
Abstract
The incidence of ectopic pregnancies is increasing, which may be related to better diagnostic tools as well as the increasing use of assisted reproductive technologies. However, the signs and symptoms of ectopic pregnancy can be similar to other complications of early pregnancy such as miscarriage. Diagnosis often requires serial human chorionic gonadotropin levels along with ultrasound and, in some cases, dilation and curettage. Once a diagnosis has been made, treatment options include medical therapy with methotrexate and surgery, which can often be performed via the laparoscope. Fertility rates after therapy are similar for both medically and surgically treated patients.
The incidence of ectopic pregnancy is increasing. In 1992, the rate of ectopic pregnancies was 19.7 per 1000 in the USA, which was an increase from 4.5 per 1000 in 1970 [1]. This increase may be associated with an increase in the prevalence of risk factors for ectopic pregnancy such as pelvic infections. Furthermore, we now have more specific and sensitive methods to diagnose ectopic pregnancies, including the use of high-resolution ultrasound. In patients undergoing assisted reproductive technologies, the incidence of ectopic pregnancy is approximately 2% and may also contribute to the increasing incidence of ectopic pregnancy [101].
Maternal mortality secondary to ectopic pregnancy has been decreasing, accounting for 13% of maternal deaths in the time period from 1979 to 1986 and approximately 6% of maternal deaths from 1991 to 1999, with most being secondary to hemorrhage [2].
Risk factors & pathogenesis
Ectopic pregnancy occurs in the fallopian tube in over 95% of cases [3]. Other locations for ectopic pregnancies are rare: abdominal, ovarian or cervical. The most common location in the fallopian tube for ectopic pregnancies to occur is the ampulla (70.0%); other locations, such as the isthmus (12.0%), the fimbria (11.1%) and the cornua (2.4%), are less common (Figure 1). The ampullar portion of the fallopian tube is more distendable than other areas. Ectopic pregnancies in this location may result in tubal abortion and not be recognized clinically. The isthmus of the fallopian tube is not able to expand to accommodate a growing ectopic pregnancy and is more prone to rupture.

Locations of fallopian tube ectopic pregnancy.
Patients with certain risk factors are known to be at higher risk of developing ectopic pregnancy. Patients who have had a previous ectopic pregnancy, who have had previous tubal surgery, who have documented tubal pathology, who have known in utero diethystilbestrol exposure or who are undergoing assisted reproductive technologies are at relatively high risk of developing an ectopic pregnancy if they were to become pregnant. Patients with infertility, previous genital