
Abstract
Crohn's disease and ulcerative colitis are two chronic inflammatory conditions involving the gastrointestinal tract. While many aspects of the management of these diseases are identical for all patients, there are some issues specific to women that are not necessarily part of routine care. Certain gender-specific issues such as menses, fertility, pregnancy and menopause are often overlooked and mismanaged. Women have different psychologic concerns compared with men in regard to their self-image and impact of disease. Healthcare providers, regardless of their primary focus, should be aware of these differences and be familiar with general information specific to women.
The incidence of Crohn's disease (CD) in women has been increasing over the past few decades [1]. It is not clear whether this is due to improved diagnostic techniques, an increase in smoking habits of young women (CD patients tend to be smokers compared with people without CD [2]) or other factors not yet identified. However, the consequence of this trend is a growing population of patients with gender-specific needs and concerns related to their medical care. Every component of the reproductive cycle can potentially affect disease course or symptomatology. As the diagnosis of CD or ulcerative colitis (UC) is often made during the childbearing years, fertility and pregnancy are important issues that have previously been handled exclusively by gynecologists. Healthcare providers caring for women with inflammatory bowel disease (IBD) should be aware of these issues and their appropriate management. The aim of this article is to review some clinically relevant gender-specific issues in IBD.
Self-image issues
Maunder and colleagues reported consistently higher levels of symptom severity and rating of IBD patient concerns in women than in men [3]. Patient concerns that differed by gender included attractiveness, intimacy and sexual performance. Women also had stronger concerns about self-image, feeling alone and being fearful of having children.
Active disease can lead to fatigue and loss of libido in addition to the embarrassment of fecal incontinence. Corticosteroids to treat active disease lead to Cushingoid features along with weight gain and mood swings. Perineal involvement in CD can be physically deforming and result in dyspareunia and self-consciousness. The presence of an ostomy or other surgical scars can also lead to lower self-esteem [4].
The menstrual cycle
For girls diagnosed with IBD before or during puberty, the onset of menses can be delayed. This can be secondary to chronic inflammation or a poor nutritional status that directly affects steroid hormone production. Menarche usually occurs once active disease is treated appropriately.
Disease activity can also affect the menstrual cycle after menarche. This can be manifested by irregular or skipped periods or an increase in disease symptoms during the premenstrual or menstrual phase. A study by Kane and colleagues corroborates this phenomenon [5]. Premenstrual syndrome (PMS) includes gastrointestinal symptoms, but women with IBD complain of these symptoms above and beyond that found in the normal population. Some women consider these mini-flares. In reality, this is a cyclic, predictable phenomenon, which is neither random or imagined. Rather than treating these symptoms as active IBD, conservative treatment to alleviate symptoms is more appropriate, as symptoms will tend to resolve after a few days.
Some women have such debilitating symptoms that the elimination of menses is the only way to provide relief. This can be achieved with short-term injectable contraceptives (e.g., Depo-Provera®) or hormones (e.g., Lupron®). At this time, a hysterectomy is not recommended for this indication, but those women who undergo this procedure for other gynecologic reasons find that their IBD symptoms improve [6].
Fertility
Overall, the fertility rates of women with IBD are essentially the same as those of the normal population [7]. The major caveat to this rule is in women who have undergone ileal pouch–anal anastomosis (IPAA) for UC [8,9]. Fecundity (the physiologic ability to reproduce) decreases by upwards of 80% in women who have undergone this procedure; the true etiology of this finding is unclear but presumed extensive adhesion formation in the pelvis, which impairs normal tubal function, is thought to play an important role. In the setting where a woman is facing a total colectomy for refractory disease, the possibility of an ileorectal anastomosis should also be discussed. Early studies suggesting lower fertility rates did not take into account an increased voluntary childlessness rate in women with IBD.
Active CD, however, can reduce fertility in several ways, depending upon the location of inflammation. Active inflammation in the colon has been shown to decrease fertility [10], as well as any inflammation or scarring directly involving the fallopian tubes or ovaries. Women who have had any surgical resection are at risk for adhesions, which can also impair tubal function.
