransferase (ALT) activity in 30%, a prevalence much higher than expected using population-based estimates, even after accounting for the risk factors of diabetes, obesity and Hispanic ethnicity [75]. Another study demonstrated ultrasound evidence of hepatic steatosis in 48 of 88 (55%) women with PCOS, nearly 40% of whom were lean women. High BMI and insulin resistance appeared to be important associated factors [74,75]. Interestingly, of the 55% of woman noted to have ultrasound evidence of hepatic steatosis, 15% had elevated liver chemistries [74,75]. Whether these women are at an increased risk for progressing to NASH and/or cirrhosis is unknown. The presence of increased ALT changes are suggestive of progression; therefore, liver biopsy may be indicated in instances where the ultrasound shows severe changes with high levels of ALT in a patient (particularly obese) with features of the metabolic syndrome as well as obesity. Two studies of adults with abnormal liver tests who were referred to hepatologists concluded that advanced NAFLD was rare before the age of 45–50 years [27,78]. Thus, it might be argued that young women with PCOS are unlikely to have liver damage. By contrast, the young age of these women could have important prognostic implications for developing liver complications later in life. In a prospective study of 41 women with PCOS, 63% had insulin resistance and 41% had NAFLD as diagnosed by abdominal ultrasound following exclusion of alternative causes of liver disease [74]. In a retrospective study of 200 women with PCOS seen at a university-based endocrinology clinic, 15% had aspartate aminotransferase (AST) and/or ALT more than 60 U/l [77]. Women with aminotransferase elevations had lower high-density lipoprotein (HDL) (41 vs 50 mg/dl; p = 0.006), higher triglycerides (174 vs 129 mg/dl; p = 0.024) and higher fasting insulin (21 vs 12 μ International Units/ml; p = 0.036) compared with women with normal aminotransferases. Of the six women (mean age: 29 years) who underwent liver biopsy for persistent aminotransferase elevation, all had NASH with fibrosis. This study demonstrated that abnormal aminotransferase activity is relatively common in women with PCOS and is associated with high triglycerides, low HDL and elevated fasting insulin levels, compared with women with PCOS without biopsy-proven NAFLD [77]. Thus, these characteristics of the metabolic syndrome of insulin resistance may help to identify PCOS women who are at increased risk of fatty liver disease. The young age of many women with PCOS, and the relatively advanced stage of NASH observed on the biopsies suggest the possibility of significant risk for long-term complications from liver disease. Therefore, women with PCOS should be screened for liver disease. A longitudinal study following women with PCOS and NAFLD may provide important insights into the risk for disease progression.
Treatment of NAFLD in women with polycystic ovary syndrome
Diet & exercise
The current treatment of NAFLD in women with PCOS targets the metabolic complications of insulin resistance. Lifestyle interventions, such as diet and exercise, are first-line treatment for women with PCOS, particularly if they are overweight [79]. Several nonrandomized trials have demonstrated that a reduction in bodyweight through diet and exercise improved insulin sensitivity and ovulation rate. In other populations, a weight loss of 5–7% decreases the conversion from impaired glucose tolerance to Type 2 diabetes by 58% over a 3-year period [80]. Likewise, diet and exercise is effective in improving liver aminotransferases, liver histopathology and/or hepatic lipid content in patients with NAFLD [81–83]. The beneficial effect of modest weight loss and exercise with substantial decrease in steatosis and inflammation on repeat liver biopsy in a woman with PCOS and severe NASH has been reported [84].
Pharmacologic therapy
Metformin, an oral antidiabetic drug from the biguanide class, improves ovulation, insulin sensitivity and, possibly, hyperandrogenemia [85]. It is commonly used to treat infertility, either alone or in combination with clomiphene citrate. Since it increases ovulation in some women, it can also increase the frequency of endometrial shedding and may help with controlling the cycle. In patients with NAFLD, several small pilot studies of up to 6 months duration using metformin at doses of 1.0–1.5 g/day have shown improvement in ALT levels compared with baseline [86–89]. Other pilot studies using metformin 1.5–2.0 g/day have revealed improvements in biochemistry, insulin sensitivity with ultrasound echogenicity [90] and variable changes in histology [90,91]. In small pilot studies that evaluated the impact of metformin on follow-up liver biopsies in patients with NAFLD, improvements in steatosis, inflammation and fibrosis have been observed [90–92]. However, confirmation of results from these pilot studies in a double-blind trial with appropriate statistical power based on liver histology is necessary.
