
Abstract
Recognition of cardiovascular disease as the leading healthcare threat to women continues to shape the prioritization of efforts to more effectively diagnose and treat heart disease in women. At its inception almost 8 years ago, the National Heart, Lung and Blood Institute in the USA sponsored the Women's Ischemia Syndrome Evaluation (WISE) study, aiming to optimize symptom evaluation and diagnostic testing for ischemic heart disease in women and to explore pathophysiologic mechanisms for symptoms and myocardial ischemia in the absence of epicardial coronary artery stenosis. The WISE study has investigated the spectrum of anginal symptoms, diagnostic strategies for micro- and macrovascular coronary disease, and the role of psychosocial variables and reproductive hormones in ischemic heart-disease presentation. One of the pivotal WISE findings sheds light on chest pain in the absence of significant obstructive epicardial luminal coronary stenosis, otherwise known as Cardiac Syndrome X. In the WISE study, using coronary vasomotor testing during angiography, investigators observed prevalent abnormalities in coronary flow reserve, suggestive of microvascular coronary dysfunction in relation to adverse morbidity and mortality among these women. Findings such as these from the WISE study have significantly added to the current management approach to heart disease in women.
Keywords
Over the last decade, three clinical paradoxes relating to women and heart disease have been recognized. First, despite having more symptoms of heart disease, women have less obstructive angiographic coronary artery disease (CAD) compared with men. Second, women with obstructive CAD have less typical symptoms of heart disease and, third, women with obstructive CAD have poorer outcomes compared with men. The Women's Ischemia Syndrome Evaluation (WISE) study is an ongoing project of the National Heart, Lung and Blood Institute (NHLBI), designed to further our understanding with regard to these clinical paradoxes. The WISE study was aimed at developing and evaluating innovative diagnostic modalities with the goal of improving the diagnostic reliability of cardiovascular testing in the evaluation of ischemic heart disease (IHD) in women, and developing safe, efficient and cost-effective new diagnostic approaches. The WISE study also explored the role of a specific pathophysiology, inflammatory mechanisms modulated by reproductive hormones, along with the renin–angiotensin system, in relation to IHD processes in women. The WISE study highlights the challenges and dilemmas facing physicians and patients in the accurate recognition and management of IHD in women, including unique pathophysiology and symptomology, diagnostic testing and novel associations between heart disease, reproductive hormones and psychosocial variables. The following article reviews some of the findings from the WISE study.
The WISE study
The WISE study is a prospective, multicenter, cohort observational study. Women undergoing coronary angiography for chest pain or symptoms suggestive of myocardial ischemia were enrolled in the WISE study from four major academic medical centers in the USA from 1996 to 2000. A total of 936 women between the ages of 18 and 83 years were enrolled and underwent collection of demographic, medical and psychosocial histories, a complete physical examination and clinically indicated coronary angiography. Qualitative and quantitative coronary-angiography analysis was performed by an experienced core laboratory directed by an interventional cardiologist. Women were prospectively followed for cardiovascular outcomes, which included hospitalization for angina, nonfatal myocardial infarction (MI), stroke and cardiovascular-event-related death. The unique feature of the study is that, in addition to a common protocol for all sites, each site had a specific protocol, employing site-based expertise complementing the evaluation of ischemia. These tests focused on physiologic and functional cardiac assessments, including magnetic resonance imaging (MRI), positron emission tomography (PET), myocardial contrast echocardiography, stress echocardiography, coronary flow reserve, coronary vasomotor testing and exercise stress electrocardiography.
The WISE study represents the largest exclusively female cohort with detailed core laboratory-interpreted coronary angiographic data. The mean age at enrollment was 58 ± 12 years with a relatively high representation of minorities (19%). The majority of the women were postmenopausal (85%) and had at least one cardiac risk factor: 60% reported a history of hypertension, 55% had dyslipidemia, 25% had diabetes, 20% were active smokers and 60% reported a positive family history of premature heart disease.
Multiple ancillary WISE studies are currently ongoing, including an extension study further exploring the relationship between metabolic and microvascular ischemia, endothelial dysfunction and its modulation by female hormones. In addition, this extension study aims to quantify disability, morbidity, mortality and the financial impact of heart disease on women and their healthcare resource consumption.
