
Abstract
Previous studies showed that low dose radiation (LDR) could stimulate the immune system in both animal and human populations. This paper reviews the present status of relevant research as support to the use of LDR in clinical practice for cancer prevention and treatment. It has been demonstrated that radiation-induced changes in immune activity follows an inverse J-shaped curve, i.e., low dose stimulation and high dose suppression. The stimulation of immunity by LDR concerns most anticancer parameters, including antibody formation, natural killer activity, secretion of interferon and other cytokines as well as other cellular changes. Animal studies have revealed that LDR retards tumor growth, decreases cancer metastasis, and inhibits carcinogenesis induced by high dose radiation. These effects of LDR on cancer control were found to be related to its stimulation on immunity. The experimental data may well explain the efficacy of the clinical trial of LDR in the treatment of cancer.
I. INTRODUCTION
Carcinogenesis induced by environmental agents is a problem of concern to the public and scientific bodies. Ionizing radiation is one among these environmental agents. It is well known that most carcinogens are immunosuppressants. Ionizing radiation is one of these when delivered at moderate to high doses. Immune surveillance is one of the most important defense mechanisms in the body monitoring the development of cancer. As reviewed in previous reports low dose radiation (LDR) enhances immune functions.(1, 2) The significance of these immunologic changes in radiation-induced cancer is still a question of debate. In UNSCEAR 1994, it is stated, “the immune system may not play a major role in moderating human radiation oncogenesis, although immune function in certain organs may ensure that some early neoplastic cells are eliminated before they become established”.(3) NCRP Report No. 136 states, “in the ultimate instance of cancer in vivo, the adaptive response may take the form of an immune surveillance of pre-neoplastic cells. This is certainly a possibility, but it is difficult to design laboratory experiments to test it”. (4) In a recent commentary article on radiation hormesis, it is recognized that “under appropriate conditions, exposure to X-rays or gamma rays at doses below those causing immunosuppressive effects has been observed to augment various immune responses in mice…” but “the mechanisms of the observed enhancement remain to be elucidated in full…”.(5) These statements accept the importance of experimental data on LDR-induced enhancement of immunity and its surveillance of cancer formation on one hand and question its significance in cancer control on the other.
