
Abstract
Treatment programs for women who use drugs during pregnancy have developed out of a backdrop of punitive policies and the psychosocial complexities of this population, which include psychological comorbidities and consideration of the needs of their children. In this literature review, we examine evidence-based approaches to treatment for these women and some promising newer initiatives. We also discuss limitations of this research and issues that need to be addressed. The increasing understanding and acceptance of substance abuse as a treatable mental health disorder brings renewed optimism to this field.
Background
Drug abuse tears at the fabric of our society and the effects on children can be tragic. The most recent National Household Survey on Drug Use and Health estimated that in 2004–2005, 3.9% of pregnant mothers had used illicit drugs, including cocaine, in the past month [101]. Even more alarming, the prevalence rate of illegal drug use was higher for pregnant women in the 15–18-year age range (12.3%) than for women aged 18–25 years (7%). Moreover, the women who abuse illicit drugs often use licit drugs. An estimated 32% of those using one illicit drug during pregnancy also use both alcohol and cigarettes, revealing disturbing estimates of 800,000 to 1 million fetuses exposed to the effects of legal (including alcohol) or illegal substances every year [1,2]. These children are at increased risk of placement in out-of-home care [3]. In addition, substance abuse is a contributing factor in child abuse and neglect cases for 40% or more of the 1.2 million annual confirmed cases of child maltreatment [101] and in 40–80% of families involved with the child welfare system [4]. The presence of substance use disorders in parents increases the risk of child maltreatment by threefold or more [5,6]. In total, 11% of children (8.3 million) live with at least one parent who is either alcoholic or in need of treatment for the abuse of illicit drugs [7]. Young adolescents with parents who abuse substances are two- to three-times more likely to try substances [8,9]. Furthermore, these children are 2.4- to 4-times more likely to have a substance use disorder during adolescence [10]. Even these estimates, conservative as they are based on self report, indicate that gestational exposure to licit drugs of abuse, such as alcohol and cigarettes, and illicit drugs of abuse, such as marijuana, cocaine, methamphetamine and opiates, is the single largest preventable cause of in utero developmental compromise of infants in the USA today.
In the 1980s, the ‘war on drugs’ associated with the crack cocaine epidemic focused national attention on the relationship between drug use and social and economic problems in society. Early reports on prenatal cocaine effects created a public frenzy regarding so-called ‘unfit to parent’ women and their damaged ‘crack babies’. This impacted public perception and state-policy decisions affecting women who used illegal drugs during pregnancy. Treatment for these women is complicated because of the involvement of the child welfare and legal systems, by wide-ranging state statutes, some of which are treatment oriented and some of which are punishment oriented. Treatment programs that target mothers with children face additional issues such as should children be allowed to remain with their parent(s) during substance abuse treatment and differences in professional perspectives and policies between child welfare workers and substance abuse treatment providers. These women are a heterogeneous group and often face, in addition to substance abuse problems, other psychiatric disorders, trauma, domestic violence, poor health, unstable work histories and compromised parenting abilities. Thus, substance abuse cannot be treated as a discrete diagnosis. Recent advances in drug-abuse research have shown that drug addiction is a chronic brain disease [11] and that treatment can result in recovery of damaged brain regions [2,4,12]. This new understanding helps to reduce the stigma of drug abuse by viewing drug abuse as a biologically determined mental health problem rather than as a lifestyle choice.
In this article, we define treatment of substance use during pregnancy broadly to include treatment during pregnancy and/or the postnatal period. We focus on illegal drugs (e.g., cocaine) with the full recognition that most women who use cocaine also use alcohol and tobacco and that the problem is really one of polydrug use [13]. We describe barriers to treatment and evidence-based approaches to treatment, with a focus on those that have been developed over the past 5 years (since 2002). We also discuss issues that need to be addressed in the study of treatment outcomes research in this field and some promising newer initiatives.
