
Abstract
Objective
The purpose of this study was to determine the impact of a nationally developed snakebite treatment protocol on the amount of anti snake venom (ASV) used in treating snakebites in a developing country and its effect on mortality. In addition, basic epidemiology data were collected and analyzed.
Methods
Experts in Indian snakebites developed a protocol specifically designed for snakebite treatment in India. A training program was implemented in Midnapore Medical College in West Bengal, India, under the direction of the Health Minister to train care providers in the new protocol. After training, data were collected for 839 snakebite victims over a 12-month period and included epidemiological data, ASV volumes administered, and mortality. The results were collated and compared with results calculated from 780 snakebite victims treated during the 12-month period before implementation of the protocol. Treatment prior to protocol implementation was based on knowledge gained by the care providers from western and forensic medicine textbooks.
Results
Protocol-guided treatment resulted in a 66% decline in the amount of ASV administered to victims. Fewer victims received ASV based on rational guidelines for assessing envenomation, dosage and repeat dosage, and clear endpoints to ASV therapy. In addition, there was a trend towards reduced mortality and an absolute reduction of 24%.
Conclusion
Use of the protocol reduced ASV utilization and the number of deaths. Locally developed protocols should be encouraged by such organizations as the World Health Organization and national and state governments and should be established with significant input from local experts.
Introduction
The snakebite problem in the developing world remains a seemingly intractable problem. In the last few decades, scores of textbooks, journals, and conferences have focused on means to reduce current mortality levels. West Bengal, India, has a long-standing reputation for having a serious snakebite problem. 1 The area's principal snakes of medical importance are the Russell's viper (Daboia russelii), spectacled cobra (Naja naja), monocled cobra (Naja kaouthia), common krait (Bungarus caeruleus), Wall's Sind krait (Bungarus sindanus walli), and banded krait (Bungarus fasciatus).2,3
In September 2006, the Health Minister of West Bengal authorized the introduction of an Indian-developed snakebite protocol for use in the state government hospitals. In addition, a program of workshop-based training in the use of the protocol was undertaken. The new local protocol used in this study was developed from the clinical observations of a large number of experts throughout India and was subsequently adopted as the Indian National Snakebite Protocol in October 2007.
Prior to the introduction of the new protocol, a large number of individual approaches/protocols were employed by doctors, even within the same ward team, based on information derived from a variety of sources, including Western and indigenous textbooks. 4 –12 A survey of doctors’ knowledge of how to treat snakebites, including the knowledge of doctors from West Bengal, demonstrated that 68% of Indian and Pakistani doctors relied on a US textbook, whereas 43% relied on forensic medicine textbooks written by medical authors with little practical experience encountering snakebites. 13 In addition, 38% of doctors admitted they were not confident in their ability to treat snakebites. 13
The purpose of this study was to evaluate the effect of the introduction of the new nationally developed protocol on snakebite management, particularly on the outcomes and the volume of overall usage of anti snake venom (ASV) in Midnapore Medical College which is situated in West Midnapore, a District of West Bengal with one of the highest snakebite mortality rates in India. 1 In addition, the study was intended to establish the demographic and epidemiological profiles of snakebite in the district.
Methods
The study was carried out at Midnapore Medical College, Midnapore, West Bengal, India. Midnapore Medical College has a catchment area of both East and West Midnapore Districts with a combined population of 8.3 million people. Rural farmers comprise 89.5% of the population, and the male to female ratio is 51:49. 14 The principal crop is rice.
A data collection proforma was prepared and used for retrospective review of cases treated from October 2005 to September 2006 before the new protocol was instituted (historical controls). The proforma was also used to prospectively capture data from new admissions treated under the new protocol from October 2006 to September 2007.
Ethical approval for this study was given by the Health Department, Government of West Bengal, India.