The thiazolidinediones are promising therapies for NASH in women with PCOS because they reduce insulin resistance by improving sensitivity to insulin in muscle and adiopose tissue and inhibit hepatic gluconeogeneis. The thiazolidinediones, potent PPAR-γ agonists, are also attractive therapeutic agents for chronic liver disease owing to their antifibrotic properties. Troglitazone, the first available agent in this drug class, has been the most studied thiazolidinedione for the treatment of PCOS. Trials evaluating the effect of troglitazone in patients with PCOS demonstrated that troglitazone was effective in decreasing hormone levels associated with PCOS, such as dehydroepiandrosterone, testosterone and estradiol, and in improving clinical outcomes, such as increased ovulation rates [93–95]. The PCOS/Troglitazone Study Group conducted the largest trials performed thus far assessing a thiazolidinedione in patients with PCOS [96]. They study enrolled 410 women with PCOS and evaluated four groups of patients receiving treatment for 48 days with troglitazone 150, 300 or 600 mg/day or placebo. In 305 women who met the evaluation criteria, a significant increase in ovulation rate was observed in the troglitazone 300- and 600-g groups versus placebo (p < 0.02 and p < 0.0001, respectively). Troglitazone also improved hirsutism, circulating insulin, fasting glucose and hemoglobin A1c (HbA1c). In a small pilot study, troglitazone improved the biochemical and histologic features of NASH [97]. However, troglitazone proved to be hepatotoxic and was withdrawn from the market after the report of several dozens of deaths or cases of severe hepatic failure requiring liver transplantation [98,99].
Characteristics of polycystic ovary syndrome.
Obesity
Enlarged ovaries with multiple cysts
Irregular or no menstruation
Infertility
Acne
Skin tag
Acantosis nigricans
Hirsutism
Male pattern baldness
Insulin resistance
Hypothyroidism
Hypertension
Hypercholesterolemia
Elevated levels of C-reactive protein
Nonalcoholic steatohepatitis
Sleep apnea
Excess daytime sleepiness
Elevated serum IL-6
More recently, smaller trials of rosiglitazone and pioglitazone have had promising results for PCOS and NAFLD. However, these benefits need to be confirmed in larger studies. A randomized, double-blind, controlled trial investigating premenopausal women with PCOS (n = 40) demonstrated that pioglitazone 30 mg/day) for a period of 3 months diminishes insulin resistance, hyperandrogenism and enhances ovulation rates compared with placebo [98]. In addition, pioglitazone treatment demonstrated improvement in hirsutism score, restoration of menstrual cycle and decrease in luteinizing hormone and luteinizing hormone:follicle-stimulating hormone ratio [100]. Thus, pioglitazone significantly improved insulin sensitivity, hyperandrogenism and ovulation rates in women with PCOS, thereby providing both metabolic and reproductive benefits [100,101]. A prospective, open-label study of rosiglitazone in insulin-resistant PCOS women (n = 42) promoted ovulation and dose-dependently decreased insulin resistance and insulinemia; ovulators had lower circulating insulin and testosterone [100–102]. In a prospective study of insulin-resistant women with PCOS (n = 24), a significant decrease in serum-fasting insulin, area under the curve for insulin, HOMA index, β-cell function, IGF-1, luteinizing hormone, and waist:hip ratio was observed in treatment with rosiglitazone. A total of 22 of 23 women had their menses restored, and three patients became pregnant [103]. Therefore, pioglitazone and rosiglitazone have been shown to improve the endocrine reproductive condition in insulin-resistant women with PCOS [98,100–103]. Likewise, the role of pioglitazone and rosiglitazone for treatment of NAFLD has been evaluated in small pilot studies for NAFLD. Two, well-designed pilot studies using pioglitazone 30 mg/day [104,105] and rosiglitazone 4 mg twice daily [106] demonstrated improvement in liver aminotransferases, radiologic and/or histologic end points [104,106]. Pioglitazone, but not rosiglitazone, was associated with improvement in the overall fibrosis stage. In a recent placebo-controlled trial that compared diet plus pioglitazone (n = 26) with diet plus placebo (n = 21), pioglitazone improved glycemic control and glucose tolerance (p < 0.001), normalized liver aminotransferase levels as it decreased plasma AST levels (40 vs 21%; p = 0.04), decreased ALT levels (58 vs 34%; p < 0.001), decreased hepatic fat content as measured by means of magnetic resonance spectroscopy (54 vs 0%; p < 0.001) and increased hepatic insulin sensitivity (48 vs 14%; p = 0.008) [107]. Administration of pioglitazone improved the histologic features of steatosis, ballooning necrosis and necroinflammation compared with placebo [107]. However, the reduction in fibrosis did not differ significantly from that in the placebo group [107]. In a recent randomized, placebo-controlled study of nondiabetic patients with histologically proven NASH (n = 74) randomized to 12 months of standard diet, exercise and either placebo or pioglitazone 30 mg/day, pioglitazone therapy was associated with an increase in weight and a reduction in glucose, HbA1c, insulin C peptide level and ALT level. Histologic features including hepatocellular injury and fibrosis were reduced in patients treated with pioglitazone compared with those in the placebo group [108].
Despite these promising results, thiazolidinediones are not approved for use in patients with chronic liver disease, may increase weight, cause edema and, possibly, liver enzyme abnormalities. Since thiazolodinediones are category C drugs, women with PCOS should be counseled to use contraception while taking this medication. The rationale for determining whether patients with PCOS having fatty liver and NASH, as well as approach to treatment will be strengthened as data regarding treatment for NASH, currently being studied in a NIH multicenter trial become available [109,110].
