
Abstract
Ixabepilone (BMS247550) is a semisynthetic derivative of the natural product that optimizes the properties observed with epothilone B. This compound has some similarities with taxanes in targeting and stabilizing microtubules, but it also has major differences. Interestingly, ixabepilone was evaluated in patients with well-characterized resistance to taxanes and was able to overcome the overexpression of multidrug resistance and was unaffected by mutations in the β-tubulin genes. The interest in ixabepilone was clinically confirmed in Phase II and III clinical studies, which have demonstrated a strong activity in patients with metastatic breast cancer resistant to taxanes and in patients suffering from other types of chemoresistant tumors.
Keywords
Breast cancer is the most prevalent malignancy in women, with more than 1 million women worldwide diagnosed with breast cancer every year. Metastatic breast cancer (MBC) is a leading cause of mortality, accounting for more than 400,000 deaths annually worldwide [1]. MBC remains incurable and the administration of chemotherapy is palliative. Anthracycline- and/or taxane-containing regimens represent the most active chemotherapy able to significantly prolong survival at the metastatic setting [2]. These drugs represent a standard in the treatment of metastatic disease even when they are commonly proposed as an adjuvant therapy of early breast cancer [3]. One could anticipate that growing numbers of patients will have pretreated MBC with a tumor resistant to anthracyclines and taxanes [4]. Limited options are available for such patients [5]. Capecitabine, the oral prodrug of 5-fluorouracil, is currently the only chemotherapy agent approved in some countries for the treatment of advanced breast cancer in patients who have failed or are resistant to both an anthracycline and a taxane. Capecitabine's approval was supported by a multi-center Phase II study that demonstrated significant antitumor activity with an overall response rate of 20% (95% CI: 14–28) [6]. Nevertheless, one can consider that we have an urgent need of new agents able to provide substantial activity after a previous exposure to taxane- and/or anthracycline-containing regimens.
The epothilone family constitutes a new class of nontaxane tubuline-binding agents. Epothilones have some similarities to taxanes in targeting and stabilizing microtubules, however, they also have important differences [7]. These two families target at or near the same binding site on the β-tubulin subunit, but the structural characteristic of epothilones provides a low susceptibility to major well-known mechanisms of tumor resistance to taxanes, including changes in tubulin isotypes and/or tubulin mutations [8]. Moreover, the epothilones can be distinguished from the taxanes by their ability to overcome a resistance linked to cell membrane transporters mediated by P-glycoprotein and multidrug resistance protein (MRP). In total, the epothilones are distinguished from the taxanes structurally and functionally and have been demonstrated in vitro and in preclinical models to have superior cytotoxic potency to the taxanes [9].
Several agents of this family are under clinical development: Patupilone (EPO 906; Novartis, Switzerland) a natural epothilone B, and several synthetic derivatives including ixabepilone (BMS-247550, Bristol Myers Squibb, NY, USA), ZK-EPO (ZK-219477, Schering AG, Germany), KOS-862 and KOS 1584 (Kosan Biosciences, CA, USA)
Family of epothilones.

This article presents an overview of the current state of development of ixabepilone and provides a focus of its potential use in the treatment of breast cancer.
Ixabepilone clinical development
Phase I trials
Phase I trials studied the administration of ixabepilone once every 3 weeks [12–14]. The maximum tolerated dose (MTD) was established as 50 mg/m2, and four limiting toxicities were observed: neuropathy, neutropenia, stomatitis and myalgia. It has been proposed that the neuropathy associated with the therapeutic use of a tubulin polymerizing agent such as paclitaxel, is related more to its peak concentration than to the overall area under the curve. Based on these considerations, the recommended dose of ixabepilone was decreased from 50 to 40 mg/m2 and, knowing from the paclitaxel experience that prolonged infusion is associated with an increase in myelo-suppression and mucositis, ixabepilone was administered via a 3-h infusion.