Protocols
Prior to institution of the study protocol, snakebite management varied widely between doctors and was based on their standard medical education. It was characterized by
13
: Anti snake venom administration criteria of local swelling, local swelling plus bite marks, bleeding from any site (including bite marks), incoagulable blood measured by a variety of methods, visible neurological signs, and signs of renal failure (eg, high serum creatinine on admission)4,9–11,15,16 Clotting tests carried out using a number of different methods (including capillary tubes and old drug ampoules)4,7,17 Repeat doses of ASV continued while any sign or symptom persisted (eg, swelling, respiratory insufficiency, renal failure)
8
Inconsistent guidelines as to end points for ASV therapy
8
Anti snake venom reactions handled by test dosing and administering hydrocortisone and antihistamine7,8
The new protocol included: Anti snake venom administration criteria limited to presence of incoagulable blood, visible neurological signs, and severe current swelling (ie, swelling rapidly crossing a joint or involving half the bitten limb)
20
Coagulation testing performed with the 20-minute whole blood clotting test in a new, clean, dry, glass test tube on a 6-hourly basis once ASV was administered20,21 Anti snake venom initial dosage of 10 vials based on empirical estimation of average initial dose of venom injected20,22 Viperine bites reassessed for ASV on a 6-hourly cycle until coagulation was restored9,20 Upper limit on ASV dosage for viperine bites set at 30 vials of Indian polyvalent ASV, based on amount required to neutralize maximum possible circulating venom
20
Neurotoxic bites reassessed after 1 to 2 hours and second dose of ASV given if symptoms unimproved or progressing
20
Twenty vials set as upper limit on ASV dosage for neurotoxic bites to neutralize maximum possible circulating venom
20
Anti snake venom reactions handled with intramuscular adrenaline (0.5 mg 1:1000) at the first sign of a reaction, with a repeat dose after 10 minutes if required; ASV test doses were abandoned20,23–26
Snakebite Management Training
A 3-hour training workshop was carried out at the hospital by experts involved in developing the protocol. The workshop included approximately 80 staff from all levels of health care provision at the hospital responsible for managing snakebite patients and covered venomous snake identification, snakebite first aid, envenomation identification, dosage of ASV, ongoing management (including assessment of repeat doses of ASV), and clinical endpoints for ASV therapy. It was explained to the audience that the new method was to be used to manage all snakebites coming to the hospital.
Statistical Analysis
The chi-square test (without continuity correction) was applied to compare proportions between the 2 years of interest.
Results
Anti Snake Venom Usage and Mortality
From 2005 to 2006, ASV was given to 702 (90.0%) of 780 victims. From 2006 to 2007, ASV was given to 651 (77.6%) of 839 victims. The decreased use of ASV from 2006 to 2007 was statistically significant (chi-square test = 45.32, degrees of freedom = 1, P < .001) (Table 1).
Analysis of snakebite victims, anti snake venom (ASV) usage, and mortality
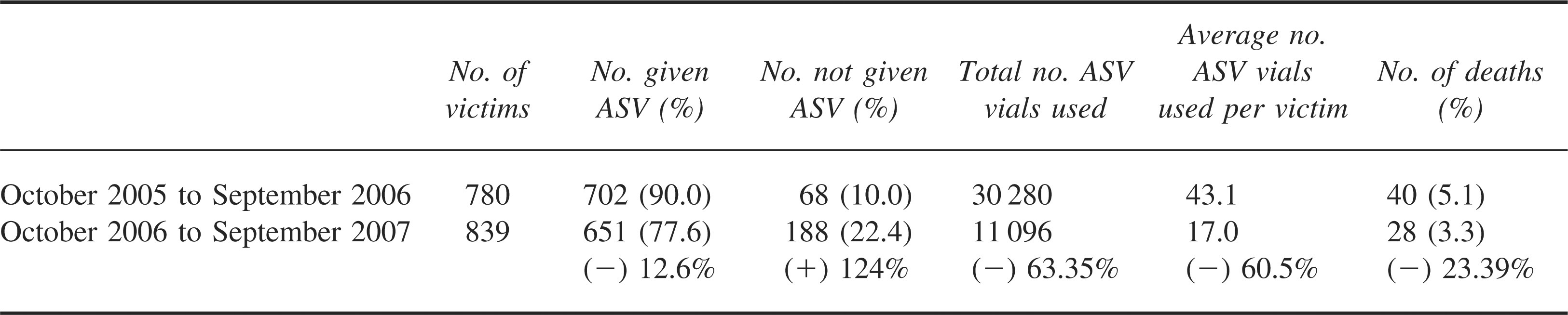
There were 40 deaths related to snakebite from 2005 to 2006 (mortality rate 5.1%) and 28 deaths from 2006 to 2007 (mortality rate 3.3%). The reduction in mortality approached statistical significance (chi-square test = 3.22, degrees of freedom = 1, P = .072) (Table 1).
