
Abstract

Introduction
Rothera research station is a British Antarctic Survey (BAS) base on the Antarctic Peninsula that is operational year round. During the 8-month winter the 20 people living there are physically isolated from any other humans. I was the resident doctor during the 2005 season. I did not leave Antarctica for 17 months of my employment with the British Antarctic Survey Medical Unit (BASMU), and during the winter period I was the sole medical practitioner on station.
My medical work load was light in comparison to any other job I have done. All personnel deployed to a UK Antarctic base were fit and well, and the wintering team in particular had been screened for any significant physical and mental illness. On average during the winter period I would perform 40 consultations per month. Because I was only serving a population of 20, the relatively large number of consultations reflected the harsh environment in which we lived and worked. The perceived major health risks of BAS Antarctic employment were the operational tasks of year round SCUBA diving and summer light aircraft movements and environmental cold injuries. Predeparture training and on-site equipment (eg, a recompression chamber) equipped me to deal with these issues. However, most of my work load was composed of minor injuries sustained during work or leisure pursuits in the difficult environment, psychological issues, dental work, gynecology, and genitourinary medicine.
During the summer months there were 2 doctors, one who had just arrived and one who had finished a winter season and would return home at the end of summer. One doctor was always on base, as diving and aircraft operations continue throughout the 24-hour daylight. In winter the solo doctor took part, as all base members did, in 2 winter training trips, each a week long, which made them inaccessible to base other than through a nightly prearranged radio call. During this time remote assistance and advice was provided to the station by BASMU based in Plymouth, UK. This group of specialist consultants also provided advice and support for the doctor throughout the term of duty.
There are many aspects of the season I spent in Rothera that I will continue to reflect on for some time. The enclosed environment created an amplified feedback on many of my actions and forced a range of emotions. Although few of the medico-social issues are unique to Rothera, I had never before been in a position where every action or word on my part, either in a clinical situation or socially, had the potential to significantly change my relationship with the other members of my group (particularly in winter) and alter my ability to serve that group as a doctor. I would like to discuss specifically the topics of medical confidentiality, treatment styles, 24-hour on-call duties, and personal relationships.
Medical confidentiality
When I first arrived in summer 2004, medical confidentiality was straightforward and easy for me to maintain. People did not really know me, and the base had a large (>100) population and a demanding work schedule, so it was not obvious if people were coming to see the doctors. There were few intimate conversations around the bar as that venue was busy. I was therefore lulled into a false sense of security about an issue that I had been fairly worried about before I took up my post. Things changed dramatically as numbers dropped toward winter, friendships formed, and people knew me and felt comfortable talking to me. Any visible sign of illness or injury was asked about. However, this only represented a minority of cases. I certainly made this worse for myself because of my willingness to discuss general medical issues with people socially when they inquired, for example, about the effects of drugs and alcohol or high profile diseases in the press. The questioning became more intense and educated when “doc school” started (the weekly training sessions run by me aimed at training half the winter base members to be medical assistants in emergency situations). There was a core of 11 winterers who were very interested in medical matters. Any plastering and stitching was organized to involve members of doc school if the patient consented, further blurring the margins of exclusive doctor-patient relationships.
I initially tried, at the end of summer, to say that I was not going to discuss any aspect of a patient's pathology or treatment outside of the clinical area, but it soon became apparent that often the patient talked about his or her injury/illness in social settings and wanted to involve me in the discussion, either to explain better what was going on to friends or because during the discussion with others the patient had thought of other points he or she wanted to discuss. It seemed socially inept to cut these conversations off when in fact it was the patient initiating them. I then made the decision, when appropriate (obvious or witnessed injury, for example), to ask the patient at the initial consultation whether they would like me to share any information with the group and, if so, how much. Where it was clearly inappropriate for any information to be shared (gynecological, psychiatric, and genitourinary consultations, for example), I also made a point of stating in the consultation that none of this information would be shared with anyone else. A continuum of confidentiality evolved (see the Figure).