A fourth study investigated a schedule of ixabepilone given at a 1-h infusion for 5 consecutive days every 3 weeks [15]. The MTD was 6 mg/m2/day with neutropenia as the limiting toxicity and, interestingly, with mild neurotoxicity.
Phase II trials
Five Phase II studies assessed the activity of ixabepilone in several subsets of MBC patients according to their tumor resistance or sensitivity to taxanes, anthracyclines and capecitabine. Those studies are summarized in
Phase II studies assessing the activity of ixabepilone in metastatic breast cancer.
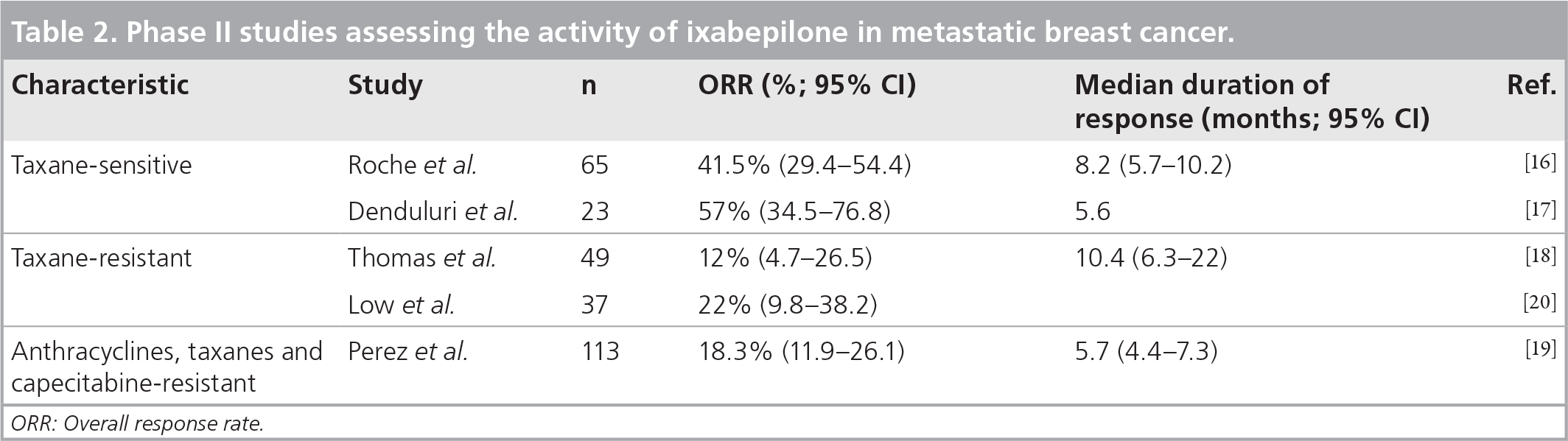
ORR: Overall response rate.
In 65 taxane-naive patients who had received a prior anthracycline-based regimen as adjuvant treatment, ixabepilone, as a first-line metastatic chemotherapy, was administered at 40 mg/m2 for 3 h every 3 weeks. An overall response rate (ORR) of 41% (95% CI: 29.4–54.4) was achieved and the median duration of response was 8.2 months (95% CI: 5.7–10.2 months) [16]. Another trial with taxane-sensitive patients assessed the administration of ixabepilone at 6mg/m2/day on day 1 through 5 every 3 weeks and showed an ORR of 57% (95% CI: 34.5–76.8) in 23 patients. The median duration of response from date of first documentation of response was 5.6 months [17].
In 49 patients with taxane-resistant MBC, the ORR was 12% (95% CI: 4.7–26.5) in the cohort treated at a dose of 40 mg/m2 over 3 h [18]. Strikingly, among 126 patients with a tumor resistant to anthracycline, taxane and capecitabine, the ORR was 18.3% (95% CI: 11.9–26.1) [19]. This study appears to be the first one that demonstrated an activity in this unmet situation of patients with an anthracycline–taxane–capecitabine-resistant tumor.