Barriers to treatment
The development of treatment programs for drug-using pregnant women surged as a result of the ‘cocaine epidemic’ of the 1980s. Despite the increased support and availability of treatment programs, there are serious barriers to treatment for pregnant substance users. Many programs have relied on male-based recovery models that focus on the individual and not the pregnant/postpartum addict within the context of her family or environment. In fact, it is often difficult for drug-using mothers to be accepted into programs. Many maternal substance users are reluctant to admit drug use for fear of losing custody of their children, or fear criminal prosecution, including negative attitudes by treatment providers, which drives them away from the healthcare system [14]. Lack of resources such as health insurance, transportation and child care, limited residential treatment programs that allow children to stay with their mothers, and staff without training to help the pregnant addict and her children, also dissuade mothers from accessing treatment. These factors contribute to the low numbers of pregnant substance users receiving prenatal care.
Evidence-based approaches
Pregnancy
Treatment that starts during pregnancy is known to be effective. Prenatal clinics are prime settings for identifying substance users during pregnancy and for providing services [15–18]. The 4P's Plus screening tool administered in a prenatal clinic identified 9% of women as using illicit substances, which is higher than the 5.5% reported in national statistics [15].
Length of time
There is increasing evidence that length of time in treatment is critical and that this holds for both residential and outpatient treatment. An analysis of treatment outcomes of pregnant and parenting women in residential treatment programs found longer lengths of stay and treatment completion were the strongest predictors of abstinence following discharge [19]. Length of time in residential treatment was associated with abstinence, obtaining employment, fewer psychiatric symptoms, decreased involvement in the criminal justice system, and more positive parenting attitudes [20]. High rates of retention for pregnant and parenting women in residential treatment were associated with having their children live with them and being involved with child protective services (CPS) or criminal justice [21].
Participation in treatment is affected by pragmatic concerns, such as child care and transportation [18,22–24]. Postpartum African-American women with CPS involvement were more likely to stay in a gender-specific day program than an intensive outpatient program. Women who did not complete treatment endorsed high internal barriers, including severity of the drug problem, not feeling like going to treatment, and negative staff attitudes, and resumed drug use [102].
Treatment engagement
Determining the most appropriate level of treatment and tailoring treatment protocols to meet the specific client needs has shown to impact engagement and retention in treatment [18,25]. However, engaging pregnant substance abusers in treatment remains a challenge. Pregnant substance users with heavier substance use, more psychopathology and involvement in the legal system were more willing to engage in a comprehensive substance abuse day treatment than were women with fewer needs. A study examining the psychopathology of perinatal drug users participating in a comprehensive day program found most of the women (72%) had low psychopathology [26]. For the women in the study with low psychopathology, being in a program that was more intensive than their needs required may have contributed to high attrition rates, leading the authors to conclude that identification of the degree of psychopathology is necessary to best tailor interventions for drug-using women. In a study of pregnant drug users participating in methadone treatment, 73% had a mood or anxiety disorder, which was seen as an indication that mental health services need to be offered to improve treatment outcomes [27].
The Engaging Moms Program was effective in promoting substance using mothers' enrollment in treatment through the use of supportive counselors who worked with the women and their families [23]. Unfortunately, few women remained in treatment after 90 days. In a comprehensive residential 7-day treatment program with intensive outpatient follow-up services, 19% of attrition occurred within the first 5 days [28]. Similarly, in other studies, severity of addiction and psychiatric problems were associated with early termination of treatment [25]. Compared with women who primarily used marijuana, had CPS involvement and were enrolled in a day treatment program, women who primarily used cocaine or crack sought, received and completed outpatient treatment, and were not involved in CPS had more positive treatment outcomes [8]. Although a high percentage (48%) of substance abusing mothers had been sexually abused, another study [29] reported no association between history of sexual abuse and retention, completion or abstinence after discharge when counseling for sexual abuse was offered as part of treatment.
Comprehensive treatment components
There is widespread agreement that treatment for pregnant and parenting substance using women is more effective with comprehensive treatment. Earlier studies are summarized in Table 1 [30]. Recent work supports this approach.
Model programs and key indicators for success.