None of the medications used to treat IBD have an effect on female fertility, but it is important to remember that sulfasalazine therapy reduces sperm motility and count in males. While there is no minimum required time period for quiescent disease prior to a planned conception, at least 3 months is recommended. Open discussions between patient and physician are the best way to ensure the optimal outcome of a pregnancy. If a woman is doing well and in remission, there is every reason to expect the pregnancy to proceed smoothly. If active disease is present, it is likely to continue through pregnancy and will place the pregnancy at greater risk for complications [11]. This risk appears to be higher in CD than in UC.
The main priority is to establish and maintain remission before the patient conceives. One of the problems in CD is the accurate definition of remission. In CD, a patient may feel fine even though she has elevated C-reactive protein (CRP) levels, an abnormal colonoscopy and/or x-ray.
Some women remain childless for fear of disease transmission to their offspring. Current data suggests that this risk is low; 7% if one parent has CD and less if one parent has UC [12]. However, the risk of IBD increases to as high as 37% if both parents have the disease. The risk of inheriting IBD is higher in Jewish (7.8%) than in non-Jewish (5.8%) families [13]. It is important to remember that IBD is not a genetic disorder in a true Mendelian fashion. Even with genetic predisposition, other factors are necessary to produce expression of either disease.
Contraception
The management of contraception in those women with IBD who do not wish to become pregnant differs from that for normal women. The most important goal still remains the selection of the most reliable method of birth control. Barrier methods of contraception are acceptable but are not as effective as alternatives. The use of intrauterine devices is not usually recommended, as any complaint of abdominal pain could potentially delay the correct diagnosis of active IBD versus pelvic inflammatory disease.
The data regarding the safety of oral contraceptives (OCs) in IBD are conflicting. Early studies suggested an increased risk for the development of CD and UC but did not account for tobacco use [6,14–16]. Reports from Europe, where contraceptives contain a higher estrogen content, continue to show modest increases in the risk of developing CD after adjusting for cigarette use (odds ratios [ORs]: 1.2–2.0) [17–19].
Other data suggest that OC use may exacerbate disease activity [20,21]. Two small, prospective studies have found an increased risk of disease recurrence after induction of remission in CD with OC use. No information is available regarding a possible similar risk in UC.
At this time, no standard guidelines exist for OC use, as there are many preparations available. Some physicians successfully use OCs to treat symptoms that appear to be related to the menstrual cycle, to temper the effect of fluctuating hormone levels. Variable amounts of progesterone and estrogen are the factors that determine the side-effect profile. The choice of OC preparation must be individualized, taking into consideration other factors including patient history, parity and personal preferences. It appears prudent to try a formulation that contains the lowest amount of estrogen possible, given the additional risk factors of smoking and predilection towards thromboembolic events in patients with CD.
Effect of inflammatory bowel disease on pregnancy
Women with inactive IBD appear no more likely to experience spontaneous abortion, stillbirth or children born with a congenital abnormality [13]. Figure 1 summarizes the results of 24 published reports comparing outcomes in women with IBD versus the normal population. Some studies have suggested that babies born to women with IBD, regardless of disease activity, are of smaller birth weight [22]. This appears to be particularly the case in those women with CD. Women with active disease run a greater risk for premature birth [23].

Effect of inflammatory bowel disease on pregnancy outcomes in 24 published reports.
The presence of IBD does not appear to have an impact on maternal complications related to pregnancy, including hypertension or proteinuria [24]. However, active perianal disease may worsen after a vaginal delivery. One retrospective study of women with CD found that 18% of those without previous perianal disease developed such disease after delivery, usually involving an extensive episiotomy [25]. Otherwise, the presence of IBD does not have a significant impact on the method of delivery, nor is it an indication for cesarean section.