Interestingly, a Phase II trial assessed the administration of ixabepilone at 6 mg/m2/day on day 1 through 5 every 3 weeks in patients previously exposed to taxane-containing therapy [20]. An ORR of 22% was reported with a different toxicity profile including a lower rate of neuropathy. This finding warranted future studies to compare various schedules.
Toxicity profile
Currently, the majority of available completed data concerns safety of ixabepilone at 40 mg/m2 given as a 3-h infusion. Treatment-related adverse events were mostly grade ½, generally reversible and one can consider that ixabepilone demonstrated a manageable and acceptable safety profile.
Grade 3/4 toxicities in metastatic breast cancer patients treated with ixabepilone.

*240 patients.
‡D37 patients.
§369 patients.
Peripheral neuropathy was a dose-limiting toxicity in Phase I monotherapy trials of ixabepilone, and cumulative neuropathy was reported in the Phase II trials. This problem appears to be the major relevant toxicity. This is dose-dependent and may also be schedule-related, as it is cumulative and generally reversible [21]. With ixabepilone administered at 40 mg/m2 as a 3-h infusion, severe peripheral neuropathy generally developed after a median of four treatment cycles (range: 1–11). With dose reduction, most patients remained on therapy without any worsening of their neuropathy and after completion of treatment neuropathy resolved with a median time to resolution of 5.4 weeks (95% CI: 3.3–11.4 weeks). Using a schedule of 5 consecutive days every 3 weeks, 54% developed peripheral sensory neuropathy and only 4% a grade 3, with a median time to development of neuropathy of 108 days (range: 42–189 days).
The lower incidence of this complication may be related to the administration schedule, or to the population enrolled in this study.
The neuropathy related to ixabepilone treatment is typically described as sensory manifestations (i.e., dysesthesias, paresthesias, involving hands and feet) but neuropathic pain has also been reported, although less frequently (grade 3/4 related in 3% of 439 patients treated across all Phase II trials). Motor and autonomic neuropathy has only been reported as a related grade 3/4 event in less than 1% of all patients; they were not described in the absence of sensory or painful neuropathy.
The characteristics and incidence of grade 3/4 neuropathy were similar to those reported in trials of other tubulin-targeting agents, in which incidences ranged from 2 to 32% [22–25]. This neuropathy appears to be somewhat different from that caused by taxanes and the recovery from ixabepilone-induced neuropathy may be more rapid.
The diluent (cremophor) used with ixabepilone has the potential for inducing a hypersensitivity reaction. In clinical trials, anaphylaxis and severe hypersensitivity reactions occurred in less than 1% of patients. Nevertheless, routine premedication, including H1 and H2 antihistamines (not corticosteroids), must be instituted.
Hematological events, consisting primarily of neutropenia and leukopenia, were manageable and did not contribute noticeably to dose reductions or discontinuations. Grade 3 or 4 neutropenia was observed in 54% of patients; however, febrile neutropenia and infection were uncommon.
Phase III trials
The results of early Phase II trials motivated further randomized studies in patients pretreated with or resistant to anthracyclines and resistant to taxanes. Since the combination of ixabepilone and capecitabine allowed a complimentary mechanism of action and nonoverlapping toxicity profiles, this association helped develop the design of randomized studies. Anthracyclines and taxane resistance was defined as tumor progression during treatment or within 4 months of last dose in a metastatic setting, or recurrence within 12 months in the neoadjuvant or adjuvant setting. The recommended doses resulting from the Phase I/II study are ixabepilone 40 mg/m2 (3-h infusion on day 1 every 21 days) and capecitabine 2000 mg/m2 (twice-daily divided doses on day 1 through 14 every 21 days) [26]. This association was studied in two randomized Phase III trials comparing capecitabine alone versus ixabepilone and capecitabine in patients with MBC.
