
Abstract
The reduced capacity of older skin to synthesize vitamin D3 under the influence of ultraviolet light makes older persons at risk of vitamin D deficiency. The risk could even be increased in institutionalized persons owing to their lower sunshine exposure. It has been reported that an inadequate vitamin D level is associated with secondary hyperparathyroidism, increased bone turnover, and bone loss, which increase fracture risk. The objective of this study was to assess the prevalence of inadequate serum vitamin D levels in institutionalized, postmenopausal, osteoporotic women. Assessment of 25-hydroxyvitamin D [25(OH)D] was performed in 445 institutionalized, osteoporotic women from nine countries (Australia, Belgium, France, Germany, Hungary, Italy, Poland, Spain and UK). For each institutionalized woman, three age-matched, noninstitutionalized, osteoporotic controls were also included. Four cutoffs of 25(OH)D inadequacy were fixed: less than 80, less than 75, less than 50 and less than 30 nmol/l. Mean age was 79.7 years (standard deviation [SD] = 5.8) for the institutionalized women and 79.5 years (SD = 5.5) for the noninstitutionalized women (p = 0.45). Significantly fewer institutionalized women received vitamin D supplements (13.2 vs 24.0%; p < 0.0001). In women without vitamin D supplements, the level of 25(OH)D was significantly lower in institutionalized women (56.9 [SD = 23.9] nmol/l) compared with noninstitutionalized women (63.2 [SD = 22.0] nmol/l; p < 0.0001). In institutionalized women (without vitamin D supplements), the prevalence of 25(OH)D inadequacy was 10.4, 41.2, 80.3 and 84.2% when considering cutoffs of 80, 75, 50 and 30 nmol/l, respectively. In the control group, the prevalence was 2.7, 22.9, 74.4 and 81.7%, respectively. The prevalence of vitamin D inadequacy was significantly higher in institutionalized women when considering the 75, 50 and 30 nmol/l cutoffs but not when considering the 80 nmol/l cutoff. This study highlights a high prevalence of vitamin D inadequacy in institutionalized, osteoporotic women. Compared with age-matched osteoporotic controls, the prevalence of severe vitamin D inadequacy was substantially more important in institutionalized women. We believe that a greater awareness of the importance of vitamin D inadequacy is needed in order to address this public health problem.
It is well known that an inadequate vitamin D level is associated with secondary hyperparathyroidism, increased bone turnover, and bone loss, which increase fracture risk. Vitamin D inadequacy has also been implicated as a contributing factor to muscle weakness and falls [1,2]. Moreover, a positive relationship has been demonstrated between cognitive functioning and vitamin D level, which may also influence the risk of falls and fracture [3]. Consequently, osteoporosis prevention and treatment guidelines developed by scientific authorities [4–7] contain recommendations for maintaining an adequate vitamin D level.
Natural sources of vitamin D are limited and include diet and production by photoactivation in the skin. However, the ability of the gut to absorb cholecalciferol has been demonstrated to decrease with age [8]. Vitamin D deficiency is therefore to be expected in the elderly [9–11].
Elderly nursing home residents have a high risk of falls and fracture [12]. Fall-related fracture and injury is a serious problem affecting the quality of life and cost of care for these elderly nursing home residents. Approximately 50% of nursing home residents fall at least once each year [13]. Interestingly, in a study by Snijder et al., it has been shown that poor vitamin D status was associated with an increased risk of falling in the elderly, independently of age, sex, education level, region, season, physical activity, smoking and alcohol intake [14].
Consequently, a very low level of vitamin D should be expected in elderly, institutionalized persons. However, very few studies have compared the prevalence of vitamin D inadequacy in institutionalized and noninstitutionalized patients.
The objective of this study is to assess the prevalence of inadequate serum vitamin D levels in institutionalized, postmenopausal, European osteoporotic women, and to compare it with the prevalence reached in community-dwelling, osteoporotic women, in a case–control study matched for age of the patients. Since vitamin D supplementation has been shown to increase the level of vitamin D, we will also perform analyses restricted to the women without supplementation.
