
Abstract
Individual psychological responses to heights vary on a continuum from acrophobia to height intolerance, height tolerance, and height enjoyment. This paper reviews the English literature and summarizes the physiologic and psychological factors that generate different responses to heights while standing still in a static or motionless environment. Perceptual cues to height arise from vision. Normal postural sway of 2 cm for peripheral objects within 3 m increases as eye-object distance increases. Postural sway >10 cm can result in a fall. A minimum of 20 minutes of peripheral retinal arc is required to detect motion. Trigonometry dictates that a 20-minute peripheral retinal arch can no longer be achieved in a standing position at an eye-object distance of >20 m. At this distance, visual cues conflict with somatosensory and vestibular inputs, resulting in variable degrees of imbalance. Co-occurring deficits in the visual, vestibular, and somatosensory systems can significantly increase height imbalance. An individual's psychological makeup, influenced by learned and genetic factors, can influence reactions to height imbalance. Enhancing peripheral vision and vestibular, proprioceptive, and haptic functions may improve height imbalance. Psychotherapy may improve the troubling subjective sensations to heights.
Keywords
Introduction
Most people experience some degree of imbalance when exposed to heights. The term height imbalance is used synonymously with the terms height vertigo and height instability. All of these terms refer to the variable degrees of disequilibrium associated with exposure to heights. Some people dislike heights and may even have significant anxiety just thinking about them, whereas others like and even seek out heights. Is there something physiologically different between these individuals, or is it just a different psychological reaction to the same situation? This paper reviews the English literature on the physiology and psychology of height exposure while standing still in a motionless environment and suggests treatments to improve height imbalance.
Physiology of Height Imbalance
Our brain, both consciously and unconsciously, maintains an image of our bodies and the space around us called spatial orientation. An important consequence of spatial orientation is good balance. Balance requires the constant input of 3 sensory systems: visual, vestibular, and somatosensory. These 3 systems function in a complex, interactive feedback loop that can be significantly affected by emotions.
The somatosensory system has 2 important subsystems: proprioceptive and haptic. The proprioceptive subsystem senses the body's position and movement from the neural input from muscles and tendons of the torso and extremities. The haptic (touch or pressure) subcomponent provides powerful stabilizing feedback for postural control. 1 The vestibular system consists of the inner ear organ, which provides information on the relationship to gravity (head tilt) and acceleration or deceleration.
The visual system provides important binocular and monocular cues about the shape, size, distance, and movement of objects in the environment. It also provides cues about the movement of our own head relative to the entire visual scene. Depth or distance perception is the interpretation by the visual cortex of monocular cues (interposition, linear perspective, familiar size, relative size, motion parallax) and binocular cues (stereopsis, convergence, accommodation). 2 Height perception, in the visual system, is simply a special case of distance or depth perception. When standing still in a motionless environment, perceptual cues to height arise from vision.
With the overlay of emotions, these systems maintain posture while standing still (static or stationary posture) and are essential for moving within the environment. Static posture is a relative term, because in order to maintain optimal balance, some degree of normal sway results in perceptible visual cues that attenuate somatosensory and vestibular cues.
Our understanding of the effects of heights on balance (static posture) originates from the pioneering work of Brandt, Bles, Arnold, and Kapteyn. In a series of papers, 3 –5 these authors developed the theory that height imbalance is an interaction between visual distance cues and the perception of self-movement. Brandt et al 6 found that head movement results in movement of object images on the peripheral retina (visual flow). Liebowitz calculated that a visual flow movement threshold of 20 minutes of arc is required to detect movement. 7 When surrounding visual objects are within 3 m, normal head sway while standing still is commonly in the range of 2 cm, which achieves the threshold 20-minute arc on the retina. As eye-object distance increases, head sway increases proportionally. From these observations, Brandt et al 3 theorize that simple trigonometry predicts the relationship between normal sway and the distance of visual objects. To achieve the threshold 20 minutes of visual arc when objects were further than 3 m, head and body sway must increase (Figure).