Mortality Analysis
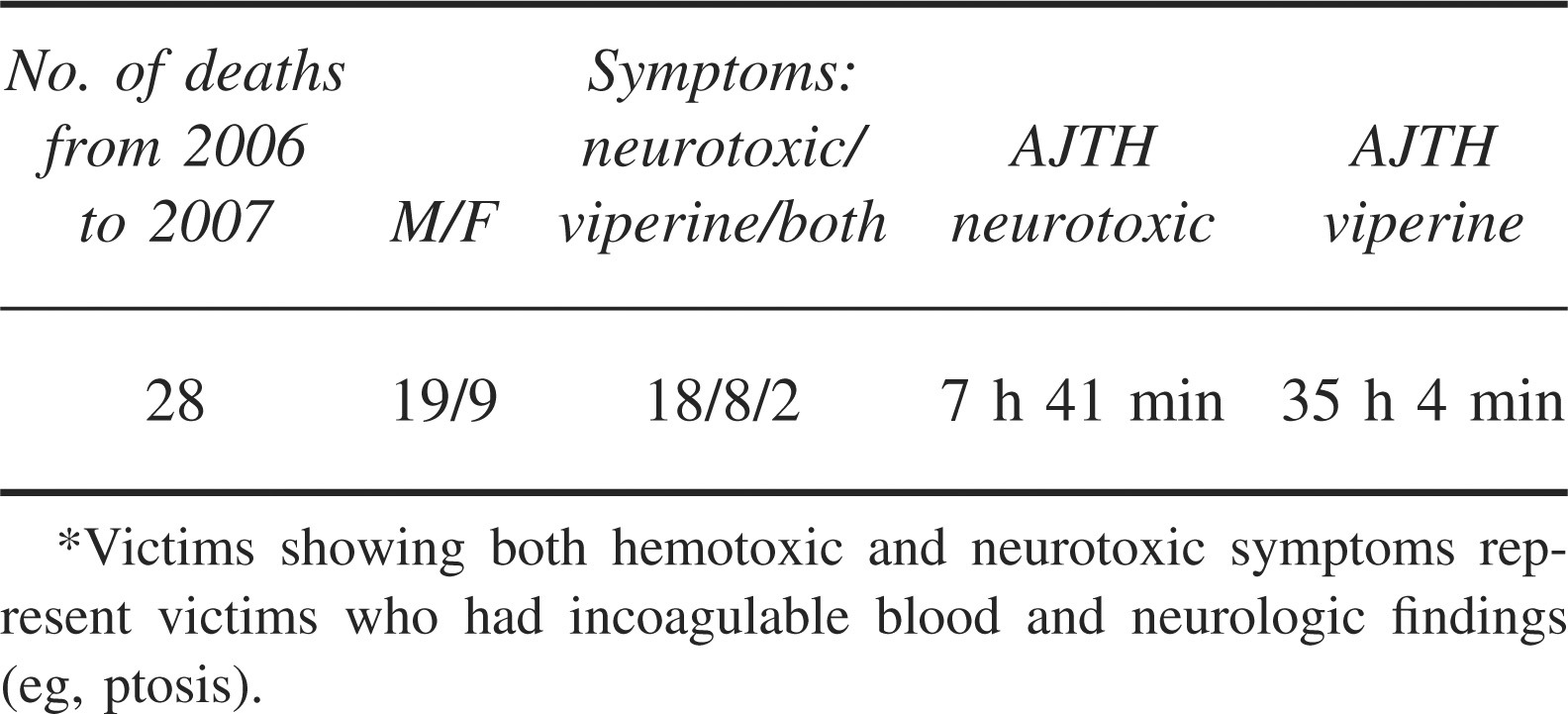
The average journey time to the hospital during the new protocol period was much greater for viperine bite victims compared with neurotoxic bite victims, reflecting the difference in the onset of symptoms and the mode of death, which in viperine bite victims in the study area is usually due to acute renal failure (Table 2). The reliance on traditional healers results in viperine bite victims remaining under such treatment for longer periods due to the slower speed of onset of symptoms compared with neurotoxic victims. The failure of such treatments is more rapidly visible in neurotoxic bites, and the victim is referred to an allopathic hospital.