Material & methods
Institutionalized, osteoporotic women from nine countries (Australia, Belgium, France, Germany, Hungary, Italy, Poland, Spain and the UK) were included in this study. These women were part of a run-in study aimed at normalizing the calcium and vitamin D status of patients prior to being included in a trial investigating the antifracture efficacy of a new antiosteoporotic drug. Patients were considered to be osteoporotic if their lumbar spine or femoral neck bone mineral density T-score was equal to or less than −2.5 according to the centralized normative data. For each institutionalized woman, three age-matched noninstitutionalized controls were also included. These women were also part of the run-in study. Consequently, they were also osteoporotic.
Assessment of 25-hydroxyvitamin D [25(OH)D] was performed with a commercial radioimmunoassay (DiaSorin, Italy). It consists of a two-step procedure. In the first step the 25(OH)D and other hydroxylated metabolites are rapidly extracted from serum or plasma with acetonitrile. The extract is then assayed by radioimmunoassay using a polyclonal antibody with specificity to 25(OH)D. The sample, the antibody and the tracer are incubated for 90 min at room temperature (20–25°C). The antigen–antibody complexes are separated after 20 min incubation at room temperature with a second antibody-precipitating complex. This radioimmunoassay is a competitive binding assay with a detection limit of 4 ng/ml and within and between assay precision lower than 8%.
There is no clear international agreement on what should constitute a diagnostic serum level of vitamin D deficiency. Recent publications suggest that circulating levels of 25(OH) D should be between 50 nmol/l (~20 ng/ml) and 80 nmol/l (~32 ng/ml) [15], or at least 80 nmol/l [16]. Indeed, it has been demonstrated that calcium absorption is reduced in patients with vitamin D levels below 80 nmol/l [17]. In this particular study, three cutoffs of 25(OH)D inadequacy were fixed: less than 80 nmol/l, less than 50 nmol/l and less than 30 nmol/l. However, we also used the threshold of 75 nmol/l that has been reached by a consensus expert panel [15].
Normality of variables has been confirmed by Kolmogorov-Smirnov tests. Student T tests or nonparametric tests were used to compare baseline characteristics of the institutionalized and noninstitutionalized groups. Student T tests were used to compare mean values of serum 25(OH)D in women with and without vitamin D supplement. A chi-square test was used to compare the proportion of vitamin D inadequacy between groups. The analysis of variance was performed to compare mean values of serum 25(OH)D according to the seasons. All the data were analyzed using STATISTICA (version7.1; StatSoft Inc., OK, USA). p-values of less than 0.05 were regarded as significant.
Results
A total of 445 institutionalized, osteoporotic women and 1335 noninstitutionalized, osteoporotic women were included in this study. Baseline characteristics of the study population are presented in
Baseline characteristics of the study population.
The level of 25(OH)D was 58.2 (SD = 24.0) and 65.4 (SD = 22.8) nmol/l in the institutionalized and noninstitutionalized groups, respectively (p < 0.001 between the two groups). Moreover, significantly less institutionalized women received vitamin D supplements (13.2 vs 24.0%; p < 0.0001).
In institutionalized women, regardless of the vitamin D supplementation, the prevalence of 25(OH)D inadequacy was 9.6, 38.8, 77.5 and 82.5% when considering cutoffs of 80, 75, 50 and 30 nmol/l, respectively.
In women without vitamin D supplements, the level of 25(OH)D was significantly lower in institutionalized women (56.9 [SD = 23.9] nmol/l) compared with noninstitutionalized women (63.2 [SD = 22.0] nmol/l; p < 0.0001).