A review of 38 studies of substance abuse treatment for women found more positive treatment outcomes associated with the provision of child care, prenatal care, mental health services, a focus on women's issues, women-only admissions and comprehensive treatment [22]. In another review, effective programs included improving parenting capabilities and family interventions, home visits during pregnancy to help prepare women for parenting responsibilities, parenting training and collaboration among multiple agencies [31]. Positive treatment outcomes in a study of clients in a long-term comprehensive residential treatment program included abstinence following treatment, no involvement with the criminal justice system, not living with a partner who abused substances, employment gains, improved mental health and obtaining child custody [32]. Increased self-esteem, decreased depressive symptoms and improved parenting attitudes were found in a program with comprehensive, gender-specific services to women with children aged under 3 years, who lived with them in the program [33]. Even though women had more mental health issues than men initially, they had a greater reduction in drug use than men when mental health and gender-specific services were provided [34]. Improvements in a ‘one-stop shop’ program included decreased substance abuse, increased social support, more positive parenting attitudes, less maternal depression, and improvements in child social development [35,50].
Comprehensive treatment is effective in both long-term residential and outpatient treatment modalities [37]. Although analyses of data from national surveys on substance abuse treatment settings for women between 1987 and 1998 showed a slight increase in the proportion of women in all types of substance abuse treatment programs [38]:
“Less than half of the drug treatment providers whose clients were only women provided services for pregnant or postpartum women, prenatal and perinatal care, child care services, women's groups, or domestic violence services”
Another examination of 10 years of outpatient services for women between 1995 and 2005 found that specialized services were decreasing, with less availability of single-sex group therapy, fewer staff with specialized training and a trend towards less child care being provided [39].
Home based
There is a history of home-based interventions [40]. Positive long-term outcomes were reported in a home-visitation program that used an advocacy approach and was staffed by women with backgrounds similar to the perinatal substance users with whom they worked [41]. Outcomes measured at the 3-year treatment completion and following treatment completion found women who participated in the program had high rates of abstinence and low rates of subsequent pregnancies. Another home-based intervention program for women who had used drugs during pregnancy provided home visits by paraprofessionals every week for the first 6 months following delivery and every other week until the babies were aged 12 months [42]. No significant differences were found in maternal competence, parenting attitudes, child responsiveness or substance use between the mothers who received the home-based intervention and a control group, which was attributed to continued substance use and negative parenting attitudes. In a subsample from this study, children in home-based intervention whose mothers had retained custody of them for at least 18 months showed positive results in cognitive and motor development [43]. The Reaching Families Early program found that the use of outreach and case-management services was highly effective in working with a group of perinatal substance users who were primarily poor, urban, single African-American women. More home case-management visits were associated with retaining custody of the child, less drug use and more drug-use treatment [44].
Promising new approaches
Motivational interviewing
Motivational interviewing and computer-based motivational interventions are starting to be used as brief, accessible tools for substance using women [45–47]. Motivational interviewing attempts to increase the motivation for change through empathy, collaboration and setting goals for change. Women who were more compliant with motivational interviewing and behavioral incentives delivered infants with higher birth weights and had more negative drug-urine screens, although they were not drug abstinent [48]. In a study examining the effectiveness of motivational interviewing and behavioral incentives, pregnant substance users needed more intervention to keep appointments and had lower participation rates than a nonuser comparison group, and there was a positive association between the number of completed motivational interviewing sessions and clean urine screens [8,49]. However, no significant group differences were found between a group of perinatal substance users with CPS involvement who received motivational interviewing and a comparison group who were given an educational intervention [45].
substance using postpartum women who used a computer-based motivational intervention program that gave them feedback regarding the negative consequences of drug use, potential benefits to not using, and a summary related to their motivation to change had higher levels of motivation [47]. A one-time computer-based motivational intervention contributed to decreased substance use among the group of postpartum women, who had reported illicit drug use in the month before pregnancy [46].
Mother-infant relationship
Another new focus is interventions that address the emotional aspects of the mother-child relationship. These include working with mothers to help them understand child developmental and psychological needs by increasing their ability to identify and appreciate the impact that their own internal states have on the ways that they perceive and interact with their child [50]. This approach has been shown to reduce parenting stress and maternal depression [51] and to increase mothers' knowledge regarding caring for their infants [52].