Effect of pregnancy on inflammatory bowel disease
For women with quiescent UC, the rate of relapse is approximately the same in pregnant versus nonpregnant patients [11]. This is in contrast to the presence of active disease at the time of conception, which is associated with continued or worsening disease activity in approximately 70% of women. Comparable observations are seen in CD. Figures 2 & 3 illustrate pregnancy-related disease activity as reported by Miller and colleagues [11]. The older literature suggested a trend for disease to flare up in the first trimester; however, this was documented prior to the accepted practice of maintenance therapy, continued even during pregnancy. A possible explanation for these findings was investigated by Kane and colleagues [26]. They demonstrated that the degree of maternal–fetal human leukocyte antigen (HLA) disparity predicted disease course throughout pregnancy. The proposed mechanism is that disparity at specific alleles leads to a downregulation of the mother's innate immune system so as to not reject this foreign entity; a consequence of this downregulation is a self-induced immunosuppression and a clinical improvement.
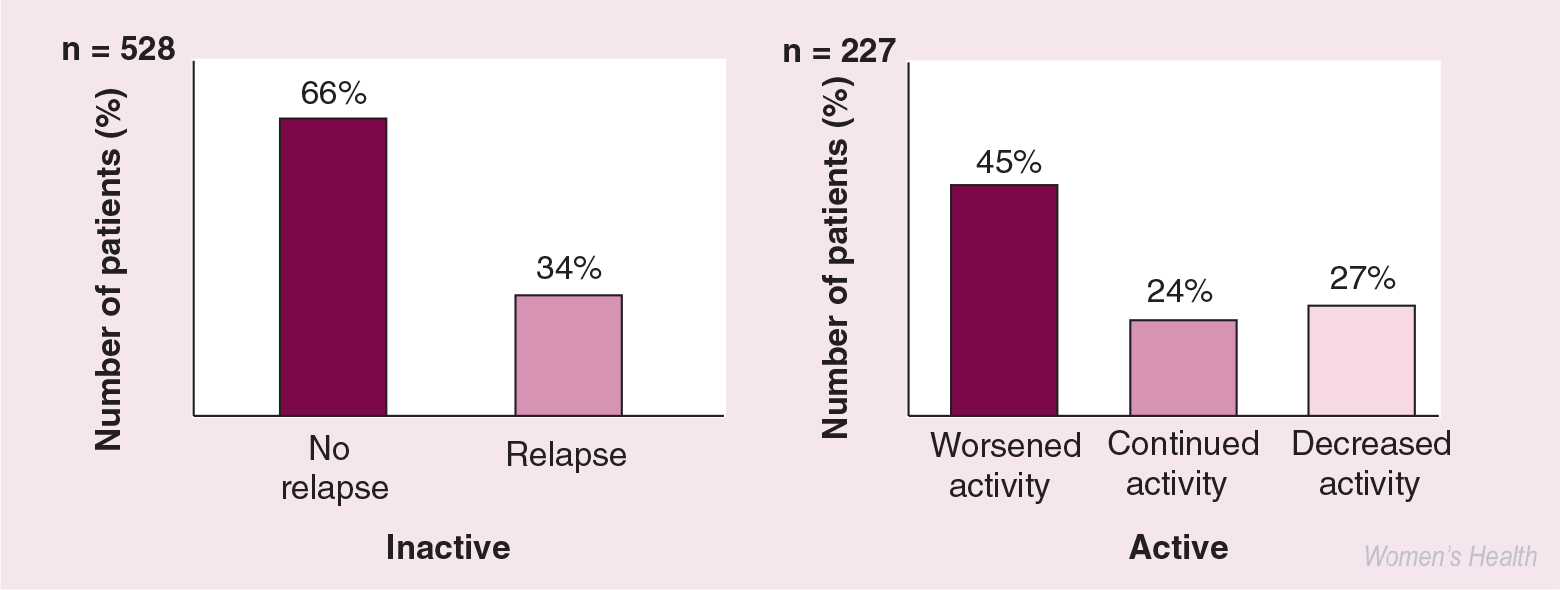
Effect of pregnancy on ulcerative colitis: disease activity at conception.

Effect of pregnancy on Crohn's disease: disease activity at conception.