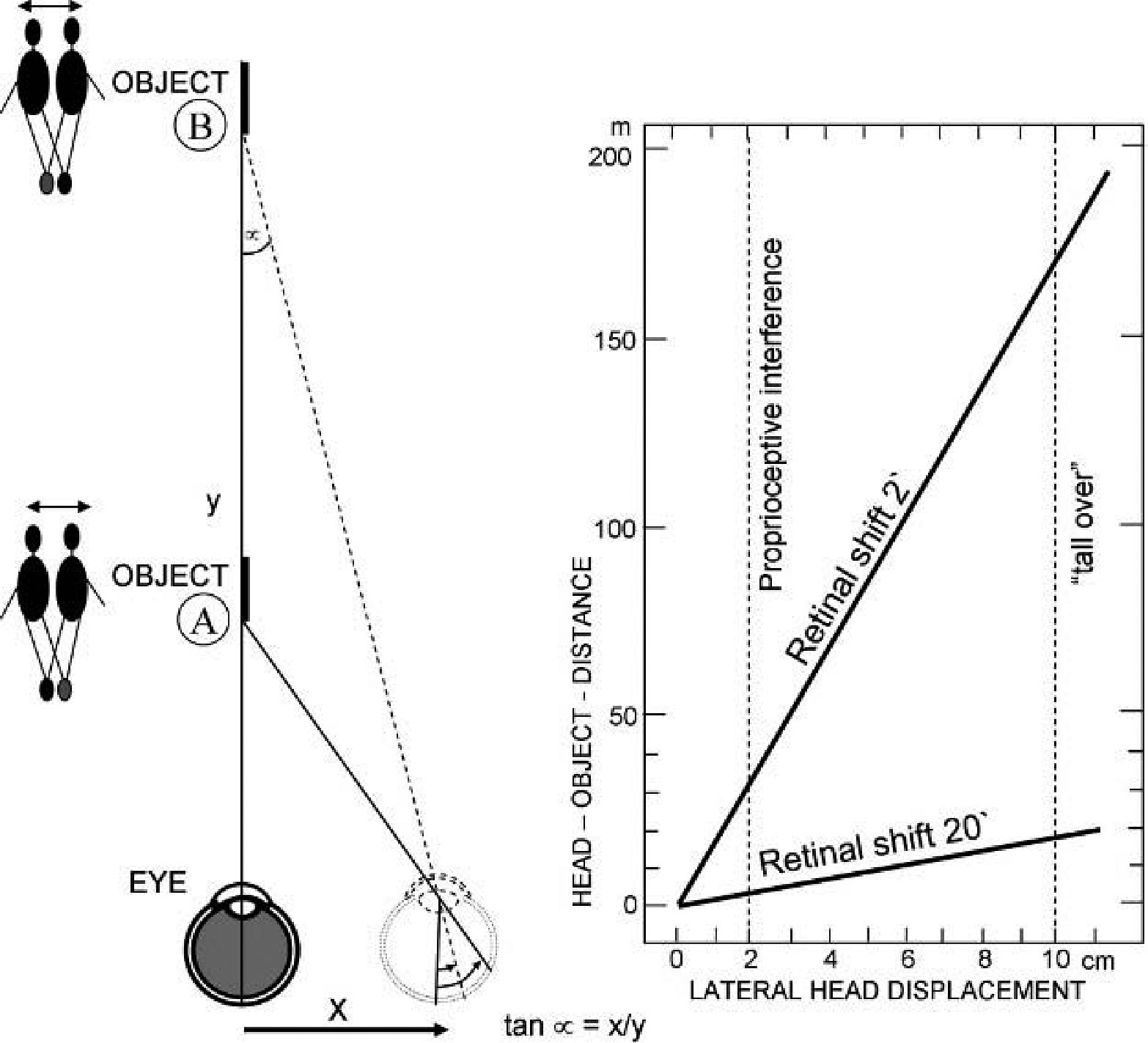
Diagram showing the relationship between head-object distance, y, and lateral head displacement, x, for given retinal displacement. Adapted from Brandt T, Arnold F, Bles W, Kepteyn TS. The mechanism of physiological height vertigo. I. Theoretical approach and psychophysics. Acta Otolaryngol 1980;89:515. Used with permission.
