
Abstract
Epilepsy affects 50 million people worldwide, including women afflicted with catamenial epilepsy. Catamenial epilepsy is a form of epilepsy in which seizures are clustered around specific points in the menstrual cycle, most frequently during the perimenstrual or periovulatory phase. Although there are a number of standard and newer antiepileptic drugs for epilepsy, no specific drugs exist to treat catamenial seizures, which affect at least one in three women with epilepsy. Moreover, the molecular pathophysiology of catamenial seizures remains unclear. This article describes the pathophysiology, hormonal basis, diagnosis and treatment of perimenstrual catamenial epilepsy. Natural progesterone and synthetic neurosteroid replacement appears to be a suitable therapeutic approach for catamenial epilepsy.
Definition & prevalence of catamenial epilepsy
Epilepsy is a neurological condition characterized by repeated occurrence of seizures, which are clinical manifestations of abnormal electrical discharges in the brain. Epilepsy affects an estimated 2.7 million people in the USA and 50 million worldwide [1,2], of whom approximately 40% are women. Despite many advances in epilepsy research, nearly 30% of people with epilepsy have ‘intractable seizures’ that do not respond to even the best available treatment. Accurate diagnosis of seizure type and epileptic syndrome is critical for determination of appropriate drug therapy and prognosis.
Epilepsy is characterized by the unpredictable occurrence of seizures. However, there is a form of epilepsy, called catamenial epilepsy, which does not adhere to this lack of pattern. Catamenial epilepsy, from the Greek katomenios, meaning ‘monthly’, is characterized by seizures that cluster around specific points in the menstrual cycle (Figure 1). Catamenial epilepsy affects 10–70% of women with epilepsy [3–8]. The large variation in prevalence of catamenial epilepsy is partly due to methodological differences, such as the criteria used for defining seizure exacerbation in relation to menstrual cycle, patients self-reporting, diaries and other inaccurate records of seizures relating to menses. In general, a twofold or greater increase in seizure frequency during a particular phase of the menstrual cycle could be considered as catamenial epilepsy [7–10]. Based on this criterion, recent studies confirmed that catamenial epilepsy affects 39–60% of women with epilepsy [7,8]. Thus, there is a need to reconcile these differences in the prevalence rate of catamenial epilepsy. In a recent study by Herzog and colleagues, the frequency of catamenial epilepsy was assessed in 87 women who charted seizures and menses during three cycles [7]. Overall, 39% of the women had catamenial epilepsy, which supports the prevailing notion that at least one in every three women with epilepsy show catamenial seizure exacerbation.
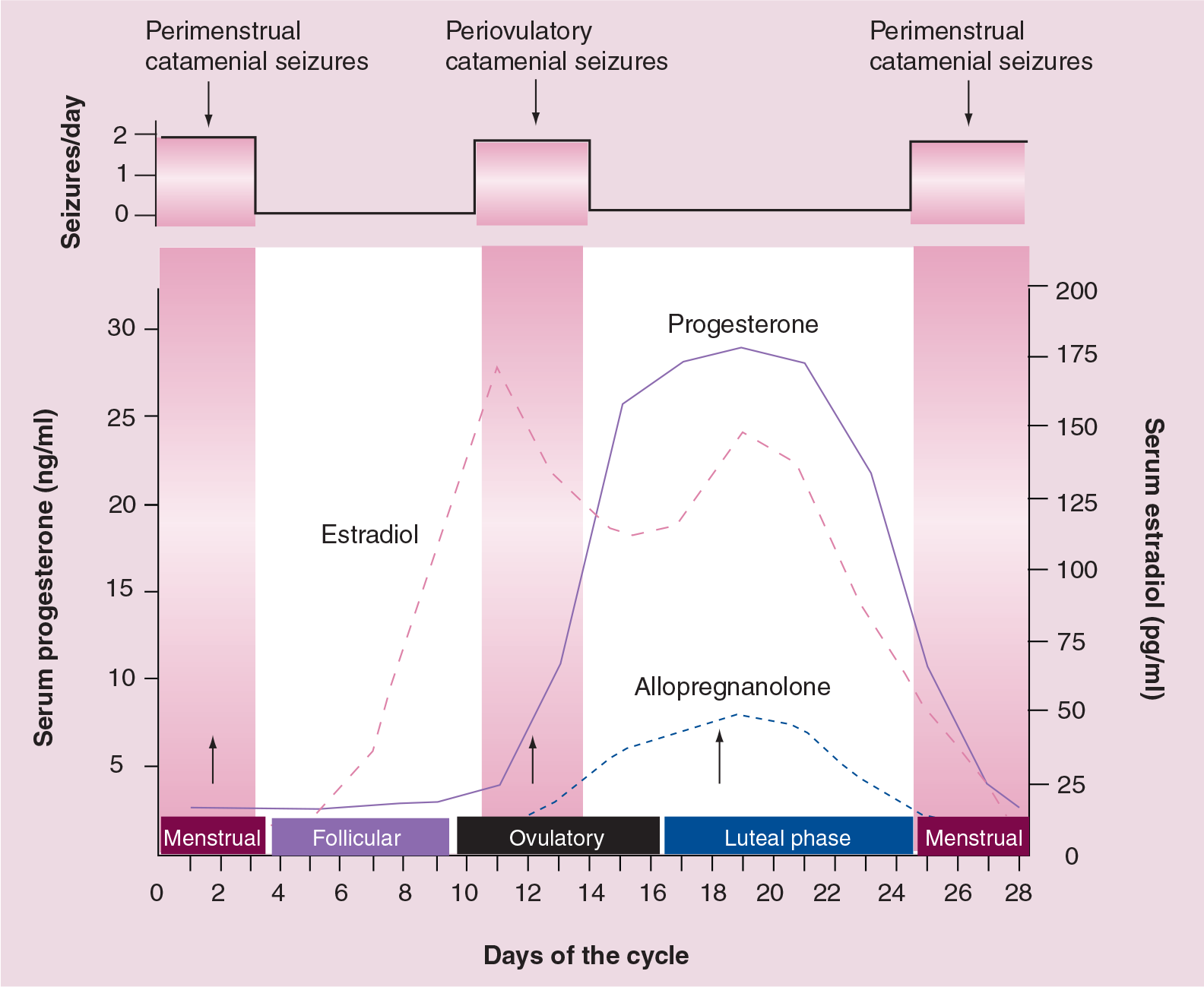
Relationship between ovarian hormones and seizure susceptibility during the menstrual cycle.