There have been accumulating data disclosing the cellular and molecular mechanisms of LDR-induced activation of anti-tumor immunity in animal models, as reviewed in Reference 1. LDR increases cellular antioxidant activity; facilitates DNA damage repair; reduces malignant transformation and mutagenesis, and stimulates immune surveillance.(6 –10) All these may contribute to the effect of LDR on the reduction of cancer incidence. There have been experimental studies illustrating: a) the suppressive effect of LDR on tumor growth, metastasis and carcinogenesis, b) the increased anti-cancer immunity, including enhanced NK and CTL activity, and c) the increased IFNγ and IL-2 secretion. All these data point to the significance of enhanced immune responses in cancer control.(11 –23)
II. LOW DOSE RADIATION AND IMMUNITY
Stimulation of immunity by low dose radiation is manifested in various aspects.(1) Table 1 shows the immunologic parameters studied in the author's laboratory demonstrating up-regulation of immune functions in animal models exposed to single as well chronic irradiation.(24 –36) As illustrated in this table, most immunologic parameters are stimulated after whole-body irradiation (WBI) by doses within 0.1 Gy, using a dose-rate within 15 mGy/min. The NK (natural killer) activity of splenocytes was assessed with the 125I-UdR release method using YAC-1 cells as targets in C57BL/6J mice. Significant stimulation was observed after WBI with both 75 and 500 mGy. For most immunologic parameters of splenocytes, doses above 500 mGy may exert an inhibitory effect. But with NK activity, 500 mGy showed an even higher stimulatory effect than 75 mGy. This is obviously related to the relatively higher radio-resistance of the NK cells. This is also the case with macrophages. WBI with 75 mGy caused a 32% increase of the secretion of IL-12 (see Table 1), with higher increases after doses above 1 Gy (not shown). The inhibitory effect of peritoneal macrophages on the growth of tumor cell line S180 was increased by 52% after WBI with 75 mGy. The specific CTL activity was assayed in C57BL/6J mice bearing Lewis lung carcinoma; a 40% increase of cancer suppressive effect was observed. The ADCC (antibody-dependent cell-mediated cytotoxicity) activity is a specific reaction to P815 cancer cells, assessed with the 125I-UdR release method. These four parameters are directly related to anticancer immunity. The PFC (plaque forming cell) reaction denotes the capacity of antibody formation in response to sheep RBC as antigen. This is a T-dependent reaction, which was found to be stimulated by both cute and chronic low dose radiation. Under very low dose rate, 15 μGy/min, a cumulative dose of 65 mGy increased the response significantly – by 16%. The measurement of T cell proliferation is an indication of activation and clonal expansion of the T lymphocytes, representing immune activation. Four sets of data are shown in Table 1, the first two of which are from experiments on Balb/c mice. These mice are relatively sensitive to ionizing radiation. The third and fourth sets of data are from Kunming mice, which show a response to ionizing radiation comparable to that of C57BL/6J mice, as tested in our laboratory. It is interesting to note that after an acute dose of 75–106 mGy, at the dose rate of 12.5–12.7 mGy/min, both strains of mice responded with an increase in T cell proliferation of more than 100%. However, for the Balb/c mice, this dose would have no effect in T cell proliferation if the dose rate were 200 mGy/min.