WISE & angina
Symptoms of angina have typically been described to correlate with obstructive angiographic CAD, reflecting altered supply-and-demand physiology within the myocardial macrocirculation. Women, unless diabetic, were thought to be at low risk. More contemporary views denote the presence of typical and atypical chest-pain symptoms in men and women with variable degrees of angiographic CAD and involvement of the coronary macro- and micro-circulation. It has been demonstrated that chest pain in women is less likely to be associated with flow-limiting obstructive coronary stenosis than chest pain in men [1], yet women continue to have poor associated cardiovascular outcomes when compared with men.
The WISE study data suggest that women with obstructive CAD tend to have less typical signs and symptoms of angina [2]. In comparison to traditional typical angina characteristics, WISE angina variables that correlated with significant angiographic CAD in women were arm or shoulder pain without neck pain or palpitations [101]. Additional WISE study reports demonstrated that the traditional classification of the typical angina, atypical angina and nonanginal chest-pain model to predict CAD is only weakly related to angiographic CAD prevalence in WISE study women. A history of typical angina in WISE study women predicted angiographic CAD in less than half, demonstrating that typical chest-pain symptoms alone are not as sensitive in women as previously thought. When these same criteria were applied to women younger than 55 years, a history of typical angina was no better than chance at predicting CAD [5]. Thus, chest pain itself was not an adequate predictor of significant CAD, highlighting the need for a more sensitive diagnostic algorithm in women.
To improve the diagnostic accuracy of chest pain in women, models that incorporate additional variables, such as inflammatory cardiac markers, noninvasive testing and reproductive status may be necessary. Ongoing WISE efforts are focused on developing a more reliable chest-pain assessment tool specifically designed to risk-stratify women with chest pain.
WISE, angiographic coronary artery disease & microvascular ischemia
It is estimated that approximately 25–40% of women who undergo coronary angiography for evaluation of ischemia have ‘normal’ coronary arteries [3]. Normal (no visible disease on angiography) or nonobstructive (defined as coronary luminal stenosis <50%) CAD is present in 10–25% of women presenting with acute coronary syndrome and ST-segment elevation MI (STEMI) compared with 6–10% in men [4]. Women with chest pain and without obstructive CAD (Cardiac Syndrome X) pose both a special diagnostic and therapeutic challenge. Furthermore, in the WISE study, the prognosis of ‘normal’ coronary angiogram in the setting of angina is not as benign as initially thought [5].
Despite the high prevalence of cardiac risk factors, only 40% of WISE women had obstructive angiographic CAD (luminal obstruction ≥50%). Patients with chest pain and nonobstructive CAD underwent further provocative ischemic testing during angiography. Interestingly, many had significant microvascular ischemia, defined as a diminished coronary-flow velocity reserve (CFVR) of less than 2.5 in response to intra-coronary adenosine. CFVR and other risk factors for atherosclerosis were measured in 159 WISE women with chest pain and nonobstructive CAD [6]. A total of 47% of women had diminished CFVR (<2.5), suggestive of microvascular dysfunction. Demographic characteristics, blood pressure, ventricular function, lipid levels and reproductive hormone levels did not differ between women with or without microvascular dysfunction. These findings support the concept that microvascular ischemia associated with sub-endocardial hypoperfusion plays an important role in women with chest pain and nonobstructive angiographic CAD, and that microvascular dysfunction is not predicted by traditional risk factors for CAD and hormone levels.
Furthermore, WISE data demonstrated that patients with microvascular dysfunction and nonobstructive CAD have a relatively poor prognosis compared with women without evidence of microvascular dysfunction and nonobstructive CAD [5,7]. Comparing women with and without microvascular dysfunction, those with microvascular ischemia were at a significantly increased risk of a cardiovascular event over the next 3 years (87 vs 57%; p < 0.01). Over 40% of these patients were rehospitalized for chest pain more than once, while 30% underwent repeat angiography over the 1–5 year follow-up period and were at a twofold increased risk for major cardiovascular events. These findings underscore the need for accurate recognition and availability of treatment modalities targeted towards microvascular ischemia. This includes a need for further studies to improve our understanding of the pathophysiology and derangements of microvascular dysfunction.
Finally, the WISE study demonstrated the safety, feasibility and reliability of CFVR response to adenosine as a tool to measure microvascular function, and its potential clinical application for working up patients with Cardiac Syndrome X. Of note, microvascular dysfunction may be heterogeneously distributed in the myocardium, and assessment of CFVR in a single coronary vessel may not allow for accurate assessment [8].
