
Abstract
The prevalence of asthma in pregnant women appears to be increasing. Recent evidence demonstrates that pregnant asthmatic women with moderate-to-severe asthma may have an increased risk of adverse perinatal outcomes. The goal of asthma management during pregnancy is to optimize maternal and fetal health.
Asthma is the most common, potentially serious medical problem to complicate pregnancy. Recently, Kwon and colleagues reported that asthma affected 3.7–8.4% of pregnant women in the USA between 1997 and 2001 [1]. Pregnant asthmatic women have an increased risk of adverse perinatal outcomes [2,3], while controlled asthma is associated with reduced risks [4]. The two main goals of asthma management during pregnancy are to optimize maternal and fetal health while minimizing the side effects of drugs. This is an easier task if the patient's asthma is under good control prior to pregnancy. This article will present an overview on the management of asthma during pregnancy in both the chronic and acute setting.
Maternal respiratory physiological changes during pregnancy
The various physiological changes observed during pregnancy may alter the course of asthma in the pregnant asthmatic. Both the mechanical and hormonal changes of pregnancy can influence respiratory function. For example, as the uterus enlarges during pregnancy there is secondary elevation of the diaphragm, decreased diameter of the chest and an increase in abdominal pressure. These changes were thought to partially explain the decrease in expiratory reserve volume (ERV), residual volume (RV) and functional residual capacity observed in late pregnancy. Meanwhile, physiological tests of large-airway function including forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC), FEV1:FVC ratio, mean forced expiratory flow during the middle half of forced vital capacity (FEF 25–75%), and peak expiratory flow rate remain unaffected by pregnancy [5,6]. Not only are these physiological measures useful indicators of asthma control, they are also helpful in differentiating dyspnea caused by asthma from dyspnea caused by hyperventilation or pressure on the diaphragm with late pregnancy.
Approximately 30–40% of women with asthma who visit outpatient clinics report peri-menstrual worsening of symptoms [7]. The likelihood that female sex hormones influence asthma symptoms in this condition seems obvious. Since female sex hormones increase 100–1000-times over the level found in nonpregnant females, their role in influencing asthma during pregnancy is also likely [8]. What is less clear are the underlying mechanisms through which these hormones influence asthma symptoms.
Progesterone, estrogens or both are the most frequently implicated hormones, but cortisol and prostaglandins (PGs) may also be important. Considerable evidence suggests that female sex hormones have effects on several cells and cytokines involved in inflammation. Specifically attributed to estrogens are increases in B-cell differentiation, decreases in T-cell suppressor activity and numbers, and increases in antibody (immunoglobulin [Ig]G) production [7]. There is less evidence documentating the effects of progesterone on inflammation. Evidence suggests that progesterone can act as a partial glucocorticoid agonist and suppress histamine release from basophils [7]. Both estrogen and progesterone are involved in eosinophilic infiltration in many organs including the uterus [8], and both can reduce the oxidative burst after phagocytic stimuli [7]. Estradiol enhances eosinophilic adhesion to human mucosa microvascular endothelial cells and the combined effect with progesterone induces eosinophil degranulation [7].
Maternal plasma cortisol levels increase with pregnancy. This includes both free and total cortisol levels [9]. Since a greater amount of free cortisol is available during pregnancy, one might expect both improvement in asthma control and reduced steroid requirement in pregnant asthmatics. However, it appears that cortisol's effects on asthma during pregnancy are more variable.
Several PGs could affect asthma, as bronchodilators (PGE2) and bronchoconstrictors (PGD2 and PGF2). During pregnancy, amniotic fluid contains a mixture of these PGs. There is a 10–30-fold increase in PGF2-α during pregnancy and its levels have been found to correlate with estrogen levels. Asthmatic patients appear to be more sensitive to the bronchoconstrictive properties of aerosolized PGF2-α than unaffected individuals [9]. However, a relationship between increased levels of PGF2-α during labor and asthma exacerbations in the pregnant patient has never been established.