Analysis of mortality under the new protocol in terms of type of envenomation and average journey time (AJTH) to Midnapore Medical College Hospital (M = male, F = female)*
Of patients who died during the protocol period, only 1 arrived at a medical care facility within 1 hour (Figure 1). Those in the 1- to 4-hour group took 3 hours to reach the hospital, and the remaining patients arrived in excess of 3 hours.
Epidemiology
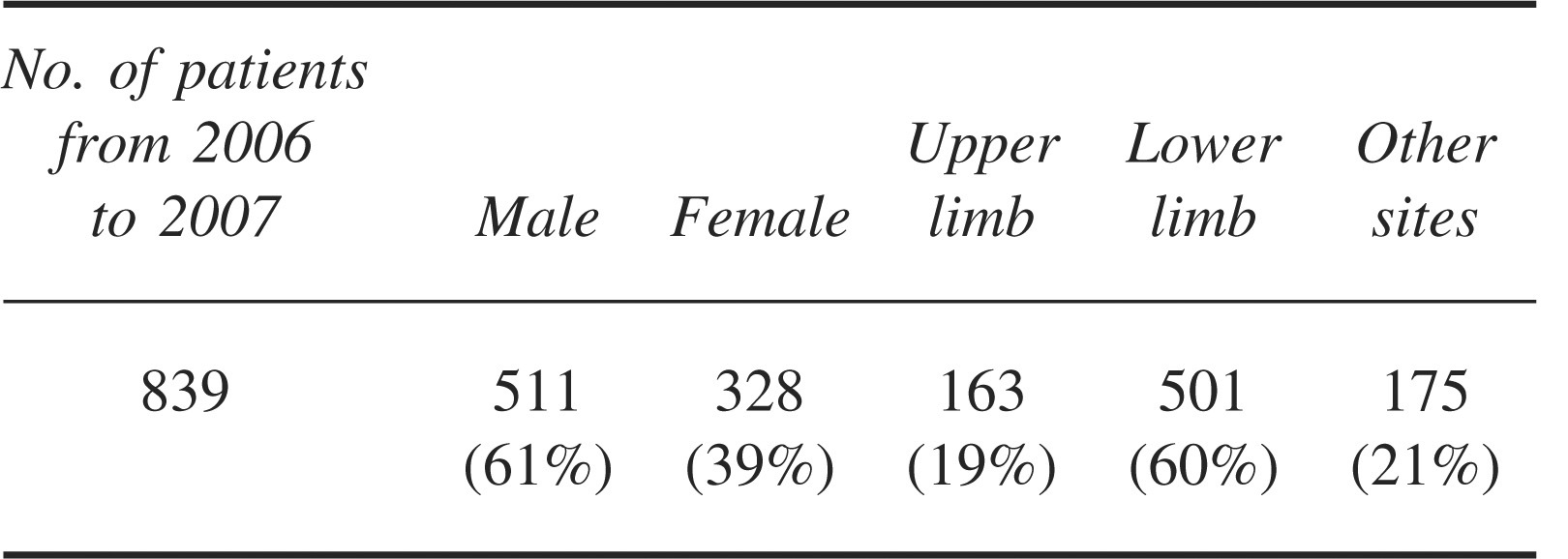
Sex distribution and anatomic bite sites for the protocol period are summarized in Table 3.