It is important to remember that hemoglobin and albumin levels decrease and erythrocyte sedimentation rate (ESR) increases during pregnancy. Due to these normal physiologic changes, disease assessment during pregnancy should rely more on clinical symptoms than laboratory parameters. Ultrasound exams are clearly safe and there is no evidence that, if indicated, a sigmoidoscopy will induce premature labor [27]. Colonoscopy should only be performed when extent and severity of disease, specifically, need to be ascertained.
There are data suggesting that a history of child-bearing changes the natural history of CD [28]. Women who had been pregnant had fewer resections or longer intervals between resections compared with women who had not had children but experienced otherwise similar disease. One theory proposed by the authors is the inhibition of macrophage function by relaxin. Relaxin is a hormone produced exclusively during pregnancy which may result in less fibrosis and stricture formation by this inhibition of macrophages.
Treatment of inflammatory bowel disease during pregnancy
The key principle to the management of IBD is to remember that the greatest risk to pregnancy is active disease, not active therapy [29]. Since there are limited definitive data available on the safety of IBD medications in pregnancy, the focus should therefore be on establishing remission before conception and maintaining remission during pregnancy.
Sulfasalazine readily crosses the placenta but has not been associated with any fetal abnormalities. However, patients taking sulfasalazine should also be supplemented with folic acid before conceiving to decrease the risk of neural tube defects. A dose of 1 mg twice daily is appropriate.
The safety of mesalamine during pregnancy has been demonstrated in a number of trials [3,30]. In two separate studies, women taking 2–3 g/day experienced no increased incidence of fetal abnormalities than that in normal, healthy women. Topical 5-aminosalicylic acid (5-ASA) agents are likewise safe during pregnancy [31].
The data regarding immunomodulator therapy (e.g., azathioprine and 6-mercaptopurine [6-MP]) are more conflicting. There are no large studies on the use of these medications during pregnancy in women with IBD. To date, the information comes from the transplantation literature [32] and from small retrospective series in IBD [33,34]. It is generally believed by the most experienced IBD clinicians that immunosuppressives such as 6-MP, azathioprine and cyclosporin can be used safely during pregnancy if the mother's health mandates therapy. Methotrexate, another immunomodulatory medication, is contraindicated in pregnancy.
Corticosteroids have not been associated with teratogenicity in humans and can be used as required to control disease activity [23]. Prednisone crosses the placenta less efficiently than other steroid formulations such as betamethasone or dexamethasone. Only limited data are available regarding the safety of antibiotics as a treatment for CD. Currently, ampicillin, cephalosporins and erythromycin are believed to be safe, while ciprofloxacin is contraindicated due to the potential for arthropathogenecity in the fetus. Metronidazole has been used to treat vaginitis in women during the first trimester of pregnancy but no controlled trials have definitively shown its safety [35]. The safety of medications used in IBD is detailed in Box 1.
Safety of inflammatory bowel disease medications during pregnancy.
Safe to use when indicated
– Oral mesalamine, balsalazide
– Topical mesalamine
– Sulfasalazine
– Corticosteroids
– Ciprofloxacin (after first trimester)
Limited data
– Olsalazine
– Azathioprine/6MP
– Infliximab
– Cyclosporin
– Metronidazole
Contraindicated
– Methotrexate
– Thalidomide
Infliximab is the first biologic therapy approved for use in CD. It has been given a category B safety rating. Postmarketing data suggest that it is not associated with an increased risk of congenital anomalies or infectious complications in those children born to mothers receiving this therapy [36,37].
The medications known to be safe for breastfeeding include sulfasalazine, the mesalamine preparations (e.g., Asacol®, Pentasa® and Rowasa®) and steroids. Mothers planning on breastfeeding should discontinue the use of cyclosporin, metronidazole, ciprofloxacin and methotrexate. No data are available regarding the thiopurines and these should be discussed on a case-by-case basis. The safety data regarding medications and their use during breastfeeding are summarized in Box 2. Current studies are underway to measure medication levels in breast milk to assess for any increased risk of immunosuppression of the infant.