infections including gonorrhea and chlamydia, or who have greater than one lifetime sexual partner are at moderately increased risk [4]. Overall, patients who have an intrauterine device (IUD) or who have had a tubal ligation are at decreased risk of ectopic pregnancy compared with nonpregnant controls. However, if women become pregnant with an IUD in place or after a tubal ligation, they are at increased risk for having an ectopic pregnancy compared with women who conceive without an IUD or tubal ligation (Table 1) [5].
Risk factors for ectopic pregnancy.
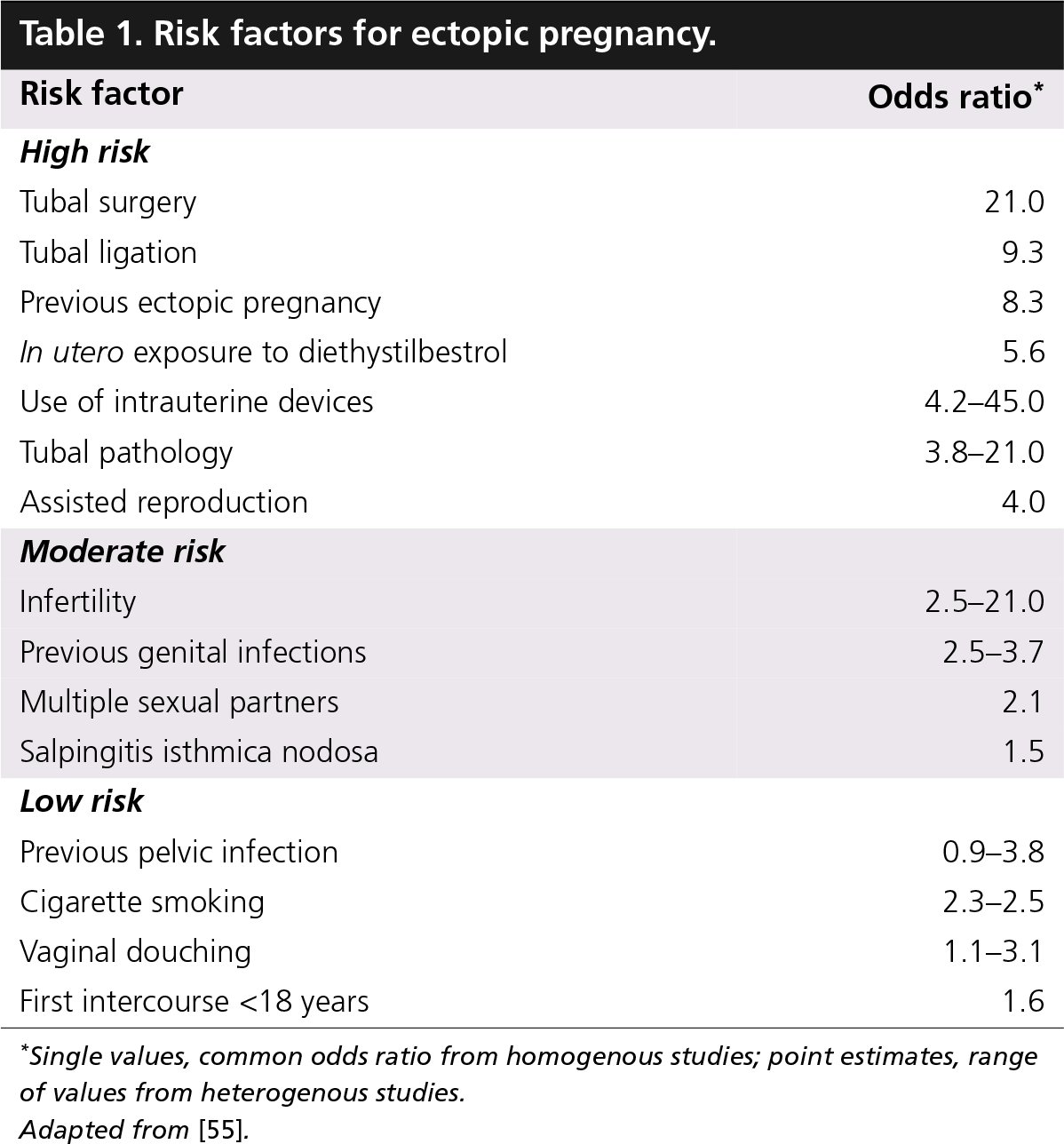
Single values, common odds ratio from homogenous studies; point estimates, range of values from heterogenous studies.
Adapted from [55].
Ectopic pregnancies may occur owing to impaired migration of the fertilized ovum in the fallopian tube, resulting from inflammation, hormonal or other factors. If the passage of the fertilized ovum is slowed and hatching occurs prior to the ovum reaching the endometrial cavity, the embryo may implant in the fallopian tube. Intrinsic factors to the embryo do not seem to contribute to ectopic pregnancy. In a series analyzing the chromosomes of abnormally implanted embryos, no karyotype abnormalities were noted [6,7]. Research is now focusing on the molecular signaling at the time of blastocyst implantation and identifying abnormalities in this event that may further explain the etiology of ectopic gestations [8].
Signs & symptoms
Patients with ectopic pregnancy may present in the first trimester of pregnancy with vaginal bleeding and pelvic pain. These symptoms are neither sensitive nor specific and are also associated with other pregnancy complications, such as miscarriage. Furthermore, patients with an ectopic pregnancy may be asymptomatic. Certain symptoms are suggestive of possible tubal rupture with intra-abdominal hemorrhage and require immediate intervention. These include hypovolemic shock and syncope. Other suggestive findings on physical examination are abdominal tenderness with rebound or guarding. Findings on pelvic examination may be nonspecific and include a tender adnexal mass, which may not been seen in most patients with ectopic pregnancy [9–11].
Diagnosis
The diagnosis of ectopic pregnancy requires differentiating it from a viable intrauterine pregnancy. This is done with the use of β-human chorionic gonadotropin levels (β-hCG), transvaginal ultrasound and, in some cases, uterine curettage. Although progesterone levels are typically higher in intrauterine gestations compared with ectopic gestations and a progesterone level of less than 5 ng/ml can rule out a viable pregnancy, there is not a definitive value that demarcates the two [12]. Therefore, progesterone levels often do not aid in the diagnosis of ectopic pregnancy.