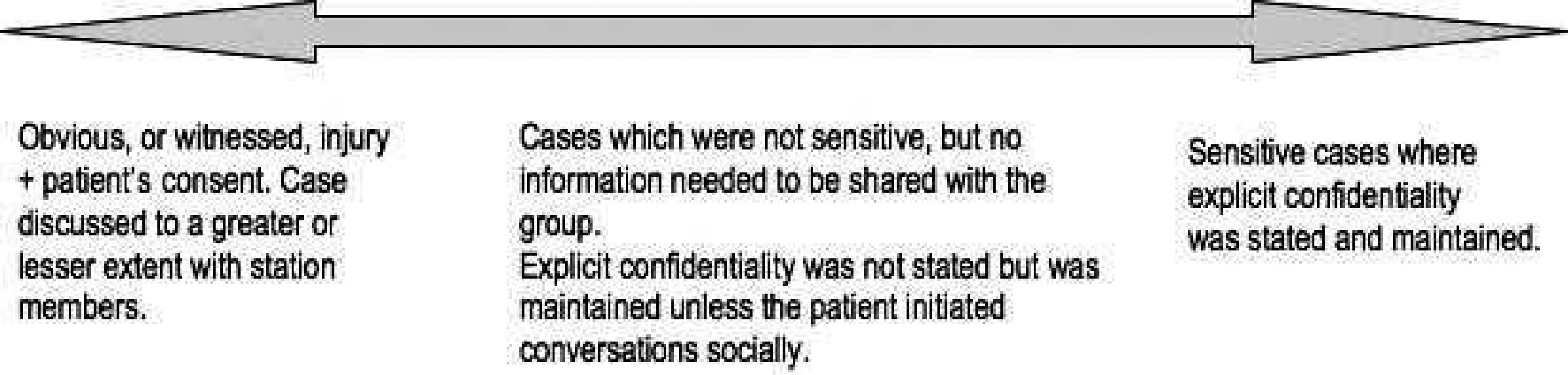
A continuum of confidentiality.
This situation was possibly damaging. The only cases that the community had a real awareness of my managing were the ones that were discussed openly. This had the potential to give the impression that all cases were discussed, rather than the reality that the minority were. This perhaps prevented a number of people from coming to see me because they were anxious about confidentiality not being kept. I think this was the minority of people, but I do worry that it was significant.
Another aspect of the group's expectation of confidentiality was the fact that I had a partner while at Rothera. Among some members of the group there was a belief that I would tell this man about aspects of my work during the day, as it was seen as natural for partners to do so. On a number of occasions I had the opportunity to refute this (twice in the bar and occasionally in consultations). When this was broached in social situations it was always in a joking manner about my partner knowing everything about people on base. I reacted to this in a very strong manner, not only because I wanted the message to be clear that I did not discuss my patients with him, but also because I was shocked that people would think I would do that. My partner at all times backed me up, jocularly saying, for example, that he tells me everything and I tell him nothing. The root of this issue was the basic misunderstanding of most of the base members about the role of the doctor and the rules of confidentiality she abides by.