Despite such high incidence and increased awareness, there is no widely accepted definition of catamenial epilepsy. Based on the review of a vast clinical experience, Newmark and Penry defined perimenstrual catamenial epilepsy as epileptic seizures occurring in women of fertile age exclusively or significantly more often during a 7-day period of the menstrual cycle, beginning 3 days before menstruation and ending 4 days after its onset [9]. Catamenial seizure exacerbations can also occur less frequently at other phases of the menstrual cycle (see ‘Patterns & diagnosis’, below). Emerging studies on the prevalence rate of catamenial epilepsy and the lack of a standard diagnosis demonstrate the complexity of the condition and the difficulty involved in studying it [10]. A detailed understanding of the patterns and pathophysiology is essential for the development of rational approaches for the prevention and treatment of catamenial epilepsy.
Patterns & diagnosis of catamenial epilepsy
The need to develop better diagnostic tools of catamenial epilepsy and catamenial patterns has been widely recognized. Recently, Herzog and colleagues described three distinct patterns of catamenial epilepsy: perimenstrual, periovulatory and inadequate luteal-phase catamenial seizures [11]. However, these authors observed that the conventional perimenstrual form of Newmark and Penry is the most common clinical type. Overall, catamenial epilepsy designation can be made if a twofold or greater increase in seizure frequency is observed during a particular phase of the menstrual cycle. In the primary clinical type, perimenstrual catamenial epilepsy, women with epilepsy experience an increase in seizure activity before, during or after the onset of menstruation [9,10].
Catamenial epilepsy is observed in women with ovulatory or anovulatory cycles. Women with ovulatory cycles could experience either perimenstrual or periovulatory catamenial pattern, or even both patterns, within a single cycle. Approximately 16.5% of cycles in study subjects were found to be anovulatory, and these women showed a third pattern, referred as inadequate luteal-phase catamenial seizures [7]. Among anovulatory cycles, average daily seizure frequency could be substantially less during the midfollicular phase than during the remainder of the cycle. Despite emerging information, very few physicians at the time were aware of menstrual cycle-related seizures.
The diagnosis of catamenial epilepsy is mainly based on the assessment of menstruation and seizure records [2,11]. A detailed diary of seizures and menstrual cycle is important for accurate diagnosis of catamenial epilepsy. The simple approach to evaluation of catamenial epilepsy, that is, whether the patient's seizures tend to worsen at certain points of the menstrual cycle, is to record a seizure diary in relation to the menstrual cycle. Using the first day of menstrual bleeding as the first day of the cycle, the menstrual cycle is divided into four phases:
Menstrual phase (days −3 to +3)
Follicular phase (days +4 to +9)
Ovulatory phase (days +10 to +16)
Luteal phase (days +17 to −4) (Figure 1)
The number of seizures in each phase is counted for at least two cycles, and a twofold or greater increase in frequency during a particular phase of the menstrual cycle can be used as the diagnostic criteria of catamenial epilepsy.