A transvaginal ultrasound can confirm the presence of an intrauterine gestation by 5.5 weeks in almost all cases. However, a gestational sac can be identified on transvaginal ultrasound as early as 4.5–5 weeks gestation and a yolk sac is visible on ultrasound by as early as 5 weeks. A fetal pole with heart motion can be seen by 6 weeks' gestation [13]. However, because patients are not always certain of their last menstrual period, β-HCG levels are often used to determine when an intrauterine gestation should be seen on transvaginal ultrasound. This cutoff level of β-hCG varies by institution but ranges from 1500 to 2500 mIU/ml. Setting a low β-HCG cutoff value increases the sensitivity of ultrasound and β-hCG at diagnosing an ectopic pregnancy but increases the risk of missing a viable intrauterine pregnancy. A higher β-hCG cutoff value is used to maximize specificity, or to ensure a viable intrauterine pregnancy is not missed. If the β-hCG level is below this value at presentation, serial β-hCG levels must be obtained to assess viability.
With the use of radioimmunoassay and specific antiserum to β-hCG, levels can be detected in serum at 1 mIU/ml and in the urine at 20 mIU/ml. This allows for very precise quantification of β-hCG and allows clinicians to accurately follow trends in β-hCG levels. Traditionally, an increase of at least 66% over 2 days would confirm the presence of a normally developing pregnancy [14]. However, more contemporary β-hCG curves have determined that some viable pregnancies have a slightly slower increase in β-hCG levels, with a 99 percentile demonstrated to be a 53% rise in 2 days. This is the expected rate of rise in β-hCG values less than 10,000 mIU/ml. Rare cases of intrauterine gestations have been noted with β-hCG levels increasing 35% in 2 days [15,16]. However, β-hCG levels rise similarly to a normally developing pregnancy in 21% of ectopic pregnancies, so ultrasound remains an important part of the diagnostic work-up when β-hCG levels reach the discriminatory cutoff [17].
In 85% of abnormal pregnancies, there is an abnormal rise in β-hCG levels or a plateau in β-hCG levels. A rapid decline in β-hCG levels, which is defined as a decrease of 21–35% (depending on initial levels) over 2 days, is most indicative of a miscarriage. However, declining β-hCG levels may also be seen in resolving ectopic gestations [17]. It is important to follow weekly β-hCG levels in these patients until they are undetectable. In patients with abnormally rising β-hCG levels, an abnormal intrauterine gestation needs to be differentiated from an ectopic pregnancy.
If β-hCG levels are above the discriminatory cutoff value, an ultrasound should be performed. See the algorithm in

Diagnostic algorithm for ectopic pregnancy.
Ectopic pregnancies can cause the formation of a pseudogestational sac in the endometrium, which is a collection of fluid in the endometrial cavity caused by bleeding from the decidualized endometrium. A pseudogestational sac is centrally located whereas a true gestational sac is often eccentric in location, but the two can be confused on ultrasound. Other ultrasound findings seen with ectopic gestations include a corpus luteum, which is seen on the same side as the ectopic gestation in 70–85% of cases [18,21,22]. In addition, the presence of blood in the pelvis is seen in approximately 30% of ectopic gestations and may be the result of tubal rupture or leakage of blood from the fallopian tube [18].
When a nonviable gestation has been confirmed, but its location has not been determined by ultrasound, a dilation and curettage (D&C) should be performed. Two such situations are when the hCG is above the discriminatory zone and no intrauterine pregnancy (or extrauterine) gestation has been visualized or in the case of abnormally rising β-hCG levels as part of the workup for ectopic pregnancy. In both cases, a histological examination should be performed on the evacuated uterine contents to look for the presence of chorionic villi. If chorionic villi are identified, the diagnosis is an abnormal intrauterine gestation, which is treated by the D&C. If chorionic villi are not present on histological examination, the diagnosis of ectopic pregnancy has been made and treatment should ensue. However, there are cases in which histological examination of the specimen is not readily available or may be unreliable. In these cases, before treatment for an ectopic pregnancy is begun, a quantitative β-hCG should be performed prior to the D&C and a second level should be drawn 12–24 h later. The β-hCG level should decrease by at least 15% in this time if an intrauterine pregnancy was evacuated. In most cases of a nonviable intrauterine pregnancy, the decline is more dramatic. If the β-hCG does not decline after the contents of the uterus have been removed, the diagnosis of an ectopic pregnancy can be made and treated accordingly. Again, it is important to follow weekly β-hCG levels until they are undetectable to confirm resolution of the pregnancy.
