
Abstract
In the Mayo Clinic Cohort Study of Oophorectomy and Aging, women who had both ovaries removed before reaching natural menopause experienced a long-term increased risk of parkinsonism, cognitive impairment or dementia, and depressive and anxiety symptoms. Here, we discuss five possible mechanistic interpretations of the observed associations; first, the associations may be non-causal because they result from the confounding effect of genetic variants or of other risk factors; second, the associations may be mediated by an abrupt reduction in levels of circulating estrogen; third, the associations may be mediated by an abrupt reduction in levels of circulating progesterone or testosterone; fourth, the associations may be mediated by an increased release of gonadotropins by the pituitary gland; and fifth, genetic variants may modify the hormonal effects of bilateral oophorectomy through simple or more complex interactions. Results from other studies are cited as evidence for or against each possible mechanism. These putative causal mechanisms are probably intertwined, and their clarification is a research priority.
Keywords
Public health significance of bilateral oophorectomy
Every year, approximately 300,000 women face the decision to undergo prophylactic bilateral oophorectomy in conjunction with hysterectomy [1]. The practice of prophylactic bilateral oophorectomy has increased over time, more than doubling between 1965 and 1999 [2], but the risk–benefit balance of prophylactic oophorectomy versus ovarian preservation remains uncertain and controversial [1,3–7]. Based on a study of the incidence of oophorectomy in Olmsted County, MN, USA, we project that an additional 300,000 US women undergo bilateral oophorectomy for a benign ovarian condition every year [8]. In total, approximately 600,000 women undergo bilateral oophorectomy in the USA every year, many before reaching natural menopause. For all of these women, it remains unknown whether, and for how long, estrogen treatment is needed, or whether other hormonal replacement treatments are needed [6].
We previously reported from the Mayo Clinic Cohort Study of Oophorectomy and Aging that women who underwent early bilateral oophorectomy before the onset of menopause have an increased overall mortality, as well as increased mortality associated with cardiovascular diseases and with neurological or psychiatric diseases, compared with referent women [3,9]. In addition, we reported that those women have an increased risk of parkinsonism, cognitive impairment or dementia, and depressive and anxiety symptoms compared with referent women (see executive summary) [7,10–13]. In this paper, we propose several possible mechanistic interpretations of the observed associations with aging-related neurological diseases, and we discuss their clinical and research implications. Results from other studies are cited as evidence for or against each possible mechanism.
The Mayo Clinic Cohort Study of Oophorectomy & Aging
We conducted a historical cohort study among all women residing in Olmsted County, MN, who underwent unilateral or bilateral oophorectomy before the onset of menopause for a non-cancer indication from 1950 through 1987. Each member of the oophorectomy cohort was matched by age to a referent woman from the same population who had not undergone oophorectomy. In total, we studied 1252 women with unilateral oophorectomy, 1075 women with bilateral oophorectomy and 2368 referent women. Women were followed for a median of 25–30 years. Parkinsonism was assessed using screening and examination, through a medical records-linkage system, and through death certificates. By contrast, cognitive status or dementia, and depressive or anxiety symptoms were assessed using a structured questionnaire via a direct or proxy telephone interview. Our results are summarized in the executive summary and were reported in detail elsewhere [3,7,9–13]. In this paper, we limit our discussion to the findings related to bilateral oophorectomy.
Endocrine consequences of early bilateral oophorectomy
The ovary is the primary source of estrogen and progesterone during reproductive life. In addition, the ovary produces testosterone both before and after menopause. This may be particularly important because testosterone is aromatized peripherally into estrone, the major circulating estrogen after menopause [1,14,15], and into estradiol, the most potent estrogen, in widespread tissues and organs including the brain [16–18].