In women with epilepsy with normal ovulatory cycles, the perimenstrual catamenial pattern is characterized by a greater average daily seizure frequency during the menstrual phase compared with the midfollicular and midluteal phases [11]. By contrast, the periovulatory pattern is characterized by a greater average daily seizure frequency during the ovulatory phase compared with the midfollicular and midluteal phases in normal ovulatory cycles. In women with anovulatory cycles, the inadequate luteal catamenial pattern is characterized by a greater seizure frequency during the ovulatory, luteal and menstrual phases than during the midfollicular phase. Overall, the seizure frequency–menstrual days chart in women with catamenial epilepsy would show greater catamenial exacerbation than the point of inflection of the S-shaped distribution of the seizure exacerbation curve [12,13]. Alterations in seizure activity in women may also be seen during changes in reproductive status (i.e., entering puberty, during pregnancy or after menopause).
Pathophysiology of catamenial epilepsy
Catamenial epilepsy is among the oldest neurological disorders known, with early reports in 1881, yet the molecular mechanisms involved in the pathophysiology of catamenial epilepsy are not well understood. There is presently no specific treatment and, often, conventional therapies have a disappointing lack of effect. Although recent studies have provided an improved understanding of hormonal changes that are responsible for catamenial seizure exacerbations [13], there is a large gap in our understanding of what changes occur in the brain in relation to the hormonal fluctuations associated with the menstrual cycle and how these changes alter sensitivity to anticonvulsant drugs. Thus, elucidation of the physiological basis of catamenial epilepsy is a prerequisite to develop specific targeted approaches for treatment of the disorder.
Catamenial epilepsy is a multifaceted condition attributed to numerous causes. A variety of mechanisms, such as fluctuations in antiepileptic drug (AED) levels, changes in water and electrolyte balance and physiological variation in ovarian hormone secretion, have been proposed as causes for catamenial epilepsy [12,13].
Overall, cyclical changes in the circulating levels of estrogens and progesterone are now widely accepted to be important in the development of this disease (Figure 1). Generally, estrogens are found to be proconvulsant, while progesterone has a powerful antiseizure effect and reduces seizures [13], and thus plays a critical role in the pathophysiology of catamenial epilepsy (see ‘Hormonal basis’ below).
In women with epilepsy, both seizures and AEDs can disturb the menstrual cycle [14]. Seizures can profoundly affect steroid hormone secretion and regulation in women with epilepsy and are the leading cause of increased incidence of menstrual disturbances in epilepsy. For example, seizures can alter the release of hypothalamic and pituitary hormones such as luteinizing hormone/follicle stimulating hormone secretion, while some AEDs alter concentrations of sex steroid hormones. Women with epilepsy are at increased risk for polycystic ovary syndrome [15]. Sexual dysfunction is common among patients with epilepsy and studies have found reduced fertility rates among women with epilepsy [14].
AEDs provide satisfactory control of seizures in most patients (
Summary of standard and nonstandard (newer) antiepileptic drugs.
GABA: γ-aminobutyric acid; IS: Infantile spasms; LGS: Lennox–Gastaut syndrome; SE: Status epilepticus; NMDA: N-methyl-d-aspartate.
Enzyme-inducing and nonenzyme-inducing antiepileptic drugs.
Weak enzyme-inducing AED. AED: Antiepileptic drug.
Hormonal basis of catamenial epilepsy
As illustrated in Figure 1, cyclical changes of ovarian hormones, estrogens and progesterone are now widely believed to be important in the pathogenesis of catamenial epilepsy. Overall, progesterone has antiseizure effects, while estrogens have the opposite effect. There is emerging evidence that endogenous neurosteroids, including those derived from adrenal steroid hormones and circulating androgens, substantially influence seizure susceptibility [13]. However, it remains unclear if there are substantial differences in plasma levels of steroid hormones between women with or without catamenial epilepsy.