Effect of pregnancy on asthma
The course of asthma may worsen, improve or remain unchanged during pregnancy, and the overall data suggest that these various courses occur with approximately equal frequency [10–13]. Schatz and colleagues reported the effects of pregnancy on asthma and related asthma morbidity during pregnancy to asthma severity in early pregnancy [14]. They observed that asthma morbidity (hospitalizations, unscheduled office or emergency department visits and oral corticosteroid use) correlated closely with the asthma severity classification applied to the subjects at entry; for example, those subjects with mild asthma experienced fewer hospitalizations, unscheduled visits, oral corticosteroid courses and total exacerbations than those with moderate-to-severe asthma.
Exacerbations of asthma during pregnancy appear to be more frequent at 24–36 weeks' gestation, and general improvements in asthma symptoms have been observed during the last 4 weeks of pregnancy [15]. Only approximately 10–20% of women developed an exacerbation of asthma during labor and delivery [14].
In a review by Kwon and colleagues, the authors questioned whether pregnancy and stage of pregnancy influence maternal asthma severity [16]. In 54 pregnant women with asthma, bronchial hyper-responsiveness to methacholine improved between preconception and pregnancy in 69% of subjects. This improvement peaked in the second trimester, reverted after delivery, and was greatest among those women who were most hyper-responsive initially. Lung function also showed a nonsignificant trend towards improvement during pregnancy.
One observation that may be mechanistically and clinically important is that there is a significant concordance between the course of rhinitis and the course of asthma during pregnancy. One study found that women who experienced improvement in asthma symptoms during pregnancy also showed improvement in rhinitis symptoms [12]. Exacerbations appeared to be more frequent between 24–36 weeks' gestation, and general improvements in asthma symptoms were observed during the last 4 weeks of the pregnancy. Only approximately 10–20% of women developed an exacerbation of asthma during labor and delivery [14,15].
The mechanisms responsible for the altered course of asthma during pregnancy are unknown. As previously described, the multiple biochemical and physiological changes during pregnancy could potentially ameliorate or exacerbate gestational asthma [10,11]. In addition, exposure to fetal antigens, leading to alterations in immune function, may predispose some pregnant asthmatics to worsening asthma [17].
There is also the possible influence of fetal sex on maternal asthma during pregnancy. Several reports have suggested that increased asthma symptoms or airway lability were associated with the presence of a female fetus [18–21]. However, the mechanisms leading to changes in asthma during pregnancy in the presence of a female fetus require further investigation. An interesting hypothesis regarding the relationship between mother, placenta and female fetus is that there may be abnormal levels of a placental enzyme that may lead to reduced fetal growth in female infants of pregnant asthmatic women [18].
Effect of asthma on pregnancy
Controlled studies that have evaluated outcomes of pregnancy in asthmatic compared with nonasthmatic women have suggested that maternal asthma may increase the risk of perinatal mortality, pre-eclampsia, low-birthweight infants and preterm births compared with nonasthmatic pregnant women [18,22–24].
It is unclear whether these adverse outcomes are related to hypoxia and other physiological consequences of poorly controlled asthma, medications used to treat asthma, or pathogenic or demographic factors associated with asthma, but not actually caused by the disease or its treatment.
Several observations do support the hypothesis that uncontrolled asthma increases perinatal risks while controlled asthma reduces these risks. For example, patients with daily asthma symptoms have been shown to have an increased risk of intrauterine growth retardation and pre-eclampsia [25]. Several studies have demonstrated that better-controlled asthma (defined by lack of acute episodes or higher maternal pulmonary function) led to improved intrauterine growth (measured by birthweight or ponderal indices) [22,26].
In one of the first studies to determine pregnancy outcomes stratified by asthma severity (as classified by the National Asthma Education Program) [2], Dombrowski and colleagues conducted a multicenter, prospective, observational cohort study involving 16 centers between 1994 and 1999 [27]. Of all outcomes explored (including preterm delivery, gestational diabetes, pre-eclampsia, preterm labor, chorioamnionitis, oligohydramnios, cesarean delivery, low birthweight, small for gestational age and congenital malformations), only cesarean delivery rates were increased in the group of moderate-to-severe asthmatics.