Pharmacotherapy
Although medications have been developed to treat addictive disorders, clinical trials typically exclude pregnant women for fear of ethical concerns and legal prosecution if there are negative birth outcomes. Methadone has been the traditional medication of choice for opioid-dependent pregnant women [53]. However, concerns regarding the severity of withdrawal in infants exposed to methadone have led to research on buprenorphine as an alternative. Early evidence has shown shorter hospitalization, less morphine needed to treat neonatal abstinence syndrome (NAS) [54], and less NAS in buprenorphine-exposed compared with methadone-exposed infants [55]. A multicenter clinical trial is underway to determine the safety and efficacy of buprenorphine for this population.
CPS & court involvement
substance abusing parents involved with CPS have a low probability of successful reunification with their children, with the children spending extended periods of time in foster care [56–58]. The latest approach to this problem is represented by the almost 200 family treatment drug courts (FTDC) in the USA. These courts are based on a nonadversarial model and focus on treatment and reunification. Outcome data are-sparse. One report found parents who participated in FTDC were more likely than a comparison group to engage in, stay in and complete treatment and achieve reunification with their children, and were less likely to become re-involved with CPS [56].
Our own program, the Vulnerable Infants Program of Rhode Island (VIP-RI), connects with parents before the newborn infant leaves the hospital, develops a treatment plan based on identified needs and includes a FTDC. VIP-RI has resulted in a reduced length of stay beyond medical necessity for infants in the newborn nursery. The program has also shown earlier reunification in FTDC compared with traditional family courts [59]. Timely permanency represents a significant improvement in family stability, as well as cost savings to the child welfare system. Figures 1 & 2 illustrates the final placement of the infant at the time of discharge from the VIP-RI program compared with the initial placement of the infant at discharge from the hospital (n = 123 cases).
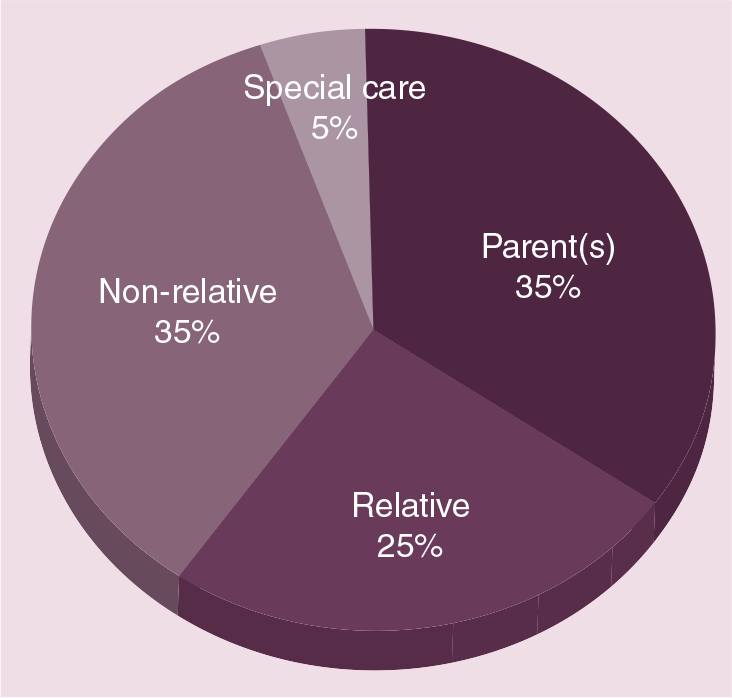
Initial placement of children at hospital discharge.

Final placement of children at Vulnerable Infants Program of Rhode Island discharge.
As evident in Figures 1 & 2, the number of children who were placed with their parent(s) increased from the point of hospital discharge to permanent placement: only 35% of these infants were initially placed with a parent or parents at hospital discharge; this increased to 56% of infants granted permanency with a biological parent. This represents a total of 69 children who achieved permanency with one or both of their biological parents (including five fathers granted sole custody of six children). Including the 21% of infants who were adopted by a relative, a total of 77% of these children remained with members of their birth families. (The term ‘Other’ refers to a specialized placement for a child with medical issues following termination of the parent's rights.)