Surgery & pregnancy
The indications for surgery during pregnancy are identical to those of nonpregnant patients. These include obstruction, perforation, abscess and hemorrhage. Pregnancy has not been shown to complicate stoma function. Women may experience some prolapse due to abdominal pressure, but no increased risk to the pregnancy is encountered.
For those women who have had IPAA procedures, an increase in the number of bowel movements during pregnancy has been reported, but no increased risk for pouchitis or delivery complications was found [38].
Surgical outcomes
A varying incidence of dyspareunia has been reported following pelvic surgery, ranging from 0–26% [39–41]. This variation may be due to the heterogeneous nature of surgeries, under-reporting of symptoms to physicians or inappropriate control populations. After IPAA, one report found a 15% incidence of dyspareunia and an increase in menstrual problems [4].
Safety of inflammatory bowel disease medications during breastfeeding.
Safe to use when indicated
– Oral mesalamine, balsalazide
– Topical mesalamine
– Sulfasalazine
– Corticosteroids
No data
– Olsalazine
– Azathioprine/6-MP
– Infliximab
Contraindicated
– Methotrexate
– Thalidomide
– Cyclosporin
– Ciprofloxacin
– Metronidazole
Menopause
Menopause, whether natural or surgical, leads to many physiologic changes in a woman's body. Just as OCs can help with controlling symptoms, there is data to suggest that some of the gastrointestinal symptoms associated with IBD decrease in women who have achieved menopause.
Women with UC are at no greater risk for an early menopause than women without IBD. There is some data to suggest that women with CD may enter menopause earlier than normal women, but a mechanism has yet to be established for this finding [6].
What is certain; however, is that the risk for osteoporosis is substantially higher due to steroid exposure, decreased dairy product consumption secondary to lactose intolerance, active inflammation and malabsorption related to inflamed gastrointestinal mucosa [42]. It is recommended by some that every woman with IBD undergo a bone-density scan to assess for bone loss. If present, then replacement calcium and vitamin D are essential, with the addition of bisphosphonates as indicated.
The issues regarding hormonal replacement therapy (HRT) are identical to those in normal women for bone loss and cardioprotection. Family history for any breast or uterine cancer, or a personal history of either these or thromboembolic events need to be taken into consideration when making a decision regarding HRT.
Conclusion
The management of women with IBD often presents special challenges to the healthcare provider. The different phases of the reproductive cycle in a woman's life can lead to significant medication changes and management decisions. While infertility rates are not usually increased, patients with an ileal pouch need to be counseled prior to surgery regarding their fertility. Management of the pregnant IBD patient has the same goals as for the nonpregnant patient – to induce remission in those with active disease and maintain remission in those without. The risk:benefit ratio for the majority of the medications used to treat IBD weighs heavily in favor of the benefit of a healthy mother. Mode of delivery and breastfeeding decisions should be individualized based on a patient's surgical history, the presence of perianal disease and the mother's preferences and obstetric indications. In the author's practice, these discussions with the patient are attempted prior to a pregnancy, with significant others and family members also involved.
Future perspective
As more biologics for the treatment of these diseases continue to be developed, an understanding will need to be reached on what impact they may have on a growing fetus and its ability to mount its own immune responses. Continued use and experience with standard medications will further document their apparent safety during pregnancy. Understanding the mechanisms underlying the immune response and its interaction with the hormonal milieu will help to better predict the disease course during the different phases of the menstrual cycle, the effect of hormonal manipulation and the effect of menopause on the innate immune system and disease symptomatology.
Executive summary
The menstrual cycle can affect inflammatory bowel disease (IBD) symptoms.
The use of oral contraceptives is not contraindicated in women with IBD.
Physicians should be mindful of self-image issues in women who have significant perianal Crohn's disease or a stoma.
Fertility can be affected in the postsurgical ulcerative colitis patient and the patient with active Crohn's disease.
Quiescent IBD does not appear to increase the risk of an adverse birth outcome.
Active disease at conception increases the risk of adverse outcomes.
The majority of medications for IBD are safe in pregnancy and breastfeeding-active disease is more deleterious than active therapy.