The hormonal changes induced by premenopausal bilateral oophorectomy are different from those occurring during natural menopause or those induced by postmenopausal bilateral oophorectomy. In particular, bilateral oophorectomy may occur at ages much younger than the natural menopause (median age of approximately 50 years) [19], and the resulting hormonal changes are abrupt. By contrast, the endocrine changes of natural menopause result from a progressive decline in ovarian function. Although hormone levels and menstrual cycles are quite irregular and unpredictable during the menopausal transition, the underlying physiologic process is a progressive decrease in ovarian follicle numbers [20,21]. Bilateral oophorectomy before menopause results not only in an abrupt drop in levels of circulating estrogen but also an abrupt drop in levels of circulating progesterone and testosterone and in a disruption of the hypothalamic–pituitary–ovarian axis [22]. Disruption of this axis is associated, in turn, with an increased release of the gonadotropins luteinizing hormone (LH) and follicle stimulating hormone (FSH) by the pituitary gland. By contrast, if the ovaries are removed long after a woman has experienced natural menopause, the hormonal changes related to estrogen, progesterone and gonadotropins may be less dramatic because estrogen and progesterone levels are already naturally reduced. However, the postoperative drop in testosterone levels is abrupt and may have clinical consequences [15].
It is uncertain to what extent the harmful effects of premenopausal bilateral oophorectomy are uniquely mediated by estrogen deficiency, or whether other mechanisms are involved [22–26]. Indeed, in the Mayo Clinic Cohort Study of Oophorectomy and Aging, estrogen treatment until 50 years of age in women with early bilateral oophorectomy did not offset the increased risks of parkinsonism, anxiety symptoms or depressive symptoms [11,13]. However, estrogen treatment up to age 50 years did offset the increased risk of overall mortality, of cardiovascular mortality, and of cognitive impairment and dementia (see executive summary) [3,9,10]. Thus, we need new mechanistic hypotheses and new research to address these unresolved issues.
Possible mechanisms linking bilateral oophorectomy with aging-related neurological diseases
In
First possible mechanistic explanation of the associations between bilateral oophorectomy and brain outcomes.
We then discuss four possible direct causal mechanisms that may act in isolation or in combination because they are not mutually exclusive (