However, at 15 to 20 m, postural sway must be 10 cm, which exceeds the ability to remain in a static posture. In effect, visual distance/height cues saturate at this distance and provide conflicting information to the vestibular and somatosensory systems. In this situation, the vestibular and somatosensory systems must override the visual system to maintain balance. Although vestibular and somatosensory cues are adequate to maintain static postural stability, visual cues are essential to construct the rich spatial orientation humans need to stand erect and move in any environment.
Humans have evolved as terrestrial creatures from a horizontal to an upright posture. Brandt et al 3 show that after this evolutionary change, height imbalance became related to body position. Subjective height imbalance scores were greatest in the upright erect position and decreased progressively as posture changed to sitting, hands and knees, and finally lying positions. It can be argued that in the absence of posture (lying position), there is no postural sway, and only then is the head motionless. This would be the only situation in which height or depth perception is independent of self-motion.
Subjective height imbalance scores also increased with the overall elevation above the ground, up to a height of about 20 m. Above 20 m, subjective height imbalance scores reached a plateau. Brandt further showed that subjective height imbalance was independent of up or down gaze direction and was only dependent on eye-object distance. They therefore preferred the term distant vision imbalance to height imbalance.
Bles et al 5 used posturography to study the destabilizing effects of aberrant visual, proprioceptive, and vestibular inputs on overall body sway in static posture. They found increased sway (destabilization) with absent vision; height elevations of up to 5 m; movement of distant objects (visual destabilization), platform incline from horizontal, soft foam platform (somatosensory destabilization); and head tilt of ≥30° (vestibular-otolith destabilization). They also found that destabilized subjects were much more sensitive to fore-aft sway than to lateral sway. Carpenter et al 8 also used posturography to study young healthy adults at relatively low heights of 0.19 m vs 0.81 m and demonstrated increased ankle stiffness manifested by decreased fore-aft amplitude with increased height. Bles 5 found no difference in overall body sway pattern measurements at altitudes of 20, 50, and 100 m. At these elevations, visual cues were saturated. Interestingly, they also found no difference between individuals who were height intolerant and those who were height tolerant (tight rope performers).
Based on these studies, it appears that the intensity of height-induced imbalance is a function of the magnitude of eye-object distance and the interaction between visual, vestibular, and proprioceptive systems. As a consequence, height imbalance would be expected to increase if one of the sensory systems is eliminated or deficient. Even individuals with intact sensory function may experience greater height imbalance if environmental factors decrease the effectiveness of sensory cues. For example, depth perception becomes more difficult at dusk or dawn when ambient light decreases. Unstable or irregular surfaces may decrease somatosensory cues. Atypical head attitudes (tilting the head when rock climbing) may provoke unusual vestibular cues. In addition, it has long been known that vestibulotoxic agents, such as alcohol and quinine, can impair vestibular cues for several hours or days after ingestion.
When sensory cues are sparse, Lackner and DiZio 1 have shown that the simple act of touching (haptics) a stationary surface can greatly improve balance. For example, light touch with a single finger to a non–weight bearing object can reduce postural sway by as much as 50%. They also suggest that haptic inputs reinforce cognitive representations and assumptions about the environment. Assurances about the accuracy or inaccuracy of balance aid in developing anticipatory strategies that influence subsequent movement.
In cases in which the construct of the external world is uncertain, there is more value in interrogating all sensory inputs. This is why height imbalance is associated with increased postural sway. Not only does increased sway maximize the potential for self-induced visual cues, but also it increases available somatosensory (ankle proprioceptive and planter foot surface pressure), as well as vestibular cues. When somatosensory and vestibular cues do not resolve ambiguities in spatial orientation, the threat of losing one's balance and falling increases. In some individuals, this can become a self-reinforcing loop. In experiments exposing subjects to various heights, some were modestly disturbed; others demonstrated increased sway and anxiety; and still others moved into a prone position, lying on the ground to resolve their balance ambiguities. 3 –5
Common to these reactions is the psychological sense of danger. When normal terrestrial clues to balance are in conflict, perceived fall risk increases and a feeling of danger is appreciated. Bles 5 found that subjects exhibited a wide range of interindividual variability but a narrow range of intraindividual variability. This would suggest that the psychological response of height intolerance vs height tolerance in otherwise physiologically “normal” individuals may be based on different psychological factors.