Patients and clinicians are often mutually frustrated by situations where the patient continues to experience chest pain and the physician continues to reassure the patient due to ‘normal’ coronary angiography results. These cases may require development and implementation of careful treatment plans and options. A practical algorithm for the management of patients with symptoms and nonobstructive CAD is shown in Figure 1 [9]. Awareness of microvascular dysfunction as a true disease entity and a possible diagnosis should allow us to better manage these challenging patients.
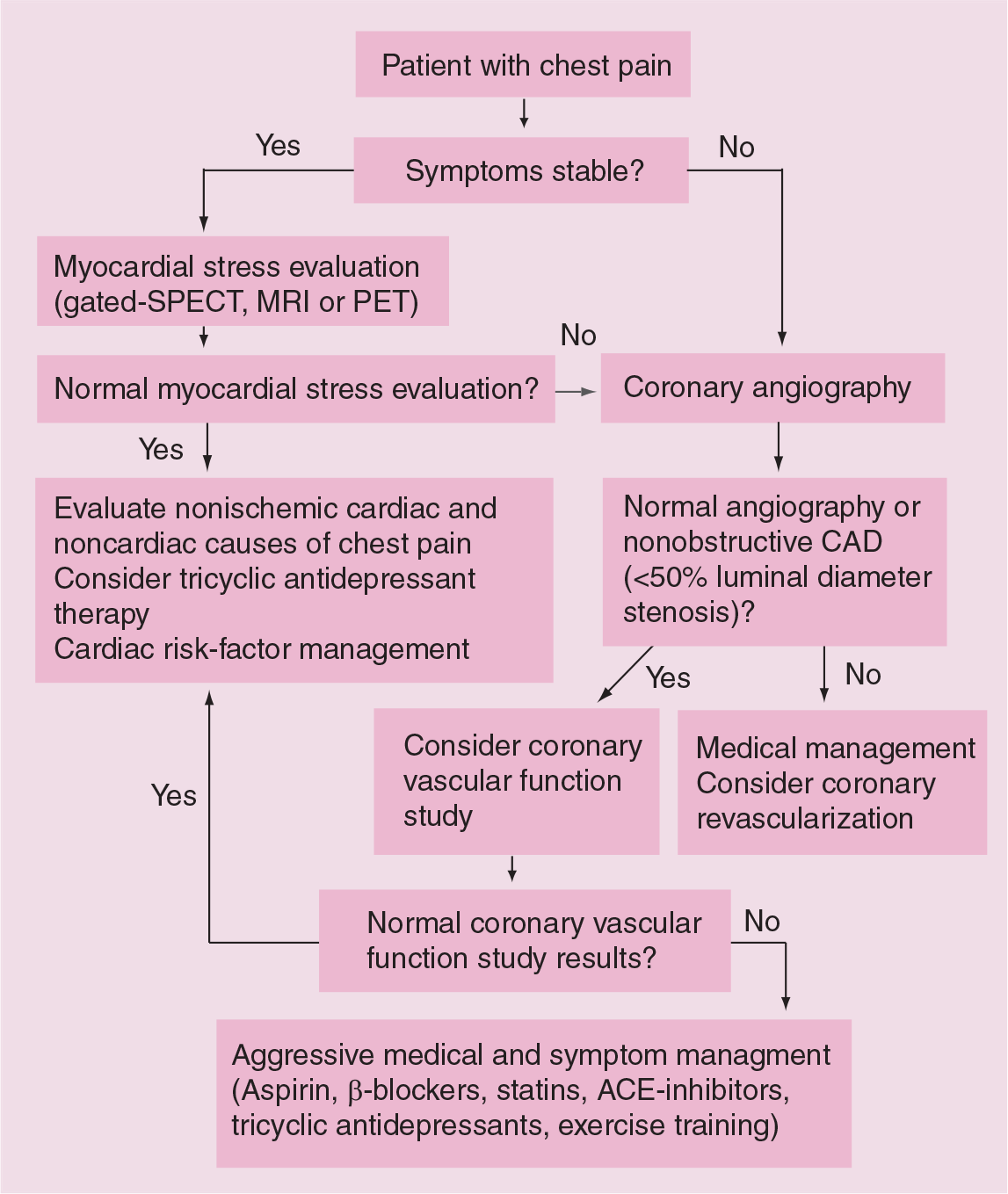
Algorithm for the management of patients with symptoms and nonobstructive coronary artery disease.