(32) Other authors have also noted this strain difference of lymphocyte proliferation in response to radiation.(37) The secretion of cytokines was stimulated in favor of differentiation of the TH1 subset. Activation of T lymphocytes is related to the up-regulation of surface molecules CD2, CD3 and CD28 after LDR.(1, 2, 27, 38) In response to these changes, intracellular signal transduction is facilitated.(39 –44) Among these, the up-regulation of PKC and [Ca2+]i forms the most important intracellular molecular basis of T lymphocyte stimulation (Table 2).
Immune functions stimulated by low dose radiation in mice

All data represent experimental results obtained 24h after LDR except otherwise specified. 1. Macrophage antitumor activity assayed with S180 cells; 2. Specific cytolytic T lymphocyte activity of splenocytes assayed with Lewis lung cancer cells; 3. Antibody-dependent cell-mediated cytotoxicity of splenocytes assayed with P815 cells; 4. Mice were immunized with sheep RBC on day 4 after WBI and plaque-forming cells were counted on day 9; 5. T cell proliferation was measured with 3H-TdR incorporation in the presence of Con A 5 μg/ml; 6. G-CSF was assayed with RIA. Reference numbers are given in parenthesis; pc=personal communication).
Important Intracellular signal molecules stimulated by low dose radiation 1
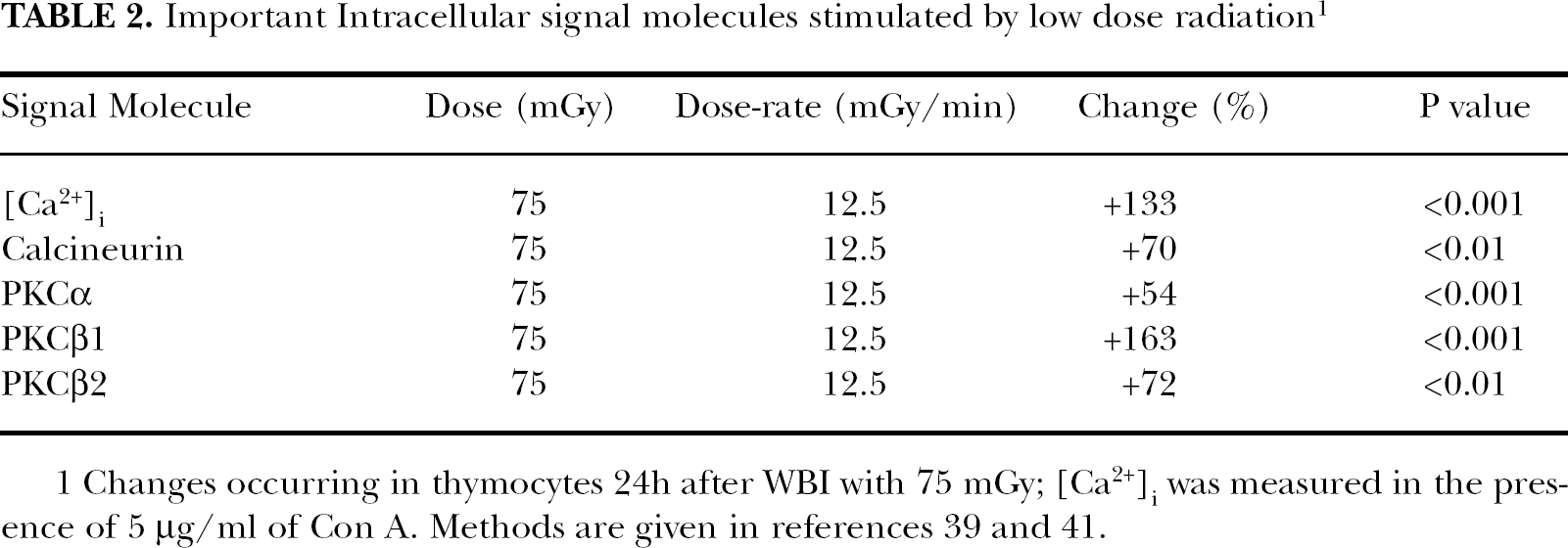
1 Changes occurring in thymocytes 24h after WBI with 75 mGy; [Ca2+]i was measured in the presence of 5 μg/ml of Con A. Methods are given in references 39 and 41.
III. EFFECT OF LOW DOSE RADIATION ON CANCER CONTROL(11 –23)
It was shown that irradiation with low dose X-rays decreased the growth rate and metastasis of implanted B16 melanoma and Lewis lung cancer in C57BL/6J mice. As shown in Figure 1, the effect of WBI with 0.075 Gy (given 24h before implantation of Lewis lung cancer cells) on tumor growth is manifested as: decrease in tumor size by ∼50% (column 1); increase in mean survival time by ∼40% (column 2), and decrease of 30-day mortality rate by ∼40% (column 3).(11, 18, 31)

Effect of low dose radiation on Lewis lung cancer (0.075 Gy WBI, 24 h before tumor implantation)
Figure 2 shows the reduction of pulmonary metastasis of B16 melanoma cells after WBI with 0.05–0.15 Gy (intravenous injection of B16 cells 24 h after irradiation, showing significant reduction of lung nodules of cancer cells 14d after injection)(12, 14, 15). Figure 3 shows the effect of LDR on the efficacy of mitomycin C (3 mg/kg body weight) on the growth of Lewis lung cancer cells implanted to mice. WBI with 0.075 Gy, 6 h before chemotherapy, further reduced the tumor size (column 3 compared to column 2)(16, 17, 23). Figure 4 shows the alleviation of immune suppression caused by tumor burden (Lewis lung cancer implantation) by LDR, as demonstrated by the recovery of the lowered NK activity after LDR in tumor-bearing mice.(13)

Low dose radiation reduces cancer metastasis (Injection of B16 cells, i.v., 24 h after WBI with different doses of X-rays)