Estrogens may play an important role in catamenial seizures. There are three biologically active forms of estrogen: 17β-estradiol, dominant in premenopausal women; estriol, the major form of estrogen during pregnancy; and estrone, which is prevalent after menopause. Estradiol has been shown in many studies to have significant proconvulsant effects [18]. It facilitates various forms of induced seizures and has been shown to worsen seizures in women with epilepsy. On a cellular level, estradiol, aside from its normal reproductive effects, enhances neural excitation and suppresses inhibition. It also creates changes in the physical properties of some neurons (increase in excitatory dendritic spine density in the hippocampus), resulting in increased potential for seizures. Therefore, periovulatory catamenial exacerbation has been attributed to the midcycle surge of estrogen that is relatively unopposed by progesterone until the early luteal phase [19,20]. An increase in the ratio of estrogen:progesterone levels during the perimenstrual period might at least partly contribute to the development of perimenstrual seizure exacerbation.
The effect of estrogens on cortical excitability and seizure frequency is still contentious. In contrast to the seizure-inducing effect of estrogens found in several studies [18], some studies support an inhibiting effect of estrogens on cortical excitability [21,22]. Estradiol regulation of the hippocampal expression of glutamic acid decarboxylase (GAD), the principal enzyme involved in the synthesis of the inhibitory neurotransmitter γ-amino-butyric acid (GABA), could lead to a decrease in seizure susceptibility [23]. However, the exact relationship between circulating estrogens, GAD expression and frequency of catamenial epilepsy remains unclear.
Progesterone plays a critical role in catamenial seizures. Progesterone has long been known to have anticonvulsant properties [24,25]. Animal models and human clinical studies have shown the efficacy of progesterone in reducing both the frequency and severity of seizures. The clustering of seizures around the beginning of menstruation corresponds with a significant drop in the levels of progesterone circulating in the body and an increase in the estrogen:progesterone ratio. There is strong evidence that, rather than the increase in estrogens, it is the decrease or withdrawal of progesterone that partly triggers catamenial seizure exacerbation. The effects of this withdrawal could be highly relevant in perimenstrual catamenial epilepsy. The luteal catamenial seizures can be attributed to the diminished progesterone levels that occur during inadequate luteal-phase cycles.
There are two mechanisms by which progesterone affects reproduction and seizure susceptibility: binding to progesterone receptors and being metabolized to the neurosteroid allopregnanolone. Neurosteroids such as allopregnanolone are synthesized from progesterone by two sequential A-ring reductions [13]. Evidence shows that the antiseizure effects of progesterone are due to allopregnanolone, a metabolite of progesterone [24,26]. Allopregnanolone is a member of a class of compounds known as neurosteroids. Neurosteroids are steroids that are synthesized locally in the brain and have a robust and rapid effect on neural excitability [27]. Allopregnanolone is a potent, broad-spectrum anticonvulsant neurosteroid. It has been shown to protect against various forms of induced seizures. Recently, it has been discovered that allopregnanolone is a potent positive modulator of GABAA receptors. GABA is the primary inhibitory neurotransmitter in the brain [28]. Allopregnanolone has specific, distinct binding sites on GABAA receptors that are separate from those for GABA, benzodiazepines and barbiturates. It is an endogenous modulator, which has high-affinity binding sites on the GABAA receptor. Structurally, GABAA receptors are believed to be pentameric, with five protein subunits that form the chloride ion channel pore. The binding of allopregnanolone to neurosteroid sites on the GABAA receptor causes a massive influx of chloride ions into the neurons, leading to hyper-polarization and, consequently, potentiation of inhibitory neurotransmission. This mechanism almost certainly underlies allopregnanolone's protective actions against seizures. At normal physiological levels it is sufficient to activate these receptors. This suggests that an abrupt withdrawal of allopregnanolone at the onset of menstruation could decrease inhibitory effect and possibly exacerbate seizures [29,30].
Animal models of epilepsy play a key role in the discovery and characterization of AEDs. Conventional models based on acute seizure induction are not suitable for testing therapies targeted at catamenial epilepsy. Animal models of catamenial epilepsy should be designed to simulate the menstrual cycle, with its accompanying changes in seizure susceptibility. Recently, two types of models have been described in animals that partially resemble catamenial seizure patterns [10]. In the first category of models, attempts are made to mimic the luteal phase by inducing extended high levels of progesterone and estrogens, followed by rapid decline to simulate the menstruation (Figure 1). This model simulates the rise and fall of estrogen and progesterone at the point in the cycle associated with increased seizure susceptibility [31]. Some examples of this model are pseudopregnancy, chronic progesterone treatment and progesterone (neurosteroid) withdrawal models. The second category of models is based on the naturally occurring estrous cycle, or administration of exogenous hormones that simulate the specific stages of estrous cycle in ovariectomized rats.