In institutionalized women without vitamin D supplementation, the prevalence of 25(OH)D inadequacy was 10.4, 41.2, 80.3 and 84.2% when considering cutoffs of 80, 75, 50 and 30 nmol/l, respectively (
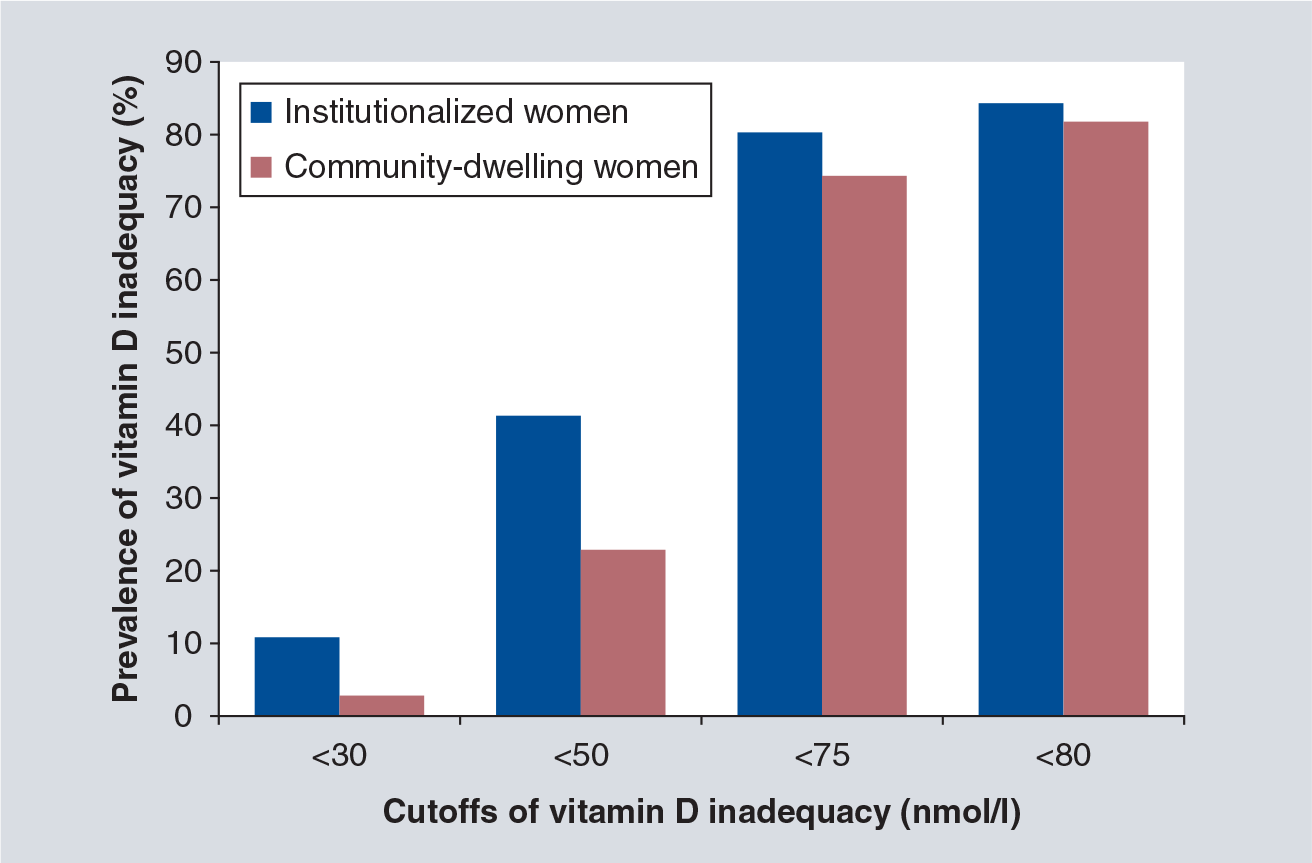
Prevalence of vitamin D inadequacy stratified for various cutoffs.
In institutionalized women (without vitamin D supplementation) we have not found a statistically significant difference in 25(OH) D level across seasons (p = 0.27). The level was 56.8 (SD = 23.9) in spring, 63.7 (SD = 27.6) in summer, 57.8 (SD = 26.1) in autumn and 54.3 (SD = 21.1) in winter. In noninstitutionalized women, the level was 65.9 (SD = 18.7), 69.6 (SD =29.6), 61.7 (SD = 24.1) and 61.3 (SD = 20.0), respectively. In institutionalized and noninstitutionalized women, a significant difference was found between winter and summer, with the lowest level in winter and the highest in summer (p < 0.01 between the two seasons).
Discussion
In this study, we confirm the high vitamin D deficiency amongst elderly European, osteoporotic women, regardless of whether a 50, 75 or 80 nmol/l threshold is used to diagnose deficiency. Interestingly, institutionalized women of the same age have the lowest level of vitamin D level compared with community-dwelling women.