Bite profile in terms of sex and bite location
Discussion
Indian medical education is heavily dependent on Western textbooks and indigenous textbooks written by fo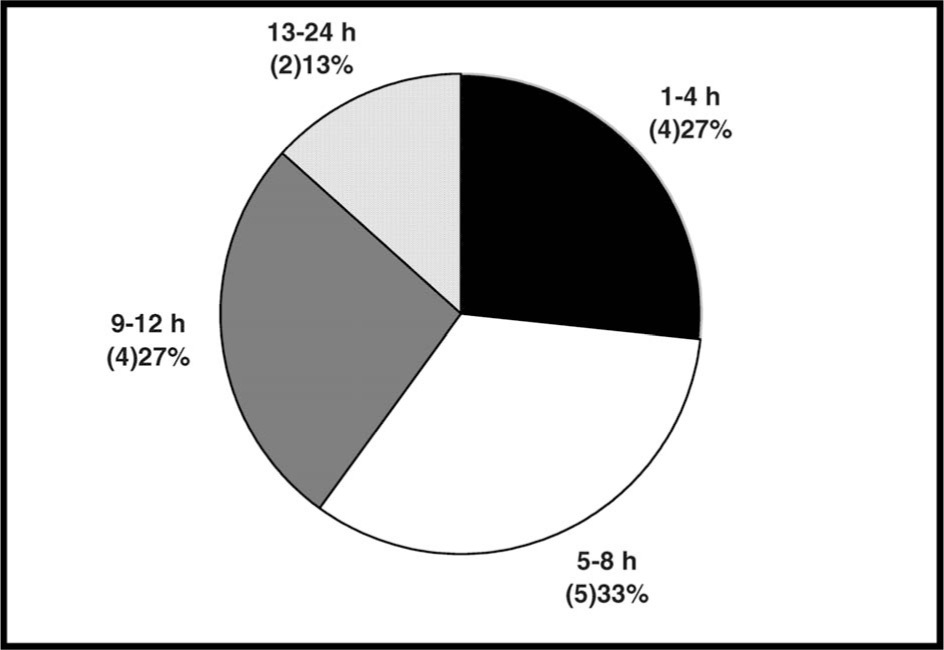
Anti Snake Venom Usage
A lack of availability of sufficient quantities of ASV has been proposed as a key reason for the lack of success in reducing snakebite mortality in the developing world. Worldwide shortages of ASV have been described.5,9,11,27,31–37 Notwithstanding this focus, mortality and morbidity continue to be key concerns.
To use ASV effectively and minimize risk and waste, it is possible to posit 4 vital requirements for which the doctor must have clear guidance
28
: Grounds to determine envenomation Initial dosage Necessity of a repeat dose Endpoints for ASV therapy
Review of the textbooks and articles used by physicians in the region as sources of snakebite treatment guidelines shows that all have serious shortcomings when used in this context, the most serious of which are: Confusing and inapplicable grounds for determining if a patient was actually envenomed
4
–12 Inappropriate or no initial dosage guidelines for ASV4,8,9,18 Unclear criteria for identifying if a repeat dose of ASV is necessary and the timing of assessments of such requirements4,8,10 Lack of clear and unambiguous endpoints for ASV administration4,5,7–10,18
The impact of utilizing a local protocol in this study on ASV usage is both obvious and considerable. The reduction in ASV usage by 19 000 vials in a single district of a developing nation has a huge impact, representing approximately 2% of India's total ASV production. 38 The saving in cost alone amounts to some $150 000 per annum within a resource-constrained state health budget. The benefit of the new protocol on ASV usage is that both risk and wastage are reduced to negligible levels consistent with optimal snakebite management. 28 Anti snake venom is deployed only when there are definitive unambiguous signs of envenoming, doses are empirical, and clear endpoints prevent over usage. The trend toward reduction in mortality suggests that a reduction in risk and reduction of ASV usage are not mutually exclusive. 28
Locally Relevant Protocols
Despite the emphasis on the provision of more and better quality ASV as the primary solution to reducing snakebite mortality, training is nevertheless given some attention in the literature.30,33,39 However, very little attention has been given to the nature of this training and the potential impact on treatment capability.