The neurosteroid withdrawal model of catamenial epilepsy is based on the hypothesis that abrupt withdrawal of progesterone, and hence allopregnanolone, will cause increased seizure susceptibility. Our team has proposed a pseudopregnancy model where high levels of progesterone were induced over time and then rapidly withdrawn by treating the animals with finasteride [31,32]. Finasteride is a 5α-reductase inhibitor that blocks the reduction of progesterone to allopregnanolone. Acute withdrawal produced an increase in seizure susceptibility, while a long-term reduction in allopregnanolone levels did not. This is consistent with the perimenstrual pattern of catamenial epilepsy.
Validation of animal models of catamenial epilepsy requires certain criteria to be met for them to be representative of the human condition. They should include close similarity in eliciting an epilepsy-like state and a pathophysiology that mirrors the disease in women. The neurosteroid withdrawal model partly meets these criteria and would offer several advantages over the use of conventional seizure models [31,32]. The pseudopregnancy–neurosteroid withdrawal model better simulates changes in the allopregnanolone:estrogen ratio that is believed to be critical for perimenstrual catamenial epilepsy. However, the actual endocrine conditions that exist in the menstrual cycle are different from those in either the pseudo-pregnant rat or the chronically progesterone-treated, ovariectomized rat. Moreover, the absence of spontaneous recurrent seizures in these models raises concern regarding whether these models represent epileptogenesis or acute increase in seizure susceptibility and drug resistance. While the neurosteroid withdrawal model is suitable for assessing ‘acute’ symptomatic anticonvulsant therapies for catamenial epilepsy, a chronic, clinically relevant model of catamenial epilepsy that has spontaneous recurrent seizures is warranted for testing antiepileptogenic strategies for the prevention of catamenial epilepsy in women at risk.
Drug treatment of catamenial epilepsy
The standard and nonstandard (newer) AEDs used in the treatment of seizure disorders are listed in Table 1 . However, none of these agents meets the ideal characteristics of an AED, that is, protecting against seizures without inducing adverse effects that impair the patient's quality of life. The conventional AEDs are the mainstay for the management of catamenial seizures in women. Approximately a third of women with epilepsy use more than one AED appropriate to their seizure type. However, there is currently no specific treatment for catamenial epilepsy. This is partly because catamenial seizures are often refractory to conventional AEDs such as valproate, phenytoin and diazepam [12,13]. Many of these drugs are prescribed for treatment of catamenial epilepsy without direct studies of effectiveness, with their use based primarily on empirical evidence.
Endocrine treatment of seizures may rationally be aimed at those endocrinological aspects of seizures that act either to exacerbate or ameliorate them. As progesterone has anticonvulsant effects and estrogen has proconvulsant effects, treatment with progesterone or estrogen antagonists may prove to be useful adjunctive treatments in appropriate patients. Table 3 lists an overview of various drugs investigated for the treatment of catamenial epilepsy. Many patients received these agents as supplements or adjunct drugs in a continuous or intermittent approach for inhibition of catamenial seizures [33,34]. While these agents may be helpful for the treatment of catamenial seizures, each is based on small, unblinded studies or anecdotal reports [33,34].
Overview of pharmacotherapy of catamenial epilepsy.
GABA: γ-aminobutyric acid.
Some drastic treatment strategies such as hysterectomy or oophorectomy, as well as administration of oral contraceptives, have been tried for catamenial exacerbation. In addition, drug therapeutic monitoring and dosage adjustments are necessary in women receiving some AEDs (
Acetazolamide
Acetazolamide is the prototype of a class of agents that are potent inhibitors of carbonic anhydrase, a key enzyme involved in NaHCO3 reabsorption and water balance in the kidney. Carbonic anhydrase is also present in the brain. Acetazolamide has been used empirically for years for the treatment of refractory epilepsy and catamenial seizures [35,36]. In a study by Lim and colleagues, the efficacy of acetazolamide was tested in 20 women with catamenial epilepsy [37]. Approximately 30–40% of subjects showed a significant reduction in overall seizure frequency and severity. This study was a retrospective telephone interview of women who had used acetazolamide in the past and hence might not be as reliable as a controlled clinical study. However, loss of efficacy or tolerance is a problem reported by many women treated with acetazolamide.