Compared with other studies of nursing home residents, our results demonstrated a similar or a slightly lower prevalence of vitamin D inadequacy [18–23]. It should be highlighted that, because of the particular design of this study (i.e., screening visit prior to being included in a randomized, controlled trial), very frail women were excluded from this study. In fact, our study population could not be considered as representative of the general institutionalized population, but more as an institutionalized, osteoporotic population starting a treatment for osteoporosis. Consequently, the real prevalence of vitamin D inadequacy could even be higher, taking into account the poor nutritional status and the lower sunshine exposure of very frail, institutionalized women [24].
In our study, we have shown a small difference in the vitamin D level between different seasons of sampling but with, a significant difference between two seasons, the lowest being observed during the winter months and the highest during the summer months. These findings are in accordance with previous studies and especially with the recent systematic review investigating vitamin D inadequacy in postmenopausal women [11], and with our previous large cohort study [25] but not with our study performed in a Belgian population [26]. However, in the present study, it should be noted that the vitamin D level was low, even during the summer months.
All these results suggest that vitamin D level should be increased both in institutionalized and community-dwelling elderly women. In a nursing home, the education of healthcare workers about simple interventions that could improve nutritional status [24] or sunlight exposure, and, consequently, vitamin D status, could be of great benefit. If these natural sources of vitamin D do not provide an adequate 25(OH)D level, supplementation with vitamin D could be useful [20,27]. One meta-analysis (including elderly nursing home residents) has shown a 22% reduction in falls with vitamin D supplementation [28]; however, it should be pointed out that the exact role of vitamin D supplementation in fracture prevention is still debated [6,7, 29–35]. At least, it should be highlighted that vitamin D repletion appears to be a prerequisite for maximizing the response to antiosteoporotic treatment, in terms of both bone mineral density changes and antifracture efficacy [36–38].
In our study population, few women were supplemented with vitamin D (13.2 and 24.0% in institutionalized and noninstitutionalized women, respectively). These results are in accordance with the study of Suominen et al., who found that among 2114 residents of nursing homes in Finland, only 21.3% received vitamin D in the therapeutic dose of 10 mg (400 IU) or more, and 3.6% in the recommended dose of 20 mg (800 IU) or more [39]. We should acknowledge, as a limitation of our study, that the doses and the compliance of vitamin D supplementation were not assessed.
Owing to the huge variability in the number of patients included in each country (ranging from 10 to 228 women), no comparison between countries could have been made. This is a weakness in this study, because it has been suggested that vitamin D status depends upon geographic location relative to the equator, with improved vitamin D status in residents closer to the equator compared with those living at higher latitudes.
In conclusion, this study highlights a high level of vitamin D inadequacy in elderly osteoporotic women that could even be higher among institutionalized women. We believe that a greater awareness of the importance of vitamin D inadequacy is needed in order to address this public health problem.
Future perspective
Future studies will need to assess the impact of this high rate of vitamin D inadequacy over the long term.
The impact of modified sunlight exposure or adapted diet needs to be investigated in institutionalized women.
The effect of vitamin D supplementation on the level of 25(OH)D level needs to be investigated in the elderly population. The compliance to these supplement also needs to be studied.
Executive summary
The reduced capacity of older skin to synthesize vitamin D3 and poor nutritional status makes older, institutionalized persons at risk of vitamin D deficiency.
Institutionalized, osteoporotic women from nine countries (Australia, Belgium, France, Germany, Hungary, Italy, Poland, Spain and the UK) were included in this study.
For each institutionalized woman, three age-matched noninstitutionalized controls were also included.
Four cutoffs of vitamin D (25OHD) inadequacy were fixed: less than 80, less than 75, less than 50 and less than 30 nmol/l.
Significantly fewer institutionalized women received vitamin D supplements
In institutionalized women without vitamin D supplementation, the prevalence of vitamin D inadequacy was 10.4, 41.2, 80.3 and 84.2% when considering cutoffs of 80, 75, 50 and 30 nmol/l, respectively.
A greater awareness of the importance of vitamin D inadequacy is needed in order to address this public health problem.
Footnotes
Acknowledgement
The authors thank SERVIER for providing access to the database.
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.