Low dose radiation increases efficacy of cancer chemotherapy
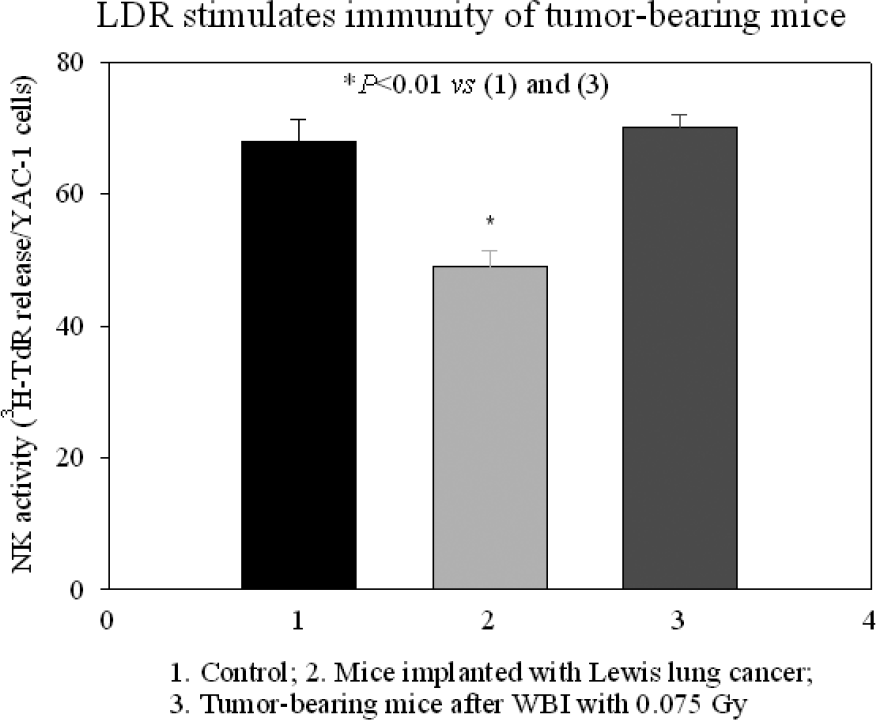
Low dose radiation stimulates immunity in tumor-bearing mice
In a well recognized model of thymic lymphoma, induced by fractionated WBI (1.75 Gy once a week for 4 consecutive weeks) in C57BL/6J mice, a low dose of radiation (0.075 Gy), 6–12 hours preceding each fractionated high dose radiation (HDR), could reduce the lymphoma incidence from 43.3% in the control (exposed to only the HDR) to 15.1% (HDR being preceded by 0.075 Gy with an interval of 6h) and 17.6% (HDR being preceded by 0.075 Gy with an interval of 12h) in 6 months after the fractionated exposures. These inhibitory effects of LDR on cancer growth and cancer induction are accompanied with immunologic stimulation.(11, 19, 21, 22)
Clinical application of LDR in the treatment of cancer has shown enlightening results. When patients with non-Hodgkin's lymphoma under chemotherapy were given total body or half body (to the thorax) LDR in a regimen of 0.1 Gy 3 times a week or 0.15 Gy 2 times a week for 5 consecutive weeks with a total dose of 1.5 Gy, the survival rate in 9 years rose to 84% from 50% of the control with chemotherapy alone (P < 0.01). The LDR-treated patients also showed enhanced anti-cancer immunity.[45]
In an area of high natural radioactivity with the exposure rate 3 times as high as that in the adjacent control area in south China with epidemiological survey having been continued for 31 years, the cancer mortality rate was found to be slightly lower than that among the inhabitants in the control area.(46) Examination of the peripheral blood of the inhabitants showed increased reactivity of the lymphocytes to PHA and enhanced DNA damage repair capability as shown by increased UDS of the lymphocytes.(47) There were increased chromosome aberrations in the blood samples implicating DNA damage.(46) It is supposed that the balance between radiation damage and defense mechanisms under this circumstance results in no increase or even lowering of cancer mortality in spite of the long term exposure of the inhabitants to the low level radiation.
IV. CONCLUDING REMARKS
The stimulation of immunity by LDR concerns most anticancer parameters, including antibody formation, NK activity, CTL activity, macrophage activity, ADCC activity, secretion of interferon and other cytokines as well as other cellular changes. Animal studies have revealed that LDR retards tumor growth, decreases cancer metastasis, and inhibits carcinogenesis induced by high dose radiation. These effects of LDR on cancer control were found to be related to its stimulation on immunity. The experimental data may well explain the efficacy of the clinical use of LDR in the treatment of cancer. This paper reviews the present status of relevant research on effects of low dose radiation on anticancer immunity as support to its trial in clinical practice.
Footnotes
ACKNOWLEDGMENT
This paper is prepared with support by grants from the Natural Science Foundation of China.