
Abstract
Objective
Altitude-related cough is a troublesome condition of unknown etiology. Inhaled tussive agents are used to quantify cough, and the citric acid cough threshold has been shown to fall on ascent to altitude. Cough can occur in patients taking angiotensin-converting enzyme inhibitors due to stimulation of airway sensory receptors by increased levels of bradykinin. We hypothesized that increased levels of bradykinin could be responsible for the decrease in citric acid cough threshold on exposure to altitude and a possible etiologic factor in altitude-related cough.
Methods
Twenty healthy volunteers underwent baseline tests at 700 m before a 2-week stay at 3800 m. Angiotensin-converting enzyme activity and plasma bradykinin were measured at baseline and altitude. Citric acid cough threshold and nocturnal cough frequency were measured at baseline and throughout the 2 weeks at altitude.
Results
Citric acid cough threshold fell from 3.7 g/dL at baseline to 2.1 g/dL on the second day at 3800 m (geometric mean difference 1.8, 95% CIs 1.0–5.0, P = .025) and remained reduced throughout the stay at altitude. Nocturnal cough frequency was unchanged compared to baseline. Plasma bradykinin fell from 0.43 ng/mL at baseline to 0.08 ng/mL at altitude (geometric mean difference 5.7, 95% CIs 2.1–15.5, P = .002), but angiotensin-converting enzyme activity was unchanged (mean difference 0.06, 95% CIs –2.7–2.8, P = .97). There was no correlation between plasma bradykinin and citric acid cough threshold.
Conclusions
Increased levels of bradykinin are unlikely to be a significant factor in the increased sensitivity to citric acid seen in hypobaric hypoxia. Further studies are required to elucidate the etiology of altitude-related cough.
Introduction
Anecdotal reports have long existed of a troublesome paroxysmal cough affecting visitors to high altitude. In the first systematic study of altitude-related cough, nocturnal cough frequency and sensitivity to the inhaled tussive agent citric acid were increased in a group of subjects ascending to 5300 m in the Nepalese Himalaya. 1 Traditionally, altitude-related cough was attributed to the inspiration of cold, dry air, but during Operation Everest-COMEX, a hypobaric chamber study mimicking an ascent of Mount Everest, nocturnal cough frequency increased and citric acid cough threshold fell, despite careful control of temperature and humidity in the chamber, refuting cold, dry air as the sole cause of cough at altitude. 2 Other possible etiologies (eg, water loss from the respiratory tract, high altitude pulmonary edema, bronchoconstriction, respiratory tract infection, postnasal drip) have been discussed in a recent review. 3
The precise neuronal pathways that mediate the citric acid cough challenge remain debated but involve stimulation of airway sensory nerves, such as airway rapidly adapting receptors. 4 Cough is a well-recognized side effect in a proportion of patients taking angiotensin-converting enzyme (ACE) inhibitors and is thought to be due to sensitization of airway rapidly adapting receptors by increased levels of plasma bradykinin and substance P. 5 In human serum, the majority of bradykinin metabolism occurs via ACE. The early literature on the response of serum ACE activity to hypoxia in humans is confusing and contradictory. 6 Nothing is known about what happens to bradykinin at altitude beyond exposure to 1 hour of normobaric hypoxia. 7 However, if overall ACE activity falls, the result would be increased levels of bradykinin, which could sensitize airway sensory nerve endings.
We therefore hypothesized that the decrease in citric acid cough threshold on exposure to hypobaric hypoxia is due to increased bradykinin levels’ sensitizing airway sensory receptors and that this is an etiologic factor in altitude-related cough.
Methods
Subjects
Twenty male Kyrgyz altitude-naïve lowlander volunteers (age range 18–35 years) underwent baseline (BL) tests in Bishkek, Kyrgyzstan (altitude 700 m) before being transported by road in 7 hours to an altitude of 3800 m in the Tian Shan Mountains. Subjects remained at 3800 m for 2 weeks, as reported previously, 8 during which time they were essentially sedentary. All subjects gave written informed consent, and the project was approved by the ethics committee of the Faculty of Medicine of the Free University of Brussels in Belgium.