Psychology of Height Tolerance
Individual psychological reactions to heights vary from acrophobia, height intolerance, height tolerance, and height-seeking behavior. The reasons for these different responses are complex and only partially understood. Less than 10% of individuals with height intolerance have true acrophobia. 9 Acrophobia by definition is a phobic disorder manifested by anxiety when even imagining a height situation. Phobic individuals often have generalized increased anxiety to stressful or dangerous situations once thought to be precipitated by a conditioned unpleasant experience to heights as a child. Menzies and Clarke, 9 however, demonstrated that this is an uncommon cause of height phobia and suggest a Darwinian explanation that reasons that the species will show fear to a set of evolutionary relevant stimuli, such as height, on their first encounter and over time this fear diminishes due to habituation. Poor habituators or those with insufficient safe exposure experience persistent fear.
The height-intolerant individual is otherwise normal and is only bothered by heights when actually exposed to them, not an imagined exposure. Some of these individuals also have proprioceptive, vestibular, or visual deficits that impair their balance even in nonheight situations. Others have normal balance functions and simply interpret height imbalance as physically fearful and avoid such situations. Maki 10 has shown that a generalized increase in anxiety or arousal has been associated with adaptation in postural control.
Height-tolerant individuals perceive the physical danger of heights but compensate either by habituation or a comfort level with their sense of physical danger. Height-seeking individuals actually enjoy the sense of physical danger when exposed to heights. These are the individuals who are the “adrenaline junkies,” sensation seekers, or risk takers/risk seekers. Much descriptive literature has been written on the risk taker, but less information exists on the cause or reason for this behavior. 11 –17
The traditional definition of risk is the “possibility of loss or injury.” Many people perceive risk as negative and maintain themselves in secure environments with little diversity to minimize their risk. To others, risk taking provides positive benefits. There is generalized agreement that risk or sensation seeking is a basic personality dimension. It leads to explorativeness and is probably necessary for the evolutionary survival of the species. During evolution, men competed for social status and resources to attract mates. Therefore, it is not surprising that men take greater risks than women. 11 Too much risk taking, however, may lead to hyperactivity and even death. Too little risk taking may lead to stagnation. Antarctic explorer Sir Ernest Shackleton was able to recruit his Endurance crew with an ad promising, “Small wages, bitter cold, long months of complete darkness, constant danger, safe return doubtful.”
Risk takers seem to form 2 major groups: the impulsive risk taker and the contemplative risk taker. 11 –15
Both have the same drive to experience the “adrenaline rush” or heightened sensation of danger. Both impulsive and contemplative risk takers tend to be individuals with a high sense of self-security or -confidence, who are self-assured, and who easily rebound from failure and try again.
The impulsive risk taker acts impulsively when a situation presents itself without forethought or planning. This individual tends to emotional swings; is unaware or unconscious of motivation; tends toward wishful thinking; and follows a favorite plan, even though it is not useful. There appears to be a destructive group among the impulsive risk takers who seek immediate gratification commonly found in drug addiction and gambling.
In contrast, the contemplative risk taker carefully calculates the risk with forethought and planning to minimize any adverse outcome. These individuals contain their emotions and tend to know their personal emotional and physical abilities. They believe themselves in control of most of the risk and therefore experience “danger” as high arousal or excitement rather than fear. When they succeed, they have a sensation of self-satisfaction derived from control of a dangerous situation that they perceive as challenging rather than threatening. A situation that involves risk without personal control (gambling) is not likely to appeal to the contemplative risk taker. In summary, they have been described as “confident and physically adventurous risk taker[s] motivated by sensation seeking and mastery needs.” 18
In the business world, risk takers are the innovators and entrepreneurs. The impulsive risk takers are often the individuals with rollercoaster careers of success and failure, whereas the contemplative risk taker's successes outweigh the failures. It is interesting that the business or intellectual risk taker is often not the physical risk taker and vice versa. Furthermore, the physical risk taker may be very selective in the activities he or she likes or dislikes, such as rock climbing but not skydiving.