WISE & diagnostic modalities for macro-& microvascular myocardial ischemia in women
Better understanding of gender differences in the manifestation and detection of myocardial ischemia is a critical initial step to improve cardiovascular health and outcomes in women. The absence of reliable diagnostic tools for myocardial ischemia in women has enormous consequences on morbidity, mortality and healthcare costs. Recent estimates suggest that of the 800,000 left-heart catheterizations performed in the USA, 40% are performed on women [102]. Given that up to 50% of these women will show nonobstructive CAD, the need to effectively work up chest-pain symptoms in women becomes of paramount importance.
As options for diagnostic testing for myocardial ischemia evolve, it is important to consider sex-related differences for optimal evaluation of ischemia in women and its prognostic implications. In general, exercise electrocardiogram (ECG) testing and stress echocardiography have lower overall predictive values and offer less accurate prognostic values in women than men [10–13]. WISE investigators evaluated the utility of the exercise treadmill test (ETT) for detecting CAD in 113 women. The sensitivity of ETT for detection of CAD was 33% and the specificity was 86% [14]. While the sensitivity of ETT in women was known to be low, the preserved specificity may reflect the impact of post-test bias in previous studies. In addition, WISE data suggest that, although dobutamine stress echo (DSE) reliably predicts multivessel stenosis in women with suspected CAD, it is usually normal in women with single-vessel disease or those with evidence of microvascular or endothelial dysfunction [15].
The WISE study also examined the use of cardiac magnetic resonance (CMR) and advanced myocardial perfusion variables to improve diagnostic and prognostic assessment. One of the promising diagnostic approaches evaluated in the WISE study is 31P nuclear magnetic resonance (NMR) spectroscopy; targeting changes between rest and stress concentrations of 31P-determined metabolites (e.g. phosphocreatine [PCr], ATP and inorganic phosphate) and intracellular pH as a measure of microvascular ischemia. A decrease in the myocardial PCr–ATP ratio in response to isometric hand-grip stress in women with chest pain and nonobstructive angiographic CAD was consistent with microvascular disease. The WISE trial studied 35 women hospitalized with chest pain and nonobstructive angiographic CAD with 31P-NMR before, during and after isometric hand-grip exercise to measure myocardial high-energy phosphates [16]. A total of 20% of these women had a decrease in the measured PCr–ATP ratio during exercise, reflecting abnormal myocardial metabolism on 31P-NMR. Those with abnormal 31P-NMR were at increased risk of rehospitalization for unstable angina, repeat coronary angiography and increased healthcare costs [5].
Findings from the WISE study highlight the strengths and limitations of current noninvasive testing for myocardial ischemia in women. Tools that reliably diagnose microvascular ischemia, such as CMR, will help identify and cost-effectively treat women with this ubiquitous disorder. Current recommendations support the use of myocardial perfusion imaging testing as the preferred noninvasive method of evaluating women for micro- and macrovascular ischemia.
WISE & psychosocial variables
The interplay between psychosocial variables such as stress, anxiety, and depression and heart disease is well known [17]. Prior reports have not characterized their role in women with obstructive and nonobstructive angiographic CAD.
WISE women with CAD risk factors were noted to have a consistent and clinically relevant association with psychosocial variables, including depression, hostility and anger expression [18]. Olson and colleagues reported a direct relationship between higher Beck depression index scores and obstructive CAD on angiography in 406 WISE study women [19]. These women were also noted to have lower Duke activity status inventory scores, possibly supporting the relationship between depression, a less active lifestyle and CAD. In another subgroup analysis, using the Cook–Medley inventory score reflecting cynicism, hostility and aggression, women with higher hostility scores were more likely to be at increased risk of a cardiovascular event [20]. On further comparison of women with and without obstructive angiographic CAD with normal controls, expression of anger and hostility conferred an increased risk of obstructive angiographic CAD. Interestingly, WISE study women reporting a history of anxiety disorder were noted to be less likely to have angiographic CAD [21]. Whether anxiety provokes more chest-pain symptoms, leading to cardiac catheterization at relatively lower CAD risk levels, could not be elucidated in a patient cohort enrolled with chest pain.
As we further define these relationships, findings suggest that it may be important to incorporate an assessment of psychosocial risk factors into clinical practice. Prospective studies should address whether treatment of psychosocial variables will have a significant impact on the morbidity and mortality related to CAD.
WISE & reproductive hormones
Hormone replacement therapy (HRT), once thought to be cardioprotective, is no longer indicated for primary or secondary prevention of heart disease in postmenopausal women [22]. There are data to support the cardiovascular protective effects of estrogen through various mechanisms. However, the disparity between these data and the results of recent clinical trials suggests that crucial pieces of knowledge are lacking.