Citric Acid Cough Challenge
Solutions of increasing concentrations of citric acid in 0.9% saline were inhaled via an ultrasonic nebuliser (Sonix 2000, Clement Clarke International, UK) during a slow vital capacity inspiration over 5 seconds. 2 The cough threshold was defined as the lowest concentration that provoked a cough, providing that a cough was also provoked at the next concentration. Cough challenges were performed at BL in Bishkek and on the 2nd (HA02) and 15th (HA15) days at 3800 m and on return to BL (RBL) in Bishkek.
Nocturnal Cough Monitoring
Nocturnal cough frequency was measured using portable voice-activated tape recorders (Panasonic RQ-L317, Osaka, Japan), as previously described. 2 Recordings were made on consecutive nights at BL and on HA01, HA02, HA12, and HA13 nights at 3800 m. The mean of the results from each pair of nights is reported as the nocturnal cough frequency. For logistical reasons, it was not possible to obtain recordings on RBL.
Blood Sampling
Blood samples were taken in the morning at BL and on HA02 at high altitude. Blood was taken from a vein in the antecubital fossa after the subject had rested, sitting, for 30 minutes. Blood was collected into EDTA tubes and then centrifuged for 15 minutes at 1600g in tubes containing aprotinin (0.6 TIU/mL of blood). The collected plasma was stored at −70°C until analysis.
Plasma Bradykinin Assay
Plasma bradykinin concentration was analyzed using a bradykinin enzyme immunoassay kit (Phoenix Pharmaceuticals, Belmont, CA). Absorbance was read on a Bio-Rad microtiter plate reader at 450 nm.
Angiotensin-Converting Enzyme Activity Assay
Serum ACE activity was assayed by hydrolysis of the specific substrate Z-Phe-His-Leu. The fluorogen o-phtaldialdehyde was then added, and fluorescence emission was measured at 500 nm. Angiotensin-converting enzyme activity was calculated and expressed as mU/mL of serum.
Clinical Data
Heart rate and oxygen saturation (Nellcor N20P pulse oximeter, Nellcor-Puritan Bennet Ltd, Warwick, UK) were recorded on the morning of each measurement day during a general clinical interview and examination. Acute mountain sickness was assessed using the Lake Louise consensus self-assessment scoring system. 9
Statistical Analysis
Normality was assessed using the Kolmogorov-Smirnov test. Angiotensin-converting enzyme levels and heart rate were normally distributed. Bradykinin levels and citric acid cough threshold were not normally distributed but were successfully log transformed. The acute mountain sickness score, oxygen saturation, and nocturnal cough frequency were not normally distributed, and neither could they be normalized by transformation. Angiotensin-converting enzyme and bradykinin levels were compared using paired t tests, and citric acid cough threshold and heart rates using repeat measure analysis of variance with posthoc analysis performed using the Bonferroni test. They are presented as means or geometric means and 95% CIs. Nocturnal cough frequency, acute mountain sickness scores, and oxygen saturation were compared using repeat measure analysis of variance on ranks with posthoc analysis performed using the Student-Newman-Keuls test and are presented as medians and ranges. Analyses were performed using SigmaStat 2.0 software (Jandell Corporation, San Rafael, CA).
Results
Completeness of Data
Due to a technical problem with the assay, bradykinin analysis was only possible on samples from 14 of 20 subjects. Citric acid data were obtained from 18 of 20 subjects. Nocturnal cough frequency recordings were obtained from 19 of 20 subjects at all altitudes. Two subjects were excluded from analysis because their BL cough frequencies in Bishkek were very high and remained high throughout the study compared with any other subject.