Benzodiazepines
Benzodiazepines, such as clonazepam and clobazam, are positive allosteric modulators of GABAA receptor and broad-spectrum antiseizure agents. Clonazepam is highly useful in the therapy of absence and myclonic seizures, but was associated with tolerance to its antiseizure effects [38]. Clobazam has been found to be an effective agent for the treatment of catamenial epilepsy [39,40]. Clobazam (20–30 mg/day) was administered intermittently 2–4 days before menses, probably to avoid the tolerance usually associated with continual therapy. The most common adverse effects of clobazam are sedation and depression. The clobazam dosage in the above study appears to be very high, as 5–10 mg/day is a more commonly used dose. A lower dose may be associated with a reduced severity of side effects. However, cross-tolerance to benzodiazepines has been described in animal models due to chronic exposure to neuroactive steroids, which could affect the clinical utility of benzodiazepines in catamenial epilepsy therapy [41].
Medroxyprogesterone acetate
Medroxyprogesterone acetate (MPA) is a widely investigated progestin-only contraceptive agent. MPA treatment in women with catamenial seizures found that it produces a 39% reduction in seizure frequency at a mean follow-up of 1 year [34,42]. Suppression of seizures was evident when the patients were treated with parenteral MPA at dosages that were designed to completely eliminate menses. Therefore, it is conceivable that in long-term MPA therapy it may be the elimination of ovarian function that is critical for suppression of catamenial exacerbation. Treatment with MPA is associated with problems such as weight gain and spotting. Moreover, stoppage of the MPA injections is associated with prolonged delays in the return of regular cycles, during which time seizures are sometimes exacerbated by the intervening anovulatory cycles.
Natural progesterone
Cyclic natural progesterone use has been demonstrated to be an effective treatment for catamenial and noncatamenial seizures in women [33,43,44]. Cyclic natural progesterone supplement has been used in dosages that mimic physiological range levels. Progesterone is efficiently absorbed after oral administration as lozenges and rectal administration as suppositories. Progesterone was given at 100–200 mg, thrice daily, on days 15–28 of the menstrual cycle. In a 3-month investigation of cyclic natural progesterone therapy, 23/25 (92%) women with intractable seizures completed the trial. Average monthly seizure frequency was reportedly reduced by 54–68% during the 3-month treatment period [44]. A 3-year follow-up report found that 15 of the women continued on the same AED and progesterone protocol. These women continued to have a very substantial (62–74%) reduction in seizure frequency [33]. Two women who did not complete the 3-month trial dropped out owing to sedative (asthenia or depression) side effects, all of which resolved within a day of dose reduction. The safety profile of cyclic natural progesterone use has permitted it to be investigated in a US NIH clinical trial. High efficacy and ready availability make progesterone a valuable treatment for catamenial seizure exacerbation. It is yet to be recognized, however, as an approved form of therapy for catamenial epilepsy. Progesterone therapy in women may cause hormonal effects such as breakthrough vaginal bleeding and breast tenderness.
Experimental evidence from studies in animal models and clinical data are consistent with the possibility that the antiseizure effects of progesterone are due to its metabolic conversion to neurosteroids, principally allopregnanolone [24,45–47]. The concurrent use of finasteride, an inhibitor of 5α-reductase required for the conversion of progesterone into allopregnanolone, with progesterone therapy has resulted in marked exacerbation of seizures in women with epilepsy [47]. Thus, finasteride should be contraindicated in women with epilepsy. Owing to the potent antiseizure efficacy of the neurosteroid allopregnanolone, synthetic GABAA receptor-modulating neurosteroids, which are devoid of hormonal side effects, could provide a rational alternative approach to therapy.
Experimental agents
The neurosteroid withdrawal hypothesis presents the possibility for novel, highly effective treatments. Using the catamenial epilepsy model, we evaluated the hypothesis that neurosteroid replacement is an effective and rational therapy for catamenial epilepsy [32,48]. During this seizure-prone state, the activity of conventional AEDs, including diazepam and sodium valproate, is reduced, possibly accounting for the clinical impression that catamenial seizures are unusually drug resistant. Unexpectedly, neurosteroids that positively modulate GABAA receptors actually have enhanced anticonvulsant potency in the model, providing support for a neurosteroid replacement approach to the treatment of catamenial epilepsy [32,48]. Overall, these observations suggest that neurosteroids represent a specific treatment approach for perimenstrual catamenial seizure exacerbations. It suggests that cyclic replacement therapy would be highly effective. Unfortunately, natural neurosteroids are ineffective as treatments. They are orally inactive, have a very short half-life (minutes) and have the potential to metabolize to compounds that produce undesirable hormonal effects. A synthetic version of allopregnanolone, called ganaxolone, is available [49]. Ganaxolone was designed to overcome the limitations of naturally occurring neurosteroids, with significant improvements in pharmacokinetic and therapeutic properties.