A total of 85% of WISE study women were postmenopausal and 40% used HRT. Currently, there is no significant relationship between HRT use and cardiovascular outcomes in WISE women. However, WISE data demonstrated that, when compared with minority women, Caucasian women receiving HRT had fewer symptoms of depression, lower aggression scores and overall better psychologic health. This effect was not found in the African–American population, highlighting a race-specific HRT effect [23].
The WISE study also evaluated estrogen deficiency and its possible relationship with premature CAD in premenopausal women [24]. Of the 95 premenopausal women not taking exogenous hormones enrolled in the WISE study, those with obstructive angiographic CAD (14%) had significantly lower serum estradiol (E2), bioavailable estradiol (bioE2) and estrone (E1) levels with low follicle-stimulating hormone (FSH) levels (<10) compared with premenopausal women without obstructive CAD. This hypoestrogenemia appeared to be mediated by the hypothalamus, consistent with prior primate studies of environmental stress-induced hypothalamic hypoestrogenemia with anovulatory cycling. Hypothalamic hypoestrogenemia was significantly more prevalent among women with CAD than those without CAD (9/13 [69%] vs 24/82 [29%]; p = 0.01). Psychosocial stress was an independent predictor of hypoestrogenemia and a biobehavioral link between psychosocial stress-induced hypoestrogenemia and CAD is plausible. Whether the stress of angiography or the current chest-pain episode was responsible for transient hypothalamic hypoestrogenemia remains a possible confounding explanation. This new finding offers insight into the third paradox of more adverse outcomes in women [25,26] and provides a platform to possibly develop new, sex-specific hormonal treatments for CAD. A WISE ancillary study is ongoing to specifically study the above hypothesis in young, premenopausal women undergoing angiography.
The interplay between reproductive hormones and physiologic and pathologic disease processes continues to evolve. The above findings from the WISE study reinforce the need for continued research studying the role of reproductive hormones and their effects on diseased and healthy vascular endothelium in pre- and postmenopausal women.
Other WISE findings
The metabolic syndrome has been closely linked to CAD [27–29]. The metabolic syndrome is an intermediate between normal glucose homeostasis and diabetes and is associated with increased cardiovascular risk. Characteristics of the metabolic syndrome, which result from insulin resistance, include glucose tolerance, dyslipidemia, hypertension and abdominal obesity. Although each of these traits are risk factors for atherosclerosis, the clinical constellation comprising the metabolic syndrome is associated with increased cardiovascular risk independent of these contributing factors [28].
In the WISE study, 25% of women had the metabolic syndrome, and 4-year event-free and overall survival was significantly lower in these women [30]. Moreover, angiographic CAD was found to be a stronger predictor of 4-year cardiovascular event risk when associated with the metabolic syndrome [31]. The prevalence of significant angiographic CAD and incidence of major adverse cardiovascular events increases in a gradient manner across the continuum of metabolic status, from normal, to the metabolic syndrome, to diabetes, in women with suspected ischemia.
When compared with obesity, body mass index and the metabolic syndrome were closely associated; however, only the metabolic syndrome conferred a twofold increased risk of death or a major cardiovascular event. These findings suggest that, although weight loss should be stressed, the role of insulin resistance and the metabolic syndrome should be at the center of treatment goals.
Anemia has also been linked to worsening outcomes in women. Anemia in patients presenting with acute MI or heart failure has frequently been associated with adverse outcomes. The WISE group recently reported on the prognostic significance of hemoglobin values in women with suspected ischemia. In the WISE study, anemic women (defined as hemoglobin <12 mg/dl) had a higher risk of all-cause death (10 vs 5%; p = 0.02) and major adverse cardiovascular outcomes (26 vs 16%; p < 0.01) when compared with nonanemic females [32]. Women with anemia also had a shorter survival time free of adverse outcomes (p < 0.001). These findings extend previous reports on an inverse relationship between lower hemoglobin levels and a higher risk of adverse cardiovascular outcomes in women with chest-pain symptoms.
Inflammation may be central in explaining the association between anemia and heart disease. The role of chronic inflammation and inflammatory cytokines in atherosclerosis has been extensively studied and documented [33,34]. Epidemiologic studies have demonstrated that the most common cause of anemia in older men and women is anemia of chronic disease (ACD) [35]. ACD is thought to be the most likely cause of anemia in WISE women. It is associated with chronic inflammatory states and proinflammatory cytokines may modulate cardiovascular risk in patients with ACD, proposing a pathophysiologic explanation for the above findings.