Citric Acid Cough Threshold
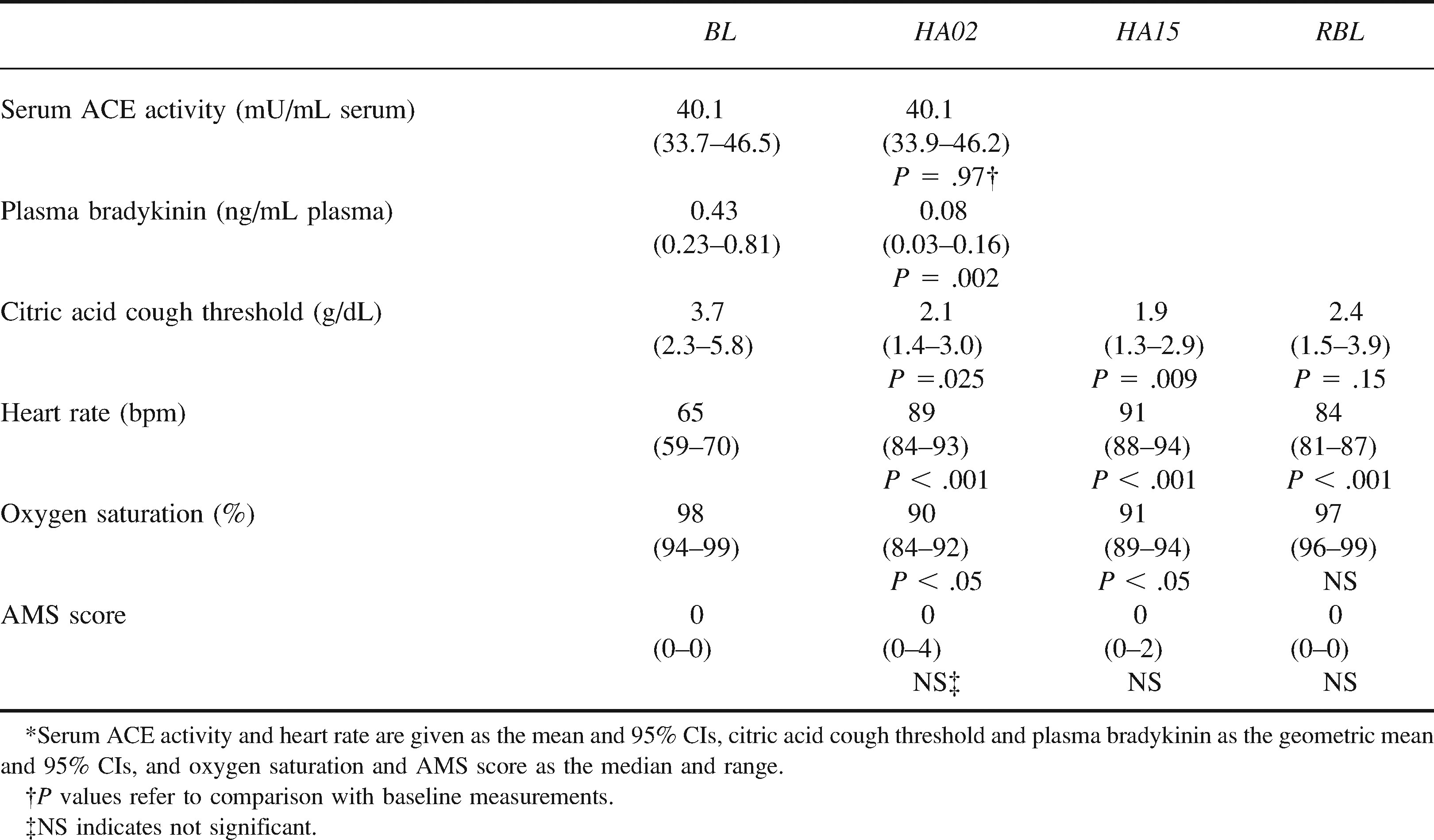
Compared with BL, citric acid cough threshold fell at HA02 (geometric mean difference 1.8, 95% CIs 1.0–5.0, P = .025) and HA15 (geometric mean difference 1.9, 95% CIs 1.1–3.4, P = .009). Although still reduced on return to the BL altitude, the reduction was not statistically significant (geometric mean difference 1.5, 95% CIs 0.9–2.7, P = .15). These results are summarized in the table.