Summary
Polycystic ovary syndrome is commonly associated with insulin resistance and significant metabolic abnormalities that increase the risk for NAFLD. Owing to the lack of large randomized, controlled trials evaluating the role of insulin-sensitizing agents for women with NAFLD and PCOS, current recommendations remain diligent regarding the counseling of patients for lifestyle interventions, such as diet and exercise, as first-line treatment. In women with PCOS and elevated liver enzymes, liver biopsy should be considered for the evaluation of advanced liver disease. If present, treatment may be tailored to aggressively treat the associated insulin resistance observed in PCOS patients (i.e., impaired glycemic control, hyperlipidemia and obesity). Further research is necessary to better define the impact of insulin-sensitizing agents on the histologic features of NAFLD in women with PCOS.
Conclusion & future perspective
Gender and gender-related factors are associated with risk for acquisition and disease progression of NAFLD. A better understanding of the mechanisms underlying these gender differences (i.e., levels of sex hormones, change in anthropometric measures, body fat distribution or change in metabolic profile) will allow for targeted prevention and intervention strategies to be developed. At present, limited clinical data are available to justify a different approach to therapy of NAFLD in women. However, given the unique aspects of care associated with aging and hormonal changes that occur in menopause and with PCOS, individualized therapeutic strategies will be required in the future. For now, heightened awareness of the increased risk for NAFLD following menopause and with PCOS is necessary. Given the increased risk for fibrosis progression, postmenopausal women and those with PCOS should undergo further evaluation of chronic liver disease.
Executive summary
Nonalcoholic fatty liver disease (NAFLD) is a disease condition of excess hepatic lipid accumulation, not caused by excess alcohol use.
NAFLD became the most common etiology of chronic liver diseases in the USA as obesity increased, and is more prevalent among subjects with obesity and clinical feature of metabolic syndrome.
The prevalence of NAFLD is significantly different between genders and is higher in men than in women.
Clinical evidence in other chronic liver disease (i.e., chronic viral hepatitis) and evidence in experimental models suggest that estrogen may be protective against the NAFLD progression.
After menopause, total body fat as well as visceral fat increase and unfavorable metabolic alterations, such as insulin resistance, may occur.
Prevalence of NAFLD in women increases after menopause and exceeds that of men. The prevalence is lower among women taking HRT compared with women who did not use HRT.
Postmenopausal women with NAFLD may be at increased risk for advanced fibrosis or cirrhosis, despite the lack of sufficient clinical data.
Weight reduction and exercise may be beneficial among postmenopausal women. However, the approach to weight reduction requires special attention since significant weight reduction could accelerate the loss of lean tissues. Modest (3–4 kg), sustained weight loss and exercise may help to prevent bone and muscle loss during weight loss.
Postmenopausal women were more likely to develop hepatic steatosis with short-term depletion of choline from their diets compared with premenopausal women. The decrease in de novo synthesis of phosphatidylcholine following menopause necessitates an increase in daily choline requirement. Efficacy of dietary choline supplementation in postmenopausal NAFLD remains unknown.
A randomized, controlled trial of women with diabetes mellitus demonstrated 6 months therapy with low-dose continuous combined HRT decreased liver enzyme elevation with presumed NAFLD; however, the risk–benefit ratio of long-term HRT therapy for NAFLD has not been defined.
Melanin concentrating hormone 1 antagonists may inhibit the development of obesity and NAFLD and have a future therapeutic role in the treatment of NAFLD in postmenopausal women.
Polycystic ovary syndrome (PCOS) is a common endocrine disorder, affecting 5–11% of reproductive age women, characterized by irregular menstrual cycles, hyperandrogenism and polycystic ovaries. PCOS is frequently associated with various metabolic abnormalities, such as insulin resistance, dyslipidemia and hypertension.
Women with PCOS may be at an increased risk for NAFLD. Therefore, women with PCOS should be screened for liver disease. However, whether women with PCOS are at an increased risk for advanced fibrosis or cirrhosis is unknown.
Modest weight loss and exercise are beneficial in a woman with PCOS and severe nonalcoholic steatohepatitis (NASH) and improves hepatic steatosis and inflammation.
Metformin improves ovulation, insulin sensitivity and, possibly, hyperandrogenemia, and may improve NAFLD in women with PCOS.
Clinical trial data of various thiazolidinediones has demonstrated promising results treating women with PCOS as well as patients with NASH. Thiazolidinediones are effective in improving insulin sensitivity, hyperandrogenism and ovulation rates in women with PCOS, and ameliorating NAFLD histology, including fibrosis stages. Currently, thiazolidinediones are not approved for use in patients with chronic liver disease. The role of thiazolidinediones in the treatment of NASH in patients with PCOS requires further evaluation.
Footnotes
Acknowledgement
The authors thank Dr Anna Mae Diehl for her critical review of this manuscript.
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.