Ganaxolone is a synthetic 3β-methyl analogue of allopregnanolone [49]. The 3β-methyl substituent minimizes metabolism at the 3α-hydroxyl group so ganaxolone is orally active, is not converted to the hormonally active 3-keto form and hence lacks hormonal side effects. Like allopregnanolone, ganaxolone is a potent positive allosteric modulator of GABAA receptors and a broad-spectrum anticonvulsant agent. The anticonvulsant potency of ganaxolone is enhanced in the period following neurosteroid withdrawal in a rat model of catamenial epilepsy, while the potencies of two reference anticonvulsants, diazepam and valproate, are reduced [32]. Recently, a total of over 500 people have received ganaxolone in several Phase II clinical trials [50]. Safety and tolerability in the human experience have been impressive, except for a dose-dependent sedation. In a preliminary study, ganaxolone was evaluated in women with catamenial epilepsy [51]. Patients received oral ganaxolone (300 mg/day, twice daily) starting on day 21 of the menstrual cycle and continuing to the third full day following the beginning of menstruation. During the 4 months of this ganaxolone ‘pulse’ therapy, patients had a marked decrease in their catamenial seizures. Ganaxolone is still at development stage but researchers hope that it may provide a specific treatment option for catamenial epilepsy.
Given the neurosteroid's critical role in catamenial seizures and ganaxolone's enhanced potency, ganaxolone may offer a rational approach for the treatment of perimenstrual catamenial epilepsy without producing hormonal side effects. Owing to ganaxolone's unique modulatory profile, ganaxolone could be an effective agent in cases where other GABAA receptor modulators fail to offer seizure protection because ganaxolone modulates most GABAA receptors with distinct subunits [49].
Executive summary
Catamenial epilepsy is characterized by seizures that cluster around specific points in the menstrual cycle, most frequently during perimenstrual and periovulatory phases.
Perimenstrual catamenial epilepsy can be defined as epileptic seizures occurring in women of fertile age exclusively or significantly more often during a 7-day period of the menstrual cycle, beginning 3 days before menstruation and ending 4 days after its onset.
In general, a twofold or greater increase in seizure frequency during a particular phase of the menstrual cycle could be considered as catamenial epilepsy.
Recent studies indicate that catamenial epilepsy affects 39–60% of women with epilepsy. Overall, one in three women with epilepsy shows catamenial seizure exacerbation.
Detailed understanding of the patterns and pathophysiology is essential for the development of rational approaches for the prevention and treatment of catamenial epilepsy.
There are three patterns of catamenial epilepsy: perimenstrual, periovulatory and inadequate luteal-phase catamenial seizures.
Catamenial epilepsy is observed in women with ovulatory or anovulatory cycles. Women with ovulatory cycles could experience either perimenstrual or periovulatory catamenial pattern.
Among anovulatory cycles, average daily seizure frequency could be substantially less during the midfollicular phase than during the remainder of the cycle.
Diagnosis of catamenial epilepsy is mainly based on the assessment of menstruation and seizure records of at least two cycles.
The number of seizures in each phase (menstrual, follicular, ovulatory and luteal) is counted and a twofold or greater increase in frequency can be used as criteria for the diagnosis of catamenial epilepsy.
Catamenial epilepsy is a multifaceted condition attributed to numerous causes.
A variety of mechanisms, such as fluctuations in antiepileptic drug (AED) levels, changes in water and electrolyte balance and physiological variation in ovarian hormone secretion, have been proposed as causes for catamenial epilepsy.
Overall, estrogens are found to be proconvulsant, while progesterone has a powerful antiseizure effect and reduces seizures. At times when the level of estrogen is high relative to progesterone, as occurs before the menses, the likelihood of seizures would increase.
Some AEDs, such as phenytoin, carbamazepine and phenobarbital, are potent enzyme inducers and thereby enhance metabolism of steroid hormones, which may cause the increase in breakthrough seizures in women.
Both seizures and AEDs can disturb the menstrual cycle in women with epilepsy.
Hormonal changes that are experienced during the menstrual cycle play a large role in the increased seizure susceptibility. Cyclical changes in the circulating levels of estrogens and progesterone are now widely accepted to be important in the development of this disease.
There is emerging evidence that endogenous neurosteroids, including those derived from adrenal steroid hormones and circulating androgens, substantially influence seizure susceptibility.
Estrogen is a key hormone in catamenial seizure exacerbation. Estradiol has been shown in many studies to have significant proconvulsant effects and increases neuronal excitability.