Treatment
Medical management
Methotrexate is a folic acid antagonist. It works by inhibiting the synthesis of purines and pyrimides and therefore interfering with DNA synthesis. Methotrexate affects rapidly dividing cells and halts mitosis. In ectopic gestations, it prevents the proliferation of the cytotrophoblasts. This results in decreased trophoblast β-hCG production, which causes decreased secretion of progesterone by the corpus luteum.
In the 1980s, methotrexate was first used to treat ectopic pregnancies. A study by Stovall et al., published in 1989, described outpatient treatment of ectopic pregnancy with methotrexate. In this protocol, a leucovorine ‘rescue’ was used [23]. Leucovorine is folinic acid and allows a higher dose of methotrextate to be used by mitigating some of its side effects. In this protocol, which is known as the multiple-dose methotrexate protocol, methotrexate is given at a dose of 1 mg/kg intramuscularly on days 1, 3, 5 and 7. Leucovorine is given at a dose of 0.1 mg/kg intramuscularly on days 2, 4, 6 and 8. In the multidose protocol, up to four doses of methotrexate are given until β-hCG levels decrease by 15% on two consecutive days
Methotrexate protocols.

For all protocols, after initial decline in β-hCG, check weekly levels until undetectable or, in the multidose protocol, until <15 IU/l.
β-hCG: β-human chorionic gonadotropin; CBC: Complete blood count; LFT: Liver-function tests.
A single-dose protocol was developed subsequently. It was noted in prior studies that giving a single-dose of methotrexate might enhance patient compliance without decreasing effectiveness. Therefore, the protocol came to be known as the single-dose methotrexate protocol, as most patients only receive a single dose of the medication. In this protocol, methotrexate is given at a dose of 50 mg/m2 on day 1. A second dose is given on day 7 if β-hCG values do not decrease by at least 15% between days 4 and 7. β-hCG levels are followed weekly until they are undetectable (see Table 2). An article by Lipscomb et al. reported that 20% of patients undergoing this protocol will require more than one treatment cycle [24]. The mean time to resolution of the ectopic pregnancy was 35 days but could take as long as 109 days. There is no leucovorin rescue used in this protocol. After initial diagnosis, ultrasounds are generally not repeated. The ectopic gestation may actually increase in size after methotrexate treatment, which may be due to hematoma formation.
Prior to giving methotrexate, a complete blood count, liver function tests and creatinine should be checked. In a patient with a history of pulmonary disease, a chest x-ray should be obtained owing to the risk of interstitial pneumonitis with methotrexate therapy. Absolute contraindications to methotrexate therapy are a hemodynamically unstable patient, a patient who is breastfeeding, has immunodeficiency, liver disease or alcoholism, active pulmonary disease, peptic ulcer disease and hematologic, renal or liver dysfunction. Relative contraindications are an ectopic gestation 3.5 cm in size or greater and the presence of fetal heart activity [25]. These contraindications are related to the efficacy of methotrexate as well as its side effects. Methotrexate is generally well tolerated in doses given to treat ectopic pregnancy. High-dose methotrexate has been associated with bone marrow suppression, hepatotoxicity, stomatitis, pulmonary fibrosis, reversible alopecia, photosensitivity and febrile morbidity. The most common side effect is mild elevations of liver transaminases. Patients receiving methotrexate should stop prenatal vitamins or folic acid supplements.
During treatment with methotrexate, β-hCG levels may actually rise or plateau between days 1 and 4 before they start to decrease. This is thought to be due to the syncytiotrophoblasts that continue to produce β-hCG after methotrexate treatment. Another phenomenon seen during treatment with methotrexate is transient abdominal pain, which can occur 3–7 days after the start of therapy and can last for 4–12 h. This can be due to a tubal bleed, the formation of a hematoma or a tubal abortion. It is also important to rule out tubal rupture, which would be an indication for surgical intervention. Clinical indications for surgery are abdominal pain that is severe and persistent beyond 12 h, orthostatic hypotension or decreasing hematocrit values.
Beyond the clinical signs of treatment failure, other signs indicating possible methotrexate failure include an increase or plateau of β-hCG, which occurs after the first week of treatment [25].