Treatment and examination options
I was surprised how difficult it was to examine people in Rothera. Once again, this is because I had underestimated the difference between how people perceive doctors and doctors’ perception of themselves and their role. In order to perform my job I am relatively detached, especially during the acute consultation. This, of course, needs no enforcing while in the UK. You have limited time with patients in a very clearly clinical environment, and you usually have no history with them other than as doctor and patient. I felt very strongly that I wanted to maintain that detachment as far as possible. I conducted doc school and medical consultations in my clinic, but did not sanction any socializing such as drinking and parties that have happened in previous seasons. There were chatting sessions, but these tended to be of a mild supportive nature with a few individuals. I felt comfortable with that, and the confidentiality implied by the sessions being in the clinic was appropriate. While I maintained the aura of detachment when I was seeing someone professionally, this was not the case for my patients. My wintering group was fairly resistant to examination (the summer-only BAS employees demonstrated less of this reserve). It did not seem to be solely a gender issue, but more to do with familiarity. Both in my first and second summers, the winter group would actively seek out the new doctor for intimate physical problems and their own winter doctor for other issues. There is clearly a way around this and that is not to become too close with your winterers and effectively stay in the doctor role for a much higher percentage of the time, if not always. I cannot even begin to analyze what effects this would have had on my psyche over that prolonged period. Frankly, I do not believe I would have been able to do it. The effect on the base group as a whole would also be difficult to predict. It may have resulted in even lower help-seeking behavior because of concerns that I was not liked or was not a team player. I had a brief insight into what it must have been like to be that socially isolated while chatting with the doctor on the Polar Stern (the German Antarctic research ship) when it called into Rothera. The doctor had recently done a season at Neumayer (the German wintering Antarctic station) where he was the base commander and the physician, both roles that enforce detachment from the other station members. He described an intensely lonely year, a huge contrast to my relaxed and friendly experience at Rothera.
Treatment approaches were open to more manipulation by the doctor, and from reading the Rothera annual reports there have been a range of styles. There is very little limitation of treatment options with the incredibly well stocked clinic at Rothera, the pretour training of the doctor, and subsequent doc schools on base. However, I had an interesting balance to find regarding style, as the nature of the enclosed society offered more choice than the one enforced by the UK hospital environment.
The treatment style options fell into 3 main categories, which doctors must choose among, both as a general mentality and on a case-by-case basis. The professional approach—very similar to the role of the accident and emergency doctor. The initial consultation decided the treatment, follow-up was arranged as needed, the doctor role was then over until the patient was seen again professionally. The maternal/paternal approach—treatment and advice was given at the time of the consultation, but then the unique position of being a friend and living in an enclosed community enabled advice to be given on a regular basis, more questions to be answered, and less intense but more frequent follow-up to be done. The enforcement approach—treatment and advice were given in the consultation, but power was extended outside the clinic so that advice was enforced. For example, alcohol was banned, they were confined to base, their cigarettes were confiscated: this could be done by manipulation of the doctor's relationship with the patient only or by recruitment of the base commander and other base members or even BAS headquarters in the UK.
I think it is inaccurate to say that I chose one particular style of treatment. Rather, I fell into one style because of my personality and my relationships with people and because I had developed a precedent of talking to people about medical matters in a social setting. However, I actively decided NOT to employ the enforcement approach. I strongly felt that unless a patient was threatening the well being of another base member, or clearly and significantly threatening their own well being, I did not have the remit to enforce any of the advice I gave nor involve the base commander or other base members.
My natural style of treatment was the maternal approach. This worked well in most situations. I, in effect, traded any institutional power for greater truthfulness, more presentations, and potentially increased sway because of my personal relationship with my patients. I hope that more people came to see me because they knew that they would not be stopped from work or leisure pastimes unless their actions were clearly dangerous. This approach could be very frustrating when advice was not followed, but I chose to stay consistent. For example, when large amounts of cider were condemned because of can erosion, but still consumed by certain base members because it was free, it became almost a joke that I disapproved, but the behavior continued anyway. Perhaps this particular example is not wholly negative as it had the potential to enforce the idea publicly that I was separate from management and hence gained the trust I sought.
However no style is ever pure. Certainly in summer, operational requirements meant that I was asked whether people were fit for the field. Many decisions were based on this fitness evaluation. If I thought people should return from the field, they did, regardless of their views, and any concerns over fitness for SCUBA diving were, of course, acted on. So I did have some managerial influence, but in a very few circumstances.
24 hour on-call duties as a single-handed practitioner
Alcohol was a large part of Rothera life. I am not a teetotaler in the UK, but I do not drink a great deal.
As with the issue of treatment options, there were a number of options available to the doctors working in the Antarctic regarding alcohol use, and I was able to meet doctors who employed all 3 of these different approaches. The options were: Abstain from drinking and always be available for work (excluding winter training trip weeks). Abstain and be available at times of greatest risk, for example, sporting or operational risks or social risks such as party nights. At low risk times there is a spectrum from driving-limit drinking to completely unavailable. Unavailable intermittently, but this is independent of whether this is a high risk period. This applies especially to base-wide drinking nights.