Serum angiotensin-converting enzyme (ACE) activity, plasma bradykinin, citric acid cough threshold, heart rate, oxygen saturation, and acute mountain sickness (AMS) score at baseline (BL), on 2nd (HA02) and 15th (HA15) days at 3800 m, and on return to baseline (RBL)*
Nocturnal Cough Frequency
There was no change in nocturnal cough frequency between BL (median cough frequency 0.5, range 0–4.5) and HA01/HA02 (median cough frequency 1.0, range 0–5.5) and HA12/HA13 (median cough frequency 0, range 0–5.5).
Plasma Bradykinin Levels and Angiotensin-Converting Enzyme Activity
Plasma bradykinin concentrations fell from BL to HA02 (geometric mean difference 5.7, 95% CIs 2.1–15.5, P = .002). There was no change in serum ACE activity (mean difference 0.06, 95% CIs –2.7–2.8, P = .97). These results are summarized in the table.
Clinical Data
Compared with BL, heart rate increased at HA02 (mean difference 24 bpm, 95% CIs 16–32, p<0.001) and HA15 (mean difference 26, 95% CIs 19–34, P < .001) and remained elevated at RBL (mean difference 19, 95% CIs 12–27, P < .001). Oxygen saturation fell at HA02 and HA15 compared with BL (both P < .05). The acute mountain sickness self-assessment score did not significantly increase during the stay at altitude. These results are summarized in the table.
Correlation Analysis
There was no relationship between citric acid cough threshold and bradykinin levels, heart rate, or oxygen saturation or between the changes in citric acid cough threshold and bradykinin levels.
Discussion
As in previous studies,1,2 we have demonstrated a fall in citric acid cough threshold on ascent to altitude, but this study extends these previous findings to show that the increased sensitivity to citric acid occurs at the lower, more frequented altitude of 3800 m. The citric acid cough threshold remained reduced throughout the 2 weeks at 3800 m and returned to control levels on descent from altitude. The fall in citric acid cough threshold was not, however, accompanied by a change in nocturnal cough frequency. This is consistent with the clinical observation that subjects were not troubled by cough during the study period. Plasma bradykinin fell by approximately 81% on day 2 at 3800 m compared with its control value, although serum ACE activity did not change. There was no relationship between citric acid cough threshold and plasma bradykinin levels, heart rate, or oxygen saturation.
Bradykinin is produced by plasma kallikrein from both high- and low-molecular-weight kininogen. It may also be generated by aminopeptidase-mediated cleavage of kallidin peptides, and other enzyme pathways may operate in certain disease states. Kallikrein activity is controlled principally by a number of inhibitors, including C1-inhibitor, α-2 macroglobulin, and antithrombin III. 10 There is no available evidence on the effects of hypoxia on the kallikrein-kinin system, and what evidence exists on the changes in the coagulation system indicate that hypoxia per se has minimal effects. 11 The kallikrein-kinin system is predominantly tissue based, and tissue levels of bradykinin exceed those in blood. However, changes in plasma levels of bradykinin have been shown to parallel those in the tissues. 12
Previous work on ACE activity in hypoxia is contradictory. Some studies demonstrate no change in ACE activity on exposure to hypoxia; some studies demonstrate a fall in activity; others demonstrate a biphasic response with an initial fall in activity followed by a return to baseline values. 6 These differences reflect technological uncertainties, small subject numbers, and the widely different conditions under which ACE activity was measured, ranging from acute exposure to normobaric hypoxia of only 10 minutes to a field study on Everest lasting 4 weeks. 6 It is not possible to measure lung ACE activity in living human subjects, and we therefore chose to use serum ACE activity as a surrogate marker of overall lung activity. There are limitations to this approach, although measurement of whole lung and serum ACE activity in dogs during exposure to chronic hypoxia yielded comparable results. 13 The most feasible explanations for the dramatic fall in plasma bradykinin levels seen in this study are that serum ACE activity did not parallel an increase in local tissue ACE activity and that a local tissue increase in ACE activity in, for example, the pulmonary endothelium 14 was responsible for the fall in plasma bradykinin or that it was metabolized by a kininase other than ACE. Despite being unable to explain the mechanisms behind the fall in bradykinin seen in this study, we can tentatively exclude an increase in plasma bradykinin as the cause for the increase in sensitivity to inhaled citric acid seen in this and previous papers.