Rare studies had demonstrated a progressionfree survival (PFS) benefit in patients with MBC with a therapy given beyond first-line treatment. The addition of ixabepilone to the antineoplastic agent capecitabine resulted in superior rates of PFS and response compared with capecitabine alone, according to results of these two large Phase III trials with more than 2000 patients in the setting of metastatic or locally advanced breast cancer
Comparison between the Phase III trials of ixabepilone in metastatic breast cancer.

HR: Hazard ratio; ORR: Overall response rate; OS: Overall survival; PFS: Progression-free survival.
The pivotal CA163–046 trial randomized 752 patients who were determined to have resistance to previous anthracycline and taxane therapy using strict resistance criteria [27]. The confirmatory CA163–048 trial randomized 1221 patients who were either pretreated with or resistant to an anthracycline and a taxane [28]. Baseline characteristics were essentially comparable between these trials, except that half of the patients enrolled in CA163–046 were resistant to prior therapy, while nearly all patients in CA163–048 were resistant. Both trials were identically designed and randomized patients to treatment with ixabepilone plus capecitabine or capecitabine monotherapy. The primary study end points were PFS in the first and overall survival (OS) in the second trial. Secondary end points included ORR and safety.
In both studies, the combination arm produced a prolonged median PFS compared with the monotherapy. Median PFS in CA163–046 was 5.7 (95% CI: 4.8–6.7 months) and 4.1 months (95% CI: 3.1–4.3 months), respectively. The hazard ratio (HR) of 0.69 (95% CI: 0.58–0.83; p < 0.0001), indicated a 31% reduction in the risk of disease progression [29]. In CA163–048 it was 6.2 and 4.4 months (p = 0.0005) and the HR was 0.79 (p = 0.0005), which indicated a 21% reduction in the risk of progression.
Superior ORRs were achieved by the combination arm compared with the capecitabine arm. In the CA163–046 trial, the ORR was 42 versus 23%, respectively, while in the CA163–048 trial the ORR was 43 versus 29%, respectively. Although a trend towards a superior OS was noted in the combination arms of both trials, neither reached statistical significance. Nevertheless, the median OS for the ixabepilone plus capecitabine arm versus capecitabine alone in the CA163–046 study was 12.9 versus 11.1 months, respectively (HR: 0.90; 95% CI: 0.77–1.05; p = 0.1936), and in the CA163–048 study it was 16.4 versus 15.6 months, respectively (HR: 0.90; 95% CI: 0.78–1.03; p = 0.1162).
An additional analysis of PFS in prespecified subsets of patients from the confirmatory CA163–048 trial found a clinically meaningful increase in PFS with ixabepilone in patients with triple-negative disease (TND; estrogen and progesterone receptor, human epidermal receptor 2). The increase of PFS reached 25%, the HR was 0.75 and p = 0.0003 with a median PFS within this subgroup of 4.1 months in the combination arm versus 2.1 months in the monotherapy arm. These results indicate that ixabepilone has significant clinical activity in taxane-resistant MBC, both in patients with TND and in the overall population [30,31]. This result was confirmed in a pooled analysis that provides the largest clinical data set recorded for patients with TND in MBC (n = 398). The combination prolonged the median PFS by 2.5 months, caused a 37% reduction in the risk of disease progression and doubled the OR, but did not significantly increase OS, compared with capecitabine alone [32].
The addition of ixabepilone to capecitabine resulted in an increased incidence of hematological toxicities, and consisted primarily of leukopenia and neutropenia, with 5% febrile neutropenia. Anemia and thrombocytopenia were generally grade 1–2 in both treatment groups. Peripheral neuropathy was common, primarily sensory, grade 1 and 2, cumulative, and generally reversible and occurred in 65% of patients receiving both drugs. The most frequently reported grade 3–4 adverse events in the combination group were peripheral sensory neuropathy (21%), fatigue (9%), myalgia (8%) and asthenia (8%). The incidence of diarrhea and hand–foot syndrome was similar in the capecitabine and combination arm.