Discussion
Research on treatment of substance abuse during pregnancy continues to expand. Evidence-based programs suggest that a variety of approaches are effective, including traditional programs, which focus on the pregnancy period, length of treatment, comprehensive treatment and home visitation, and newer approaches, which include motivational interviewing and contingency management, a focus on the mother-infant relationship, collaboration among social service systems, including CPS and FTDC, and pharmacotherapy.
Research limitations
It is difficult to compare approaches or individual programs for several reasons. First, these studies are difficult to evaluate because they are complex and are complicated by methodological issues, including small sample size, many confounding variables, inability to randomize patients to different conditions, and unblinded observers. Second, programs are developed for different purposes. Although it could be argued that abstinence from drug use is (or should be?) the sine qua non of all of these studies, for some studies, abstinence may be the ultimate goal but not the focus of a particular approach, such as a study with the goal of getting women into treatment during pregnancy. Alternatively, a study designed to improve the mother-child relationship might see this objective embedded in the context of a larger abstinence program. A third reason is that studies use a wide array of outcome measures, which are difficult to compare. In addition, there are no long-term follow-up studies. Fourth, studies are developed for different populations. For example, studies that address families involved with the child welfare system have a unique set of issues to address. In a similar vein, there are local population issues. State statues, regional practices, existing services and infrastructure often play a role in how programs are developed. Thus, even when positive generic practices are identified, such as ‘comprehensive services’, they still need to be adapted to the local environment. Finally, most treatment programs are multifaceted. In most cases, it will not be possible to tease out the effects of individual components. In addition, because many programs are based on the needs of the individual, not all participants receive the same treatment. There is no ‘one size fits all’ model, but there are clearly strategies that can be drawn from different models that can be adapted to a specific population. It is also worth noting that, in most cases, programs are not drug specific. In part, this is owing to the polydrug nature of the population, but also because these strategies do seem to be effective across drug groups.
Notwithstanding these limitations, this field has made great strides in the past few years and we have many reasons to be optimistic regarding treatment programs for drug-using mothers. As society moves towards the acceptance of drug use as a mental health disorder, we should see a reduction in many of the barriers to treatment, including the stigma and marginalization of these women, and a shift from punitive, criminalization to treatment based on scientifically informed policies and laws. This will enable drug-using women to take advantage of the kinds of programs described in this article and contribute to the development of improved treatment approaches as we continue to increase our understanding of their needs. For example, more women in treatment during pregnancy will reduce the number of drug-affected babies, the number of families involved with the child welfare system and the number of children in foster care.
Innovative new approaches
The past few years have seen the development of innovative programs that, although not evidenced-based, are promising. The Zero Exposure Project developed a public awareness education campaign regarding substance use during pregnancy by using a website, radio announcements, a toll-free information and referral line, and providing outreach to female inmates [60]. In the Milagro Program [16], screening for substance use, education, prevention and referrals at a prenatal clinic were effective in increasing women's willingness to engage in comprehensive services.
Treatment programs are showing an increased sophistication regarding psychological aspects of the mother-infant relationship. A Finnish residential program for pregnant and postpartum women helps mothers with infant mental health issues [32]. The mother-infant relationship is also a primary focus of a Toronto-based program that provides the mother with a therapeutic relationship to foster the development of a nurturing relationship with her infant [49].
Partners are increasingly recognized as influencing women's recovery efforts and affecting family functioning, including the roles of substance using men as fathers [61–64]. It has been suggested that families affected by drug use during pregnancy can be best served when the needs and strengths of the partners can be identified, creating opportunities for intervention in the service of promoting more adaptive family functioning whether or not the couple remains together [65].
We know that outcomes for substance using pregnant women depend not only on their individual life experiences and characteristics but also on factors related to social service systems, societal institutions, and conditions beyond their direct control [66,67]. When does the need for treatment end? Our preliminary data suggest that parents continue to need support for substance use, mental health and parenting after their involvement with FTDC [66].