Asthma management during pregnancy: nonpharmacological
The general principles of asthma management during pregnancy do not differ substantially from the management of nonpregnant asthmatics. The ultimate goal for the pregnant asthmatic is to have no limitation of activity, minimal chronic symptoms, no exacerbations, normal pulmonary function and minimal adverse effects of medications. Patient education is more important than ever during pregnancy. The patient must understand the potential adverse effects of uncontrolled asthma on the wellbeing of the fetus and that treating asthma with medications is safer than increased asthma symptoms that may lead to maternal and fetal hypoxia.
Objective assessments and monitoring should be performed on a monthly basis. Such assessments should include pulmonary function testing (ideally spirometry), detailed symptom history (symptom frequency, nocturnal asthma, interference with activities, exacerbations and medication use) and physical examination, paying specific attention to auscultation of the lungs.
The patient should also understand how she can reduce her exposure to or control those factors that exacerbate her asthma. Avoidance of asthma triggers such as animal dander, tobacco smoke and pollutants is important since exposure may lead to increased asthma symptoms and, potentially, the need for more medication.
Most importantly, there should be open lines of communication with the patient's obstetrician. Obstetricians should be involved in asthma care and should obtain information on the patient's asthma status during prenatal visits.
Choice of specific medications during pregnancy
There is limited information regarding the safety of commercially available asthma medications in pregnant women. In 1993, the National Asthma Education and Prevention Program (NAEPP) published the Report of the Working Group on Asthma and Pregnancy, which reviewed the data from available studies and presented recommendations for the pharmacological management of asthma during pregnancy [28]. An update of this report has recently been published: NAEPP Working Group Report on Managing Asthma During Pregnancy: Recommendations for Pharmacologic Treatment – Update 2004 [29].
Inhaled corticosteroids
Concern has been raised regarding a possible adverse effect of inhaled steroids on perinatal outcomes including intrauterine growth. Much of the information available regarding the safety of various asthma medications includes data from large cohort studies. For instance, one of the largest cohorts of pregnant asthmatics comes from the Swedish Medical Birth Registry. In a recent report, Norjavaara and Gerhardsson de Verdier searched for an association between inhaled budesonide use in 2968 women during pregnancy and adverse perinatal outcomes [30]. These women gave birth to infants of normal gestational age, birth weight and length, with no increased risk of still births or multiple births. An earlier study from this cohort did not find an association between maternal budesonide use and total or specific congenital malformations [31].
Using information obtained from the Registry for Allergic and Asthmatic Pregnant Patients of the American College of Allergy Asthma and Immunology (IL, USA) and the American Academy of Allergy Asthma and Immunology (WI, USA), Namazy and colleagues identified no significant relationship between specific inhaled steroid use or the dose of inhaled steroid used and the incidence of small for gestational age infants or mean bithweight reductions [32].
Schatz and colleagues evaluated over 2000 subjects from 16 centers of the National Institute of Child Health and Human Developmental Maternal Fetal Medicine Units Network (MD, USA) [33]. No significant relationships were found between adverse perinatal outcomes and the use of inhaled β-agonists, inhaled corticosteroids (ICSs), theophylline or cromolyn–nedocromil. There was an observed increased risk of preterm and low-birthweight infants associated with oral corticosteroid use. Similar results were reported in a recent study by Bakhireva and colleagues [34]. Although infants of the women receiving ICSs during pregnancy did not have a lower birthweight compared with those of the control subjects, there was a significant decrease in birthweight in the pregnant women receiving systemic steroids compared with controls without asthma and exclusive β2-agonist users.
Dombrowski and colleagues recently performed a prospective, double-blind, double placebo-controlled, randomized clinical trial comparing the efficacy of inhaled beclomethasone diproprionate with oral theophylline for the prevention of asthma exacerbations during pregnancy [35]. Results demonstrated that there was no significant difference in the proportion of asthma exacerbations among the 194 women in the beclomethasone cohort versus the 191 women in the theophylline cohort. However, there were fewer reported side effects, a lower rate of discontinuation of medication and a lower proportion of women with a FEV1 of less than 80% in the beclomethasone dipropionate treatment group. This study supports previous guidelines that ICSs are the therapy of choice for persistent asthma during pregnancy.