The effectiveness of different methotrexate protocols has been investigated. In 12 studies, which included 338 patients who underwent variable-dosing methotrexate therapy, in which therapy was titrated according to β-hCG levels, the success rate of methotrexate therapy was 93% [26]. Furthermore, on follow-up hysterosalpingogram (HSG), fallopian tubal patency was 75%. The subsequent fertility rate was 58% and 7% of patients had a repeat ectopic pregnancy. In 32 studies of 1626 patients undergoing conservative laparoscopic surgery for ectopic pregnancy, both success rates and subsequent fertility rates were similar. This compares with seven studies of 393 patients who underwent the single-dose methotrexate protocol, with 87% having a successful resolution of the ectopic pregnancy. Of these patients, 8% required a second dose of methotrexate. Follow-up HSG demonstrated tubal patency in 81% of patients. Of patients desiring fertility, 61% subsequently had a demonstrated intrauterine pregnancy and 8% had a repeat ectopic pregnancy [26]. This suggests decreased efficacy of the single-dose methotrexate protocol as compared with the multidose protocol, while efficacy of the multidose methotrexate protocol is similar to that of conservative laparscopic surgery.
In another trial of 100 patients comparing methotrexate therapy with laparoscopic salpingostomy, 86% of patients receiving one or two doses of methotrexate were successfully treated. In patients undergoing laparoscopic salpingostomy, 72% were successfully treated with surgery alone and 20% required postoperative methotrexate for persistent trophoblast. Post-treatment tubal patency rates were similar in both medically and surgically treated patients [27]. A study by Dias Pereira et al. looked at fertility outcomes in 74 women desiring pregnancy who had undergone either multidose methotrexate therapy or laparoscopic salpingostomy for ectopic pregnancy and found pregnancy rates at 18 months to be 36 and 43%, respectively [28]. Post-treatment fertility rates do not appear to be different in patients undergoing medical or surgical management of ectopic pregnancy.
A meta-analysis by Barnhart et al., which looked at 26 studies and compared single- to multi-dose methotrexate protocols, found that use of the single-dose methotrexate protocol was associated with significantly greater failure rates. When baseline β-hCG levels and the presence of fetal cardiac activity were controlled for, the single-dose methotrexate therapy had an almost five-times greater failure rate (OR: 4.75) [29].
Small studies have proposed that the success rates for medical management of ectopic pregnancy with single- and multi-dose are comparable [30,31]. However, small studies are underpowered and often lead to a type 2 error: not rejecting the null hypothesis that two therapies are different when in fact they are. In aggregate, treatment failure with single dose is a least 50% higher than multidose (RR: 1.5; 95% CI: 0.44–5.01) and as much as 135% higher when evaluating studies published after the meta-analysis (OR: 2.35; 95% CI: 0.92–7.70; p = 0.06) [32,33].
Given the lower success rate of the single-dose methotrexate protocol, a two-dose methotrexate protocol was developed in the hope of having a more effective regimen that was not too burdensome. In this protocol, the first dose of methotrexate is given on day 1 and a second dose is given on day 4. A third dose is given on day 7 only if the β-hCG level did not decrease by 15% between day 4 and day 7 (see Table 2). This protocol does not require any more office visits than the single-dose protocol, yet gives two doses of methotrexate in the first week of the protocol. The two-dose methotrexate protocol was demonstrated to be safe and well tolerated in a study of 100 patients [34]. Further studies are needed to determine overall success rates.
Several pretreatment characteristics have been studied to determine if they affect the success rates of methotrexate treatment; specifically, β-hCG level on presentation, progesterone level, size of gestation, the presence or absence of fetal cardiac activity and the presence of free blood in the pelvis. A study by Lipscomb et al. of 360 women looked at certain pretreatment characteristics of patients and correlated them with treatment success rates. The only one found to be significant on regression analysis success was initial β-hCG level, with a large decrease in successful treatment (68.2%) seen in patients with β-hCG levels at presentation of greater than 15,000 mIU/ml. The presence of fluid in the peritoneal cavity or size of the ectopic gestation was not associated with a decreased success rate [35]. A more recent study demonstrated that initial β-hCG levels of greater than 5000 mIU/ml are associated with significantly decreased success rates for women treated with the single-dose protocol [36].
Surgery
The traditional surgery performed for an ectopic pregnancy was an exploratory laparotomy with salpingectomy. Today, many patients with ectopic pregnancies that require surgical management are treated with a laparoscopic salpingectomy or salpingostomy. However, if a patient presents in hypovolemic shock with a ruptured ectopic pregnancy, laparotomy and salpingectomy remain the treatment of choice.