Periovulatory catamenial exacerbation has been attributed to the midcycle surge of estrogen that is relatively unopposed by progesterone until early luteal phase.
Progesterone plays a critical role in catamenial seizures. Progesterone is a powerful anticonvulsant hormone. Thus, withdrawal of progesterone during the perimenstrual period could result in catamenial seizure exacerbation.
The antiseizure effects of progesterone are due to its metabolic conversion in the brain to allopregnanolone, a neurosteroid and potent positive modulator of γ-aminobutyric acid A receptors.
There is substantial evidence that neurosteroids such as allopregnanolone are endogenous modulators of seizure susceptibility.
Recent data suggest that an abrupt withdrawal of allopregnanolone at the onset of menstruation could decrease inhibitory effect and possibly exacerbate seizures due to hyperexcitability of hippocampal neurons.
Executive summary
Currently, there is no specific drug therapy for catamenial epilepsy. Conventional AEDs are the mainstay for the management of catamenial seizures.
Drugs such as acetazolamide, benzodiazepines, medroxyprogesterone acetate and progesterone have been tested in women with catamenial epilepsy.
Many patients received these agents for inhibition of catamenial seizures. While these agents, which are given as supplements or adjunct drugs in a continuous or intermittent fashion, may be helpful for the treatment of catamenial seizures, each is based on small, unblinded studies or anecdotal reports.
Cyclic natural progesterone use has been shown to be an effective therapy for catamenial epilepsy. Progesterone is given at 100–200 mg, thrice daily, on days 15–28 of menstrual cycle.
Preclinical evidence suggests that neurosteroid ‘replacement’ is an effective and rational therapy for catamenial epilepsy.
In a pilot study, the synthetic neurosteroid ganaxolone was shown to be effective in women with catamenial epilepsy. Future studies are needed to confirm its efficacy.
Although ovarian hormones play a key role, the exact cause of catamenial epilepsy is unknown.
Estrogens, progesterone and neurosteroids play a crucial role, with hormone withdrawal being the critical factor.
Several AEDs are used for seizure therapy in women with epilepsy. However, catamenial seizures are not successfully treated currently with these conventional AEDs.
Based on progesterone's efficacy in catamenial epilepsy, orally active synthetic neuroactive steroids might provide a novel approach for catamenial epilepsy therapy.
Although there are three patterns of catamenial epilepsy, it is not clear if different patterns respond differentially to treatment options.
Future studies are clearly warranted to determine the specific role of neurosteroids in the pathogenesis of catamenial epilepsy
Future perspective
Studies on the frequency of catamenial epilepsy demonstrate the complexity of the condition and the difficulty of studying it. Although ovarian hormones play a key role, the exact cause of catamenial epilepsy is unknown. This knowledge is a prerequisite for the prevention of catamenial seizure exacerbation in women at risk. Experimental studies to this point have indicated a clear role of estrogen, progesterone and endogenous neurosteroids in the pathophysiology of catamenial seizure susceptibility. There is emerging evidence that neurosteroid withdrawal is a critical factor for enhanced seizure susceptibility during perimenstrual periods. However, there is a large gap in our understanding of how natural, cyclic variations in circulating estrogens and progesterone contribute to genesis of catamenial epilepsy. Several AEDs are used in catamenial epilepsy therapy. However, catamenial seizures are not successfully treated currently with these conventional AEDs. The AEDs used to control epilepsy may also affect a woman's hormones. Hormonal agents such as progesterone and neurosteroids may provide rational therapy for catamenial seizures.
Nevertheless, there is little information regarding whether catamenial seizures in humans really represent an epileptogenic process or are merely an exacerbation of existing seizure disorders. During menopause, approximately 40% of women report worsening of their seizure disorder, 27% report improvement and a third have no change [52]. Hormone replacement therapy is significantly associated with an increase in seizure frequency during menopause and this is more likely in women with a history of catamenial epilepsy. Based on progesterone's efficacy in catamenial epilepsy, orally active synthetic neuroactive steroids might provide a novel approach for catamenial epilepsy therapy. Although there are three patterns of catamenial epilepsy, it is not clear if different patterns respond differentially to treatment options. Future studies are clearly warranted to determine the specific role of neurosteroids in the pathogenesis of catamenial epilepsy.
Footnotes
Acknowledgement
This work was partly supported by a grant from the National Institute of Neurological Disorders and Stroke, National Institutes of Health (R21 NS052158). S Reddy has no conflicts of interest.