Again, no option was necessarily the correct one. They all had their positive and negative points, and I think, within reason, the final choice of approach should rest with the doctor on the base. It could be argued that option 3 was not compliant with the expectation that the doctor was going to be available whenever needed, and indeed the guidance given to me before my departure by members of BASMU was to stay within the driving limit at all times. However one could argue that this would pose an artificial barrier to taking part in what was a very important part of station social life. Winter trips were allowed, putting the doctor days away from helping base members and indeed out of contact entirely until the nightly radio communications. Climbing recreational trips were also allowed, which put the doctor hours away from base. So it seems perhaps hypocritical to outlaw this social pastime that puts them away from being competent practitioners for a similar time period.
I chose option 2, which was a difficult path at times.
Social habits are difficult to break once they have been cemented. During the initial summer period, as there are 2 doctors on station, the work pattern resembles a traditional “on-call” rotation. When winter started I certainly felt the weight of the 24-hour responsibility, but I am someone who likes to be involved socially. There was also a renewed pressure to make friends and cement relationships within the newly rearranged group. I chose the option of drinking to below the driving limit if I did drink and being abstinent on high-risk organized party nights. Everyone knew this, and I think probably felt more comfortable that I viewed my role as 24 hours per day. But still I felt pressure to drink, which I only really became aware of when I was unable to drink for a 2-week period during a medical emergency and evacuation. 1 These were my friends and they wanted me to have fun, so they tried to reassure me that they did not want me to be sober at these nights, they wanted me to be involved. It proved very difficult to explain that I felt involved as much as I needed to without drinking to excess and that it was far more stressful for me to drink on these nights than not, because of the feeling of responsibility.
Relationships with patients
As discussed above there were many subtle ways in which my relationships with the group in Rothera affected their medical care. I have not yet addressed how the way I felt about individuals directly affected my provision of care to that individual. The short answer is that in the majority of cases, I do not think what I thought of patients personally affected how I treated them. There were 2 cases, however, where the interaction between my personal and professional relationship was interesting and challenging. These cases were at opposite ends of the spectrum; one individual I disliked, and the other I loved. Paradoxically, the case involving the one I loved caused the most problems.
In the first case, consultations with this person were perhaps more difficult than with other members of the base, but this was because he was a difficult patient with difficult presentations. The consultations were no more challenging than if I had been in general practice surgery in the UK with a complicated frequent attendee. What surprised me was that because of my strained and stressful personal relationship with him, I actually enjoyed my consultations with him much more than any interaction in a social setting. We immediately had a common topic to talk about, and we both had set roles of patient and doctor with the intimate feelings of respect and trust that come with that. Certainly for me I felt it “normalized” our relationship and I think for him also. The result was a good standard of medical care and intermittent improvements to our social relationship.
The second case involved my partner. I found providing medical care to him incredibly difficult. It seemed impossible to flip into professional mode in the clinic. When advice was not followed, it was difficult not to nag, but also follow-up was totally informal as discussions of progress naturally happened when we were together, but the social setting meant adequate history and examination was inappropriate and difficult. The result was possible substandard medical care and a reasonable amount of stress for both of us.
Conclusion
My 17 months down in Rothera were certainly challenging, but in ways that I had never considered while preparing in the UK. Conversely, aspects that I most worried about (I remember being really quite worried about exposing and developing radiographs) were very quickly mastered and enjoyed. There were a lot of things I should have done differently, but whether they would have significantly changed the service I was able to provide I do not know. The social dynamics of every group on an Antarctic base are so complex and individual that to try and envisage all the multiple effects that one change in policy can have is impossible. At the same time these social groups are remarkably robust, allowing mistakes to be made, lessons to be learnt, and changes to be made, all in that one short season.