Second, third and fourth possible mechanistic explanations of the associations between bilateral oophorectomy and brain outcomes.

Fifth possible mechanistic explanation of the associations between bilateral oophorectomy and brain outcomes.
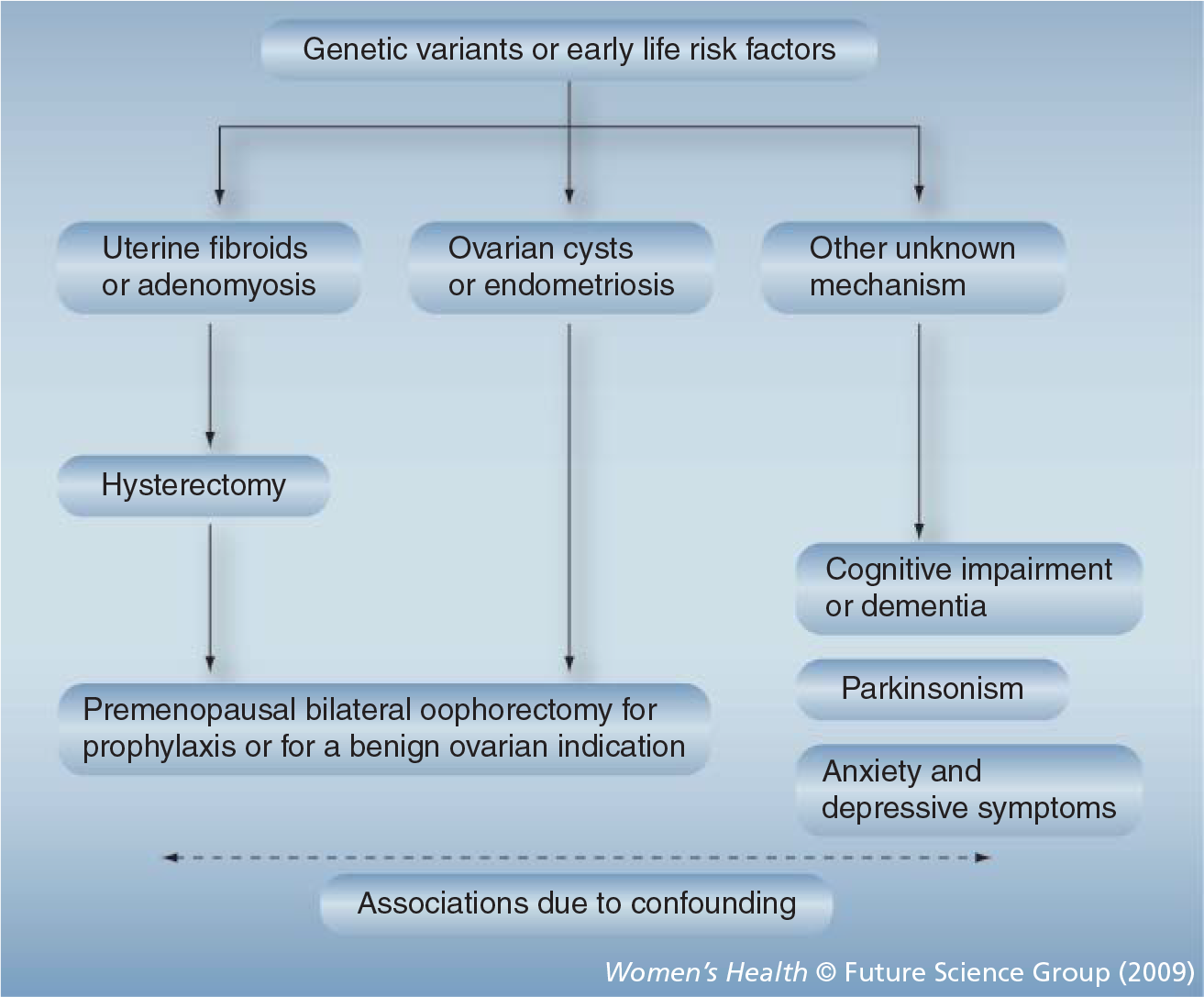
First mechanism: confounding by genetic variants or by early life risk factors
Under this hypothetical mechanism, the association between bilateral oophorectomy performed before the onset of menopause and aging-related neurological diseases is due to susceptibility genes that increase the risk of both outcomes independently (i.e., confounding by genetic predisposition;
In support of this hypothesis, there is evidence that genetic factors predispose women to hysterectomy. A twin study demonstrated 63% heritability for age at natural menopause and 59% heritability for hysterectomy prior to natural menopause. In addition, the heritability of the two major indications for hysterectomy was also high: 69% for fibroids and 55% for menorrhagia [27]. Heritability is probably due to the transmission of genetic variants. Indeed, another study demonstrated that women with a variant in the estrogen receptor 1 gene (ESR1; single nucleotide polymorphism [SNP] rs2234693) have an increased risk of surgical menopause [28]. Therefore, genetic variants could determine uterine diseases that prompt hysterectomy, in turn, prompting prophylactic bilateral oophorectomy. By contrast, the evidence for an association between genetic variants and ovarian cysts or endometriosis remains limited [29–31], and the contribution of genetic factors to the risk of benign ovarian conditions that may prompt bilateral oophorectomy remains unknown.
For the genetic variants to act as a confounder, they must be associated not only with the oophorectomy but also with the aging-related neurological diseases [32]. However, the evidence linking certain variants of the genes in the estrogen synthesis and responsiveness pathway with the risk of dementia, parkinsonism or depressive and anxiety symptoms remains limited [33–37]. For example, in the first genome-wide association study of Parkinson's disease involving a mixed sample of men and women, we found 11 SNPs associated with Parkinson's diseases. Of those SNPs, one was in the PR domain-containing protein 2 gene (PRDM2), which encodes an estrogen receptor coactivator protein [36]. In addition, we reanalyzed our data considering only women (172 cases; 229 controls), and found several additional associations with genetic variants in the ESR1, estrogen receptor 2 (ESR2) and PRDM2 genes [34]. However, these initial findings await replication.