The term hormesis describes the beneficial effect of repeated stimulation and stress by partial failure. 19 Risk taking leads to stress, failure, and variety, all of which keep individuals complex and provide hormesis. Aging often evokes complacency in lifestyle activities, which can decrease complexity and sensation seeking or risk-taking behaviors. It follows that aging is associated with a decrease in height tolerance.
The etiology of risk-taking behavior seems to be “hard wired,” because most of these relevant personality traits are evident in childhood. Identical twin studies have suggested a 60% genetic contribution to risk-/sensation-seeking behavior, 11 which is high, because most personality traits tend to show a 30% to 50% genetic inheritance. Some evidence indicates that these individuals have a dopamine deficiency and their behavior is an effort to lessen this deficiency. 11 –13,16 Von Knorring 12 found low platelet monoamine oxidase activity, an indirect measure of central nervous system serotonin activity, in sensation seekers. Ebstein et al 17 found a gene for “novelty-seeking behavior” associated with the dopamine receptor 4 gene. High-risk situations give these individuals extra dopamine, adrenaline, and cortisol, which lead to increased alertness.
Genetic control is further supported by epidemiologic studies suggesting that, as a group, risk takers tend not to get Parkinson's disease, a disorder known to be associated with dopamine deficiency. Parkinson's patients tend to have more conservative personalities. 16 Risk taking, like caffeine and nicotine, may improve the health of the brain's dopamine system and therefore protect against Parkinson's disease.
Treatment of Height Imbalance
The treatment of height imbalance is dependent on both physiologic and psychological variables.1,3,5,20–23 A height-intolerant person's gaze should avoid distant moving objects and include near objects within the peripheral vision. Commonly worn corrective progressive/bifocal glasses or glasses that decrease peripheral vision, such as glacier glasses, should be avoided, because they may distort or restrict near-peripheral vision (the ground) when looking ahead. Sitting, kneeling, or lying improves height imbalance and, if done for a period, may fatigue or habituate the destabilizing effect of visual misinformation and fear. Standing on a stable platform, a horizontal surface perpendicular to gravity rather than a sloping surface, and wearing stabilizing boots (firm soles and ankle support) tend to improve proprioceptive cues. Avoiding head tilt positions of ≥30° (right, left, down, and especially up) 5 tends to improve vestibular response to heights.
Avoiding alcohol and other vestibulotoxic drugs may also help height intolerance. Light touch to any stationary object dramatically improves postural stability, even when deficits in other systems are present. Holding a hiking stick or other stationary object is helpful, even when the object is not used for support. 1 Individuals with visual, vestibular, or proprioceptive deficits may limit these deficits with physical and balance therapy. 21
Psychological therapy for height problems is limited to psycho/behavioral therapy and not drugs, except in the high-anxiety/phobic individual. 22 Behavioral therapy with virtual reality or prolonged safe situational exposure often will habituate and fatigue adverse psychological height responses. 22
Conclusions
Individualized reactions to visual height cues involve complex physiologic and psychological relationships. Eye-object distance of >20 m in a stationary position provides visual misinformation to the somatosensory and vestibular systems and may provoke height imbalance. The individual's psychological makeup, both learned and genetic, results in an interpretation of the imbalance sensation as either a degree of fearful danger or as challenging and even pleasurable excitement. The continuum of responses ranges from acrophobia to height intolerance, height tolerance, or even height-/risk-seeking behavior. Enhancing peripheral vision and vestibular, proprioceptive, and haptic functions may improve the physiologic responses to heights. Psychotherapy may improve the psychological response to heights.