Recent data from another large, population-based case–control study in Canada addressed whether ICSs increased the risk of either pregnancy-induced hypertension or pre-eclampsia in asthmatic women [36]. In a group of over 3000 women, the authors found that while oral corticosteroids were significantly associated with pregnancy-induced hypertension, using ICSs during pregnancy was not associated with either pre-eclampsia or pregnancy-induced hypertension. In addition, there was no observed dose–response relationship with ICSs and either of these conditions.
A review of recent publications supports the overall safety of ICS use in pregnancy, with most data supporting the safety of inhaled budesonide. Thus, in the current guidelines, budesonide is considered the inhaled steroid of choice during pregnancy [29]. However, there are no data to suggest that other inhaled steroids are less safe during pregnancy. Thus, if a pregnant asthmatic woman is using an alternative inhaled steroid prior to pregnancy and her asthma is well controlled, it would not be unreasonable to continue it throughout the pregnancy.
Oral corticosteroids
As noted previously, data regarding the use of systemic corticosteroids during pregnancy have not been totally reassuring. Recent available human studies include a meta-analysis of six cohort studies by Park-Wyllie and colleagues evaluating the relationship between corticosteroid use during pregnancy and total congenital malformations, and four case–control studies evaluating the potential relationship between systemic corticosteroid use during pregnancy and oral clefts [37]. They found that while there was no unequivocal increase in the risk of total congenital malformations, there was a statistically significant increased risk of oral clefts in infants of mothers treated with corticosteroids during the first trimester (summary odds ratio [OR]: 3.35; 95% confidence interval [CI]: 1.97–5.69).
Other adverse outcomes recently associated with systemic corticosteroid use during pregnancy include pre-eclampsia, low birthweight and preterm delivery [37–39]. However, the available data make it difficult to separate the effects of the corticosteroids on these outcomes from the effects of severe or uncontrolled asthma. It must be stressed that the potential risks of oral corticosteroid use during pregnancy must be balanced against the risks to both the mother and infant of poorly managed severe disease, which include maternal mortality or fetal mortality, or both [29]. The current recommendations continue to support the use of oral corticosteroids, when indicated, for the long-term management of severe asthma or for severe exacerbations during pregnancy [29].
Short-acting bronchodilators
There is no evidence of any association between the use of inhaled short-acting β-agonists in pregnant women and an increased risk of congenital malformations or other adverse perinatal outcomes [13,38,40]. Currently, albuterol is recommended as the inhaled short-acting β-agonist of choice during pregnancy [29].
Long-acting β-agonists
Two long-acting inhaled β-agonist bronchodilators are available – salmeterol and formoterol. There are limited published data regarding the safety of these drugs during pregnancy [41,42]. The new guidelines recommend salmeterol as the long-acting β-agonist of choice during pregnancy due to greater availability in the USA [29].
Other medications
Nebulized ipratropium has been recommended for use in women presenting with acute asthma who do not improve substantially with the first treatment of inhaled β-agonists. Since 1993, there have been no further published data on anticholinergics in pregnancy, but this recommendation is maintained in the updated guidelines [29]. Other medications are recommended only as alternative, but not preferred, choices during pregnancy. These include cromolyn (for mild, persistent asthma), theophylline (for mild, persistent asthma or as add-on therapy to ICSs) and zafirlukast or montelukast (for mild, persistent asthma or as add-on therapy to ICSs). It is important to note that the serum concentrations of theophylline need to be closely monitored and low-dose therapy is recommended, with maintenance serum levels targeted at 5–12 μg/ml.