Alternatively, confounding could be caused by another nongenetic risk factor. We can postulate that some early life events, such as the use or non-use of oral contraceptives, or the number and outcome of pregnancies, may predispose women to uterine or ovarian diseases leading to bilateral oophorectomy, and may independently predispose women to aging-related neurological diseases. Once again, in this case, bilateral oophorectomy would be only a marker of risk. However, we are not aware of any evidence in support of this hypothesis.
Against a confounding effect is our observation of a similar risk of neurological diseases among women who underwent bilateral oophorectomy for benign conditions or for prophylaxis of ovarian cancer, because these findings suggest that the risk of neurological diseases was independent of the indication for the oophorectomy. By contrast, if confounding was present, we would expect a variation in risk across indications. Although the possibility that confounding is the explanation of the observed associations cannot be completely ruled out at this time, the evidence for a confounding mechanism is limited. Thus, we propose three potential causal mechanisms involving the hormonal changes induced by bilateral oophorectomy. In addition, we propose one mechanism combining hormonal changes with underlying genetic factors.
Second mechanism: chain of causality prompted by decreased levels of circulating estrogen
Under this hypothetical mechanism, the abrupt reduction in circulating estrogen caused by bilateral oophorectomy is the initial step in a chain of causality leading to aging-related neurological diseases (
The hypothesis of a neuroprotective effect of estrogen is corroborated by several observational studies that demonstrated a reduced risk of dementia in women treated with estrogen started early in menopause compared with women not treated [38–42]. By contrast, the Women's Health Initiative (WHI) clinical trials demonstrated an increased risk of cognitive impairment or dementia in women aged between 67 and 79 years treated with estrogen alone or in combination [43–46]. To reconcile the contrasting findings from observational studies and from clinical trials, it has been suggested that the effects of estrogen on the brain may vary with age (‘timing hypothesi' or ‘window of opportunity hypothesi’) [12,42,47–50]. However, several important questions remain unanswered about this hypothesis.
Third mechanism: chain of causality prompted by decreased levels of circulating progesterone or testosterone
Under this hypothetical mechanism, the abrupt reduction in circulating progesterone or testosterone caused by bilateral oophorectomy is the initial step in a chain of causality leading to aging-related neurological diseases (
The hypothesis of a neuroprotective effect of progesterone and testosterone is corroborated by several laboratory and clinical studies [23,25,26,44,51,52]. However, there is some contrasting evidence that progesterone could have harmful effects on the aging brain [53,54]. Further research is needed to clarify these issues.
Fourth mechanism: chain of causality prompted by increased release of gonadotropins
Under this hypothetical mechanism, the abrupt reduction in circulating estrogen and progesterone caused by bilateral oophorectomy prompts a disruption of the hypothalamus–pituitary–ovarian axis resulting in increased release of the gonadotropins LH and FSH by the pituitary gland. The increased release of gonadotropins is then the initial step in a chain of causality leading to aging-related neurological diseases (
This hypothesis is supported by the protective effect of estrogen therapy (which lowers gonadotropin levels) on symptoms of dementia, but is refuted by the failure of estrogen treatment to offset the increased risk of parkinsonism and of depressive and anxiety symptoms in the Mayo Clinic Cohort Study of Oophorectomy and Aging [11,13]. However, the analyses stratified by estrogen treatment were based on small samples, and the evidence is insufficient to fully understand the possible protective effects of estrogen mediated by the modulation of gonadotropin levels.
The hypothesis of a harmful effect of LH on the brain is corroborated by several laboratory and clinical studies [22,24,55,56]. For example, a study in a transgenic mouse model of Alzheimer's disease demonstrated that drugs blocking the release of LH significantly attenuated cognitive decline and decreased β-amyloid deposition in treated animals compared with placebo-treated animals [57]. However, more clinical and epidemiologic research is needed to clarify the effects of LH and FSH on the brain.