Although there was a fall in citric acid cough threshold on ascent to 3800 m, we were unable to demonstrate any clinical increase in cough frequency, despite the magnitude of the change in citric acid threshold being comparable to previous work at altitude. 2 One possible explanation for this finding would be an alteration in nebulizer output due to reduced barometric pressure. Barry 15 assessed the output from the ultrasonic device used in this study in a hypobaric chamber. It fell by only 23% at 4200 m and 13% at 5300 m compared with sea level. In a further study, serum salbutamol levels were measured in human subjects after ultrasonic-nebulized administration of salbutamol. 16 There was no difference in serum salbutamol levels between sea level and a simulated altitude of 5000 m. These findings argue against changes in nebulizer output's being responsible for the change in citric acid cough threshold reported here.
The increased sensitivity to citric acid in the absence of a clinical change in cough is an important finding, because the study was performed at an altitude of 3800 m, which is more frequented than the higher altitudes of previous studies.1,2 It suggests that the pathophysiologic process that is responsible for altitude-related cough is operating even before clinical cough is apparent. The inhalation of nebulized citric acid and the threshold concentration that produces cough is a well-recognized method of measuring the sensitivity of the cough reflex and induces cough in a dose-dependent and reproducible manner. 17 Citric acid stimulates airway sensory nerves, such as rapidly adapting receptors, which constitute a heterogeneous group known to be activated by a number of stimuli, including gaseous or aerosolized irritants, inflammatory and immunologic mediators (eg, bradykinin), edema, and atelectasis. 4 It has recently been suggested that the term altitude-related cough may cover at least 2 conditions: a cough that can occur at lower altitudes, which is related to exercise and possibly trauma or infection of the respiratory tract, and a cough that is only a clinical problem at higher altitudes and that may be due to subclinical pulmonary edema's stimulating airway sensory nerves or changes in the central control of cough. 3 None of our subjects, who were predominantly sedentary throughout the study, exhibited any clinical signs of respiratory tract infection. In addition, as previously described, 8 the subjects performed nasal lavage with 0.9% sodium chloride solution morning and evening, and vasomotor rhinitis and postnasal drip were not a problem. This excludes trauma or infection of the respiratory tract as a cause for the alteration in citric acid cough threshold seen in this study.
Respiratory control undergoes profound changes on exposure to high altitude, and although the central control of cough is poorly understood, a number of factors that suppress cough also suppress ventilation.18,19 A relationship at sea level has been reported between the hypercapnic ventilatory response and cough threshold to hypotonic saline. 20 It has been suggested that changes in ventilatory control on ascent to altitude could influence or parallel central changes in the control of cough. 3 However, a recently published study could demonstrate no correlation between hypercapnic ventilatory response and the citric acid cough threshold on ascent to 5200 m. 21
Finally, the increase in sensitivity to citric acid in the absence of clinical cough could represent early subclinical pulmonary edema. Considerable evidence exists to support the presence of subclinical pulmonary edema at high altitude, and the 2 most likely etiologic mechanisms are hypoxic pulmonary vasoconstriction, resulting in an increase in pulmonary capillary pressure, and altered respiratory epithelial ion transport. 8
In conclusion, we have demonstrated a decrease in citric acid cough threshold in a group of individuals during a 2-week stay at the relatively moderate altitude of 3800 m. The change in citric acid cough threshold was not due to altered plasma bradykinin levels, which fell on ascent to altitude. More studies are required to elucidate the mechanism of altitude-related cough.
Footnotes
Acknowledgments
We are grateful to Pascale Jespers and Marie-Therese Gautier of Erasme Hospital, Brussels, Belgium, and Dr Peter Barry, Judith Jackson, and Judy White of the University of Leicester, UK, for their invaluable assistance during preparation for the project; the members of the Kyrgyz Presidential Guard who participated in the study and the staff of Kumtor Gold Mine, Kyrgyzstan; and in particular Dr Francois du Toit, without whose help the project would not have been realized.
Funding
This work was supported by grant no. 3.4567.00 of the Fonds de la Recherche Scientifique Médical of Belgium. Some of the data presented in this paper were previously published in abstract form (Am J Respir Crit Care Med. 2002;165:A830).