Pharmacological step therapy during pregnancy
Many pregnant asthmatic women require medications to control their asthma. Current guidelines recommend a generalized stepwise approach to achieving and maintaining asthma control (Table 1). The number and dose of medications used are increased as necessary and decreased when possible. Decreasing doses should be performed carefully, since this may lead to an exacerbation of symptoms. Current guidelines suggest that it may be prudent to postpone attempts at reducing therapy that is effectively controlling the patient's asthma until after the birth.
Stepwise approach to managing asthma during pregnancy and lactation.
Based on the recommendations of the National Asthma Education Program Report of the Working Group on Asthma During Pregnancy Update (2004) [13].
More published human data using albuterol during pregnancy than using other short-acting β-agonists.
More data on using budesonide than on using other inhaled corticosteroids.
Maintain to serum concentration of 5–12 μg/ml.
Salmeterol is considered the long-acting β-agonist of choice during pregnancy due to greater availability in the USA.
Management of acute exacerbations of asthma during pregnancy
A recent large, multicenter study reported that 20% of women with persistent asthma experience an unscheduled (emergency department or physician) visit for asthma during pregnancy, and 8% required hospitalization [14]. Such exacerbations can compromise fetal wellbeing; therefore, aggressive home management of acute symptoms needs to be reviewed with pregnant asthmatic patients. Above all, pregnant asthmatic patients should be taught to recognize the early signs and symptoms of exacerbations. The current recommendations for home (Figure 1) and emergency department (Figure 2) management of asthma exacerbations in pregnant asthmatic women are not different than previously published Expert Panel Report-2 recommendations in nonpregnant asthmatic women [43]. However, fetal assessment is an important additional aspect of the management of acute asthma exacerbations during pregnancy. Patients should be instructed to be attentive to fetal activity. Some women may benefit from additional evaluation of fetal activity and growth by serial ultrasound examinations.
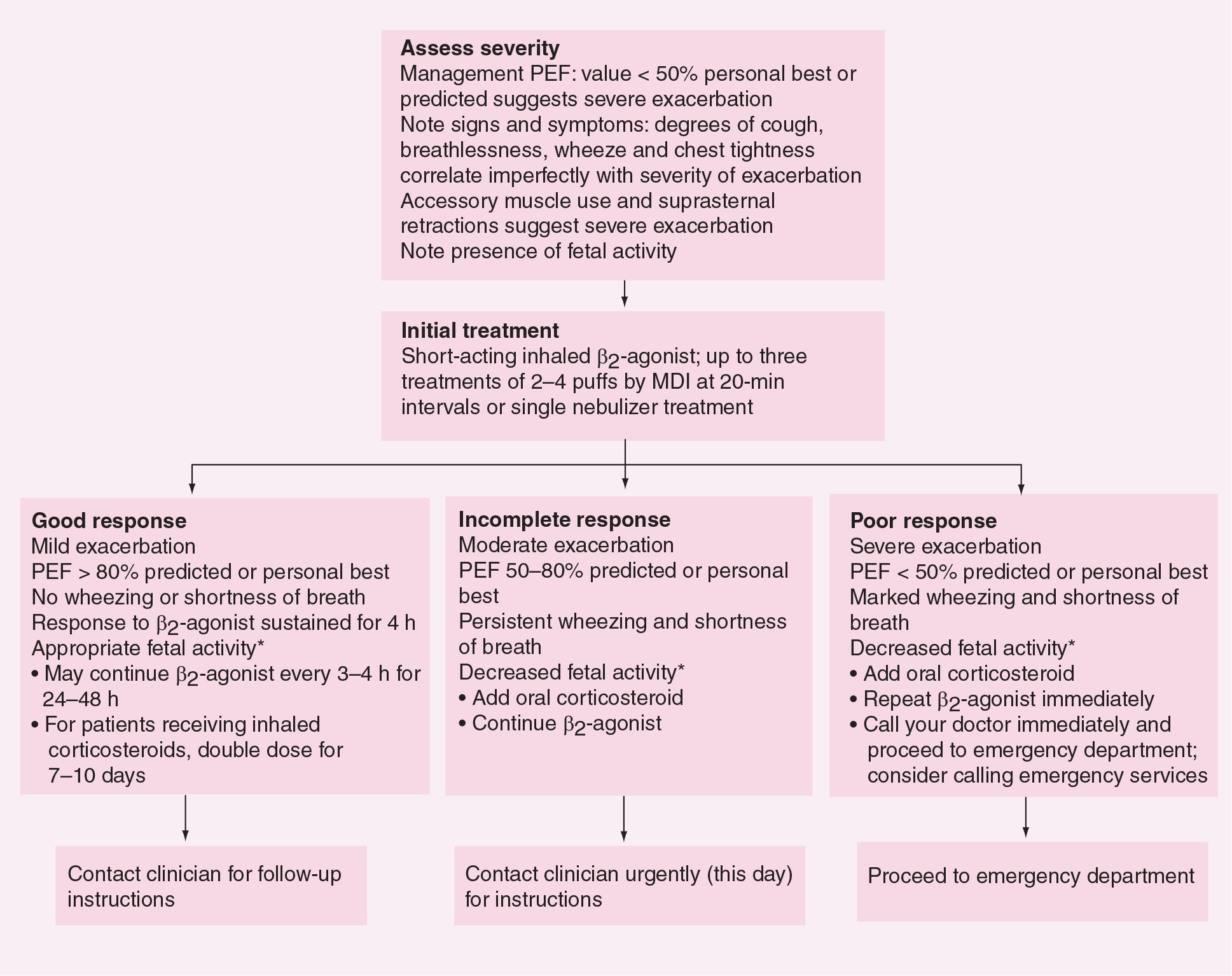
Management of asthma exacerbations: home treatment.

Management of asthma exacerbations: emergency department and hospital-based care.
Conclusion