Fifth mechanism: interactions between genetic variants, nongenetic factors & oophorectomy
Some genetic variants may modify the effect of bilateral oophorectomy on the brain causing a synergistic or an antagonistic joint effect (
It has been hypothesized that apolipoprotein E (apoE; the protein coded by the APOE gene) may be a critical factor in the neuroprotective actions of estrogen [56,57]. There is increasing evidence from both in vivo (mice) and in vitro studies (cell cultures) that estrogen may modulate the apoE protein and its receptor, namely, the low density lipoprotein receptor-related protein [60,61]. Results from numerous laboratory studies have demonstrated that:
Nerve regeneration is severely delayed in APOE-knockout mice as compared with wild-type littermates;
Estrogen replacement in ovariectomized mice resulted in a significant increase in levels of apoE protein and low density lipoprotein receptor-related protein in the olfactory bulb and other brain areas;
Estrogen treatment increased apoE protein and increased neurite outgrowth in cortical and olfactory neuronal cultures;
Estrogen treatment had no effect on neurite outgrowth in cultures deprived of apoE protein or in cultures with the apoE4 protein.
These studies suggest that apoE protein is a critical intermediary for the beneficial effects of estrogen on neuronal protection and repair [61–64]. The hypothesis that the neuroprotective effects of estrogen may be modified by APOE genotype is also supported by some clinical and epidemiologic studies [65–68]; however, none of these studies focused on women with bilateral oophorectomy.
More complex etiologic interactions
The joint effects of oophorectomy and genes may be much more complex than the example provided, and probably involve the interactions of several genes with each other and with hormonal factors. For example, the effect of oophorectomy may be modified jointly by variants of the APOE gene and of the ESR1 gene with multiple levels of synergistic or antagonistic effects [33,66]. In addition, the genetic effects may involve several complex hormonal synthesis and responsiveness pathways rather than individual genes [69]. Genetic effects may also involve epigenetic mechanisms [70,71]. Finally, other nongenetic factors (e.g., smoking and obesity) may modify the effect of oophorectomy and of several genetic variants (
Implications for research & clinical practice
The causal mechanisms discussed here have important implications for clinical practice and for research. If the harmful long-term effects of bilateral oophorectomy on the brain are mediated primarily by decreased circulating levels of estrogen, estrogen replacement may be an adequate and important treatment for women who undergo oophorectomy for benign indications. By contrast, if some of the harmful effects of bilateral oophorectomy on the brain are caused by decreased circulating levels of progesterone or testosterone, additional hormonal treatments may be needed. Finally, if the increased release of LH or FSH is an important factor, drugs targeting gonadotropins may be useful. Our results from the Mayo Clinic Cohort Study of Oophorectomy and Aging suggest that the interplay of hormonal mechanisms may be complex and may vary depending on the specific neurological disease considered.
At present, it remains unknown if and for how long estrogen treatment should be continued, or whether other hormonal treatments are needed for the approximately 600,000 women who undergo bilateral oophorectomy in the USA every year, many before reaching natural menopause [6]. In general, regardless of the causal mechanism, the optimal practice is probably ovarian preservation in the majority of young women not known to be at increased risk of ovarian or breast cancer [1,3–5,7].
From a research perspective, additional clinical studies are needed to explore the specific effects of bilateral oophorectomy on brain aging in women. Although the Mayo Clinic Cohort Study of Oophorectomy and Aging provided new provocative evidence, the findings await replication, and many new questions remain. Studies with a long period of follow-up after oophorectomy are few and insufficient, whereas studies with shorter follow-up may not be adequate to address the questions that remain unanswered. Thus, clinical trials are not likely to address the observed associations because their design is only adequate for testing short-term effects (5–10 years). In addition, the randomization of women to prophylactic bilateral oophorectomy, or the randomization of women who underwent bilateral oophorectomy to estrogen or other hormonal replacement treatment, may raise ethical concerns. In general, the practices of ovarian preservation, oophorectomy and hormone replacement therapy tend to be individualized and the complexity of decision-making precludes a ‘one size fits all’ approach.