The investigators concluded that addition of ixabepilone to capecitabine resulted in clinically meaningful efficacy, shown by superior improvements in both PFS and ORR. The results of those randomized studies formed the basis of the approval for routine use in the USA by the FDA and are under evaluation by the EMEA for European approval.
Ongoing studies with ixabepilone in breast cancer
Ixabepilone was and will be assessed in early disease. A neoadjuvant trial with ixabepilone 40 mg/m2 was performed in patients with a primary breast cancer larger than 3 cm. A total of 161 patients were treated [33]. A pathological complete response (pCR) in the breast was achieved in 18% of patients. This study allowed a search for predictive factors for response or resistance and several analyses are ongoing. Interestingly, a subanalysis pointed out an encouraging level of activity in the subgroup of patients with an estrogen-receptor-negative status (47% of patients). Among these patients, 29% achieved a pCR in the breast. Currently, two studies are recruiting patients with early breast cancer. The pivotal CA163–100 trial will evaluate the effectiveness of ixabepilone versus paclitaxel administered after doxorubicine plus cyclophosphamide. A Phase III trial sponsored by the Federation Nationale des Centres de Lutte Contre le Cancer in France, will compare a sequential regimen associating FEC100 and ixabepilone versus FEC100 and docetaxel in adjuvant treatment for poor prognosis breast cancer (triple-negative or HER2- and PR-negative tumor).
In patients with metastatic HER2-positive tumors, one Phase II study is currently evaluating the combination of ixabepilone and trastuzumab, a second trial is assessing the association of carboplatin–ixabepilone and trastuzumab. The trial CA 163–140, is a randomized Phase II study, evaluating ixabepilone plus trastuzumab versus docetaxel plus trastuzumab as a first-line treatment.
Ixabepilone is being assessed in association with bevacizumab versus paclitaxel–bevacizumab in a randomized Phase II study in first-line treatment for metastatic disease with HER2-negative tumors. In this trial, two schedules of ixabepilone administration were studied: the standard 40 mg/m2 at a 3-h infusion every 3 weeks versus 16 mg/m2 at a 1-h infusion given for 3 consecutive weeks followed by 1 week of rest [101].
Combinations of ixabepilone with cetuximab are also under clinical evaluation in patients with triple-negative locally advanced or metastatic breast cancer.
Future perspective
Resistance represents a major obstacle to successful cancer treatment and therefore the development of an agent that avoids key mechanisms of resistance is a welcome advance. Ixabepilone's activity in clinical studies is consistent with its preclinical profile where activity is evident in various chemotherapy-resistant models with multidrug resistance, MRP overexpression and tubulin mutations, and is a novel, very promising antineoplastic agent with activity in tumors resistant to multiple drugs. Several Phase II clinical studies have demonstrated that ixabepilone is active in taxane-resistant non-small-cell lung cancer, hormone-refractory prostate cancer, and certain chemoresistant tumors including gastric, renal and pancreatic carcinomas. In MBC, the Phase II and III studies have provided robust evidence of the activity of ixabepilone in such patients. It seems highly probable that ixabepilone will become a key agent in the treatment of breast cancer at various disease stages and it can be expected to demonstrate a benefit in various other tumor types and settings. Further studies will be performed to demonstrate its potential in other patient settings.
Executive summary
Ixabepilone constitutes a new class of non-taxane tubuline-binding agents.
Ixabepilone has a low susceptibility to major well-known mechanisms of tumor resistance to taxanes, including changes in tubulin isotypes, tubulin mutations and resistance to P-glycoprotein or multidrug resistance protein.
Ixabepilone and capecitabine demonstrated clinically meaningful efficacy, shown by superior improvements in both progression-free survival and overall response rate in patients with a previous exposure to taxanes and anthracyclines in a metastatic breast cancer setting.
Promising activity exhibited by ixabepilone plus capecitabine warrants future studies to establish ixabepilone as the preferred treatment option for patients with triple-negative disease breast cancer.
Peripheral neuropathy is primarily sensory, cumulative and generally reversible.
Footnotes
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.