Managing asthma in pregnant asthmatic women can be challenging. The main goals of asthma management during pregnancy are to optimize maternal and fetal health. It is clear that the risk of uncontrolled asthma greatly outweighs the risk of recommended asthma medications. Hopefully, the guidelines presented will be a helpful resource in the treatment of pregnant asthmatic patients.
Future perspective
Asthma specifically appears to be undertreated in pregnant women. Among women presenting to the emergency department with acute asthma, pregnant asthmatics are less likely to receive appropriate treatment with corticosteroids [44]. Another recent study concluded that asthma is undertreated in women before and during pregnancy [45]. Part of the reason for this under-treatment is undoubtedly inadequate information regarding the safety of asthma therapy during pregnancy. Over the past few years, there have been further insights regarding to the mechanisms involved and the treatment of asthma during pregnancy. However, there is a need for larger studies that will help answer the lingering questions regarding safety of asthma medications during pregnancy. A comprehensive surveillance system for asthma and allergy medications during pregnancy would be helpful to assess the safety of all currently used asthma and allergy medications during pregnancy. In addition, it would be valuable as newer classes of asthma medications become available.
Executive summary
Asthma affects between 3.7–8.4% of pregnant women in the USA.
Asthma course worsens in a third, improves in a third, and remains unchanged in a third of women during pregnancy.
Pregnant asthmatic women have an increased risk of perinatal mortality, pre-eclampsia, low-birthweight infants and preterm births compared with nonasthmatic women.
Uncontrolled asthma increases perinatal risks, while controlling asthma reduces these risks.
Objective assessments and monitoring including pulmonary function testing (ideally spirometry), detailed symptom history and physical examination should be performed on a monthly basis in pregnant asthmatic women with persistent asthma.
In patients starting inhaled corticosteroids during pregnancy, budesonide has been recommended as the inhaled corticosteroid of choice.
Current guidelines recommend a stepwise approach to achieving and maintaining asthma control with medications during pregnancy.
Asthma apppears to be undertreated in pregnant women, especially with regard to the use of corticosteroids during pregnancy.
Larger studies will help answer the lingering questions regarding the safety of asthma medications during pregnancy.
A comprehensive surveillance system for asthma and allergy medications during pregnancy would be helpful in assessing the safety of currently used medications during pregnancy.