Laparoscopy has the benefits of shorter hospital stay, shorter postoperative recovery time and being less expensive compared with laparotomy. We would be more likely to perform a laparoscopic salpingectomy instead of a salpingostomy in the following circumstances: uncontrolled bleeding, recurrent ectopic pregnancy in the same fallopian tube, an ectopic gestation greater than 5 cm or a severely damaged fallopian tube. In other cases, a salpingostomy may be appropriate. A longitudinal incision should be made on the antimesenteric border of the fallopian tube. This can be performed with a unipolar needle. The products of conception should then be removed from the fallopian tube by flushing with high-pressure irrigation. Any bleeding from the fallopian tube can be controlled with the use of electrosurgical fulguration. The incision on the fallopian tube can heal by secondary intention or can be sutured closed.
In a review of nine studies comparing laparoscopic salpingostomy with salpingectomy, there was not a significant difference in subsequent intrauterine pregnancy rate (approximately 50%). However there was an increased rate of repeat ectopic pregnancy in the salpingostomy group (10 vs 15%) [37]. Another study suggests that there may be a higher subsequent fertility rate in patients undergoing salpingostomy instead of salpingectomy [38].
After 5–20% of salpingostomies performed for ectopic pregnancies, there is persistent trophoblastic tissue [39–41]. All patients undergoing salpingostomy need to be followed with weekly β-hCG levels until they are undetectable because of this risk. If β-hCG levels plateau or increase, a persistent ectopic pregnancy is diagnosed. This may be treated with methotrexate. There is an increased risk of persistent ectopic pregnancy if the salpingostomy was performed at a very early gestational age, if the size of the ectopic pregnancy was less than 2 cm or in patients with high initial β-hCG levels [42].
Conclusion
With the use of transvaginal ultrasound and serial β-hCG levels, and in some cases uterine curretage, most ectopic pregnancies can be diagnosed and treated at an early stage. Medical treatment of ectopic pregnancy with methotrexate avoids surgery and, in properly selected patients, is highly successful and well tolerated. The optimal methotrexate protocol is the focus of ongoing research and initial data suggest that the two-dose methotrexate protocol is promising. Medical and surgical treatment of ectopic pregnancy have similar success rates. Future fertility is comparable in medically and surgically treated patients.
Future perspective
Ideally, patients who are at risk for ectopic pregnancy could be screened for and treated earlier, therefore avoiding morbidity and mortality. A study looking at screening asymptomatic women using serum β-hCG level, serum progesterone level and transvaginal ultrasound found a high false-positive rate [43]. Other investigators have looked for a serum-based marker that could be used to diagnose women with ectopic pregnancy. VEGF is elevated in ectopic pregnancies; however, it has low predictive values for these gestations [44,45]. A combination of three markers, VEGF, pregnancy-associated plasma protein-A and progesterone, has been shown to be 97.7% sensitive and 92.4% specific for ectopic pregnancy [46]. Other potential biochemical markers, including creatinine kinase, fetal fibronectin, serum leukemia inhibitory factor and smooth muscle heavy-chain myosin, have not been found to be useful in diagnosing ectopic pregnancies [44,45,47–52]. Gerton et al., who used a proteomic approach on serum from women with ectopic pregnancies with a goal of identifying serum markers, have found potential candidates that will need further characterization [53].
Executive summary
Risk factors
Previous ectopic pregnancy, previous tubal surgery, tubal pathology, known in utero diethystilbestrol exposure or assisted reproductive technologies put patients at a higher risk of developing an ectopic pregnancy.
Symptoms
Symptoms of ectopic pregnancy, including abdominal pain and vaginal bleeding, are neither sensitive nor specific and are also associated with other pregnancy complications, such as miscarriage.
Diagnosis
β-human chorionic gonadotropin levels (β-hCG), transvaginal ultrasound and uterine curettage allow for early diagnosis of ectopic pregnancies.
Treatment
The single-dose methotrexate protocol may have decreased efficacy compared with the multidose protocol.
High initial β-hCG levels (especially >5000 mIU/ml) may decrease the success rate of single-dose methotrexate treatment.
Efficacy of the multidose-methotrexate protocol is similar to that of conservative laparoscopic surgery.
Post-treatment fertility rates are similar in patients undergoing medical or surgical management of ectopic pregnancy.
Footnotes
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.