These findings support the role of modifying traditional and nontraditional risk factors for CAD. Future studies need to investigate the biologic link and association between metabolism, inflammation, coronary atherosclerosis and cardiovascular risk in women.
Expert commentary & conclusions
IHD morbidity and mortality in men has continuously declined over the last few decades [26]. In contrast, the prevalence of IHD and its related consequences in women has continued to increase steadily to a point where more women than men die from IHD. Findings from the WISE study support the need to define key gender-specific differences in pathophysiology, presentation, evaluation and treatment of IHD. Many existing evaluation models were developed based on clinical research in a predominantly male patient population. Epidemiologic data shows that significant gender and racial differences continue to exist in the treatment and management of CAD [36]. It appears that typical angina symptoms and electrocardiographic changes in women do not predict CAD as well as they do in men. Models incorporating variables specific to women are necessary to effectively risk stratify these patients. In addition, the estimated prevalence of microvascular ischemia specific to women defines a patient cohort that is not included in the assessment of the burden of heart disease on healthcare and related costs in the general population. More importantly, the WISE study results highlight the adverse prognostic implications of Cardiac Syndrome X, and strongly lend support to efforts towards further study into the pathophysiology, diagnosis and treatment of microvascular ischemia. The use of noninvasive tests such as CMR and invasive coronary vasomotor testing are tools that can be used for appropriate diagnosis and cost-effective management of these challenging patients. The WISE study findings remind us of the importance of psychosocial variables and their association with IHD and that we must incorporate behavioral cardiology into clinical care. Last but not least, WISE results emphasize the need to continue to study and define the major role of reproductive hormones on the cardiovascular system through the spectrum of pre-, peri- and postmenopausal life.
So, in response to our initial question, ‘Are we ‘WISE’r?’ – the answer is ‘absolutely!’ The WISE study has produced a number of important findings, some new and others confirming previous observations, and has forged new key concepts relating to ischemic heart disease in women. Future research into the mechanisms, diagnosis and treatment of and public education regarding coronary heart disease in women is needed to improve outcomes and save lives.
Executive summary
The Women's Ischemia Syndrome Evaluation (WISE) study is an ongoing project of the National Heart, Lung and Blood Institute in the USA, aiming to improve pathophysiologic understanding, evaluation, diagnosis and treatment of ischemic heart disease in women.
Traditional assessment tools for chest pain do not reliably predict angiographic coronary artery disease (CAD) in WISE study women.
More women than men have chest pain in the absence of obstructive CAD on coronary angiography (Cardiac Syndrome X). Almost half of WISE study women with Cardiac Syndrome X have evidence of microvascular ischemia, measured as diminished coronary flow velocity measured during coronary angiography.
Women with microvascular ischemia have increased morbidity and mortality.
Myocardial perfusion imaging tools, such as cardiac myocardial resonance, are important in the accurate assessment of macro- and microvascular ischemia in women.
WISE reports demonstrated a direct relationship between depression and angiographic CAD. WISE reports also demonstrated an increased risk of cardiovascular events in women with traits of cynicism, hostility and aggression. The incorporation of an assessment of psychosocial variables in women with CAD risk factors may be of vital importance, as treatment may lend benefit.
Premenopausal women with CAD have significantly worse cardiovascular outcomes compared with age-matched men. Hypothalamic hypoestrogenemia was the strongest predictor of angiographic CAD in premenopausal WISE study women.
The metabolic syndrome confers a twofold increased risk of angiographic CAD and treatment goals central to the treatment of insulin resistance should be incorporated into practice.
The evaluation, diagnosis and treatment of ischemic heart disease in women requires understanding that there are key differences between men and women. Women with ischemia do not present with typical angina symptoms, and women with persistent or recurrent typical or atypical chest pain in the presence of significant cardiac risk factors and a ‘normal’ coronary angiogram need further evaluation for microvascular ischemia.
Footnotes
This work was supported by contracts from the National Heart, Lung and Blood Institutes, Nos. N01-HV-68161, N01-HV-68162, N01-HV-68163, N01-HV-68164, a General Clinical Research Centers (GCRC) grant MO1-RR00425 from the National Center for Research Resources, and grants from the Gustavus and Louis Pfeiffer Research Foundation, Denville (NJ, USA); The Women's Guild of Cedars-Sinai Medical Center, Los Angeles (CA, USA); and The Ladies Hospital Aid Society of Western Pennsylvania, Pittsburgh (PA, USA). None of the work represents a conflict of interest and there are no financial relationships to disclose among the coauthors.