In addition, new laboratory and clinical research studies are needed to clarify the hormonal mechanisms and the possible genetic interactions. Studies of the effects of estrogen, progesterone, testosterone, LH and FSH on the brain may provide new strategies for the prevention and treatment of aging-related neurological diseases. However, these hormonal effects may vary greatly with age [12]. For example, estrogen effects on the brain may vary in premenopausal women, during the menopausal transition and after menopause ('timing hypothesi' or ‘window of opportunity hypothesi’) [12,42,47–50].
Future perspective
We are facing a rapid aging of the population worldwide [72]. This rapid aging will dramatically increase the number of people projected to be affected by aging-related neurological diseases. This dramatic trend is well exemplified by the available statistics for dementia in general and Alzheimer's disease in particular. In 2006, the number of people affected by Alzheimer's disease was 26.6 million worldwide and the majority of patients were women. Moreover, it was estimated that $156 billion is spent annually to care for dementia patients worldwide [73]. By 2050, the prevalence is expected to quadruple, so that one in 85 persons will be living with the disease [74], and 43% of them are expected to need a high level of care (e.g., a nursing home).
Although the prevalence of dementia and its associated disability increases exponentially with age [75,76], the focus of research has recently shifted towards younger persons and very early stages of cognitive decline and mild cognitive impairment. The hope is to delay the conversion of cognitive decline and mild cognitive impairment to full dementia. Indeed, if interventions could delay disease onset or progression by as little as 1 year, we would expect nearly 9.2 million fewer Alzheimer's disease patients by the year 2050 [74].
Executive summary
Bilateral oophorectomy performed before the onset of menopause is associated with an increased risk of cognitive impairment or dementia. The association is stronger with younger age at oophorectomy, is independent of the indication for oophorectomy and may be offset by estrogen treatment.
Bilateral oophorectomy performed before the onset of menopause is associated with an increased risk of parkinsonism and Parkinson's disease. The association is stronger with younger age at oophorectomy and is independent of the indication for oophorectomy, but is not offset by estrogen treatment.
Bilateral oophorectomy performed before the onset of menopause is associated with an increased risk of long-term depressive and anxiety symptoms. The association is stronger with younger age at oophorectomy and is independent of the indication for oophorectomy, but is not offset by estrogen treatment.
The associations may be due to a chain of causality prompted by reduced levels of circulating estrogen.
The associations may be due to a chain of causality prompted by reduced levels of circulating progesterone or testosterone.
The associations may be due to a chain of causality prompted by an increased release of gonadotropins by the pituitary gland.
The associations may involve the synergistic or antagonistic interaction of bilateral oophorectomy with genetic variants (e.g., APOE or ESR1 genes). The interactions may be complex and may also involve other nongenetic factors.
The associations listed above need to be confirmed (or challenged) by other studies.
The four causal mechanisms listed above have implications for medical treatment in women who must undergo early bilateral oophorectomy.
Additional laboratory and clinical research is needed to clarify mechanisms and to guide treatment to restore normal physiology when oophorectomy is required.
A better understanding of the long-term sequelae of bilateral oophorectomy and of the effects of ovarian hormones on brain aging may guide the development of interventions to delay disease onset or slow disease progression, leading to a reduced burden of neurological diseases. Thus, we suggest that this is an area of high research priority and of major significance for the health of aging women.
Footnotes
This research was supported by the National Institute of Neurological Disorders and Stroke (grant R01 NS33978) and the National Institute of Arthritis and Musculoskeletal and Skin Diseases (grant R01 AR030582). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed. No writing assistance was utilized in the production of this manuscript.