The cost-benefit of treatment for this population is complex because the impact that pregnant and parenting women have on society is especially pronounced, as women are typically the primary caregivers in a family. The high cost of comprehensive, long-term residential programs for pregnant and parenting women may make them targets of cost-saving measures, raising questions as to whether the costs can be justified and if there may be alternative, more economical ways to provide services [19,38]. There is evidence that a specialty residential treatment program has a more favorable net benefit (US$17,144) than a standard residential treatment program (US$8090) [68]. A quality-of-life index also showed treatment and cost-benefit effects [69]. When the cost of providing special education services for these children when they get to school is considered, there is no doubt regarding the cost-effectiveness of programs for pregnant women and mothers with young infants [70]. An earlier study provided further evidence of the cost-effectiveness of the five different treatment modalities (detoxification, methadone, residential, outpatient, and a combination of residential and outpatient treatment) for pregnant substance using women [71]. Findings showed that involvement in treatment led to a noticeable reduction in the costs of crime-related activities, with the two types of residential programs showing the greatest cost-benefits.
Conclusion
We no longer have to ask if treatment works for women who use drugs during pregnancy. As shown in this review, there is evidence-based research that documents the effectiveness of a number of approaches, some that have a history of success (prenatal care, length of treatment, comprehensive and home-based approaches) and others that are more recent (motivational interviewing, contingency management, FTDC, mother-infant interaction and pharmacotherapy). The recognition of the importance of relationships, with increased focus on mother-child relationships and the need to include partners, not only to address problems such as domestic violence but also as an important component of family life, reflects a more nuanced understanding of the complexity of this problem. However, this enthusiasm is somewhat diminished by the methodological limitations of the current literature. Large, randomized trials in multiple settings with long-term follow-up are critical. Even so, with the scientific basis we have for addiction as a brain disease and the efficacy of treatment programs, it is ironic that policy has still not caught up with all that we have learned.
Future perspective
Continued advances in drug-abuse research show that drug addiction is a chronic brain disease that can be treated. The stigma of drug abuse during pregnancy is reduced. Programs are expanded to treat the whole family, including infants, older children and partners. Treatment goals should include child developmental and psychological needs. Large, randomized trials in multiple settings that include long-term follow-up are conducted to support traditional programs as well as new approaches. Pharmacotherapy approaches are developed in conjunction with behavioral treatments. Reimbursement for substance use and mental health services are bundled to make treatment more affordable and accessible, including carve outs for special populations. New approaches that await empirical validation include better use of the media and other technology and more attention to relationships, including the mother-infant relationships and the role of partners, and a broader understanding of the other forces that affect these women's lives, such as domestic violence.
Executive summary
Background
Gestational exposure to licit and illicit drugs of abuse is the single largest preventable cause of in utero developmental compromise of infants in the USA today.
Treatment for women who use drugs during pregnancy is complicated by mental health comorbidities, domestic violence, poverty, poor health, needs of their children, involvement with child protective services and legal systems, parenting and social stigma.
Barriers to treatment
Barriers to treatment include lack of resources such as health insurance, transportation and child care, and lack of availability of treatment programs.
Fear of punishment drives women away from the healthcare system, jeopardizing prenatal care.
Evidence-based approaches
Treatment that begins during pregnancy.
Increased length of treatment, whether residential or outpatient.
Comprehensive treatment including, but not limited to, prenatal care, mental health services, child care, parenting and women's issues.
Home-based treatment.
Promising new approaches
Motivational interviewing and contingency management.
Emphasis on the mother-infant relationship.
Treatment integrated with child protective services and the court, such as the establishment of family treatment drug courts.
Research limitations
Studies are limited by methodological problems including small sample size, many confounding variables, inability to randomize patients to treatment conditions, and unblinded observers.
There is no ‘one size fits all’ model but there are strategies that can be drawn from different models that can be adapted to a specific population.
Choice of a specific approach depends, in part, on the circumstances of the particular population, although there is consensus that comprehensive treatment is preferred.
There is some evidence that treatment is cost-effective.
Footnotes
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.