The reality is that snakebites in many developing countries are managed in a structure very different from Western tertiary hospitals, where many originators of snakebite management recommendations work. For example, in India there are 146 026 subcenter medical facilities, 23 236 primary health care centers, 3346 community health care centers, approximately 1000 district hospitals, and 200 medical college hospitals.40,41 Subcenter medical facilities are often without permanent staff. Primary health care centers usually have 1 doctor and limited hours of operation. Community health care centers have approximately 4 doctors and better facilities and are nominally 24-hour-a-day operations. District hospitals have more doctors but are not usually much better equipped to handle all aspects of snakebite management. For example, very few, even in the more advanced states, have analytical laboratory facilities that can deal with all the required analyses for snakebite management (identifying renal failure or occult bleeding), none are equipped with dialysis machines, and few have mechanical ventilators. Victims of snakebite are referred directly by subcenter medical facilities, primary health care centers, or community health care centers to district hospitals or medical college hospitals with better facilities. The need for dialysis or mechanical ventilation is handled primarily only by medical college hospitals, although interestingly dialysis was not available at Midnapore Medical College during the study. 15
It has been previously reported 3 that virtually all textbooks in use are written from a Western tertiary basis and set of assumptions. 4 –12 Protocols, however, need to be contextually relevant and developed with a sound understanding of local conditions and environments. Essential in these environments are clear and practical guidelines that address the 4 key areas of ASV use, in addition to simple guidelines for managing adverse reactions to ASV; directions for the use of available anti-cholinesterase drugs; guidelines that cover treatment in basic health units with criteria and guidance on when and how to transfer a victim to a better equipped hospital; and simple steps to protect neurotoxic victims with airway risk. Even medical colleges in developing countries, such as Midnapore Medical College, that do have mechanical ventilators may only have 1 or 2 in an intensive care unit setting. At periods of high usage, victims will have to be transferred to other hospitals, and simply recommending the use of a resuscitation bag is inadequate if better methods are available. Previous authors have shown the success of such good local protocols. 30
A further advantage of contextually relevant protocols, developed with cognizance of local conditions, is that snakebite treatment can commence far earlier in medical facilities close to the victim and reduce the need for extensive travel to better equipped hospitals. Primary health care centers and community health care centers are, however, capable of dealing with snakebites only if they have realistic protocols that suit their conditions. Where these have been provided excellent results have been noted.42,43 There are examples of regional protocols produced previously for South East Asia, for which there have been claims of success.9,39 However, the actual relevance of such guidelines developed by nonregional experts is very far from providing a solution. Anti snake venom guidelines are confusing and inconsistent; drugs are recommended that are unavailable in large areas of the regions concerned; ASV dosage recommendations are absent; and there are no adequate guidelines for management in nontertiary hospitals, which constitute 98% of the treating facilities. 9 Doctors in our study and elsewhere have used these guidelines in developing previous approaches to managing snakebites. This has, for example, led to patients receiving ASV simply due to the presence of renal failure, even though coagulation testing showed coagulable blood on their arrival at the hospital. This stems from such guidelines clearly (though erroneously) stating that “acute renal failure” is an indication for ASV. One set of guidelines further states that ASV may “reverse systemic envenoming even when this has persisted for several days” and lists renal failure under systemic symptoms. 9 Examples such as these are confusing, lead to inappropriate levels of ASV being given, and highlight a lack of awareness of the practical implementation of such recommendations.
Training
Due to the previous finding of the effect of snakebite knowledge on doctor confidence, 13 a workshop training structure was determined as providing the best method for training nursing staff and primary and tertiary doctors in the snakebite area. Workshops provide an environment for discussion and understanding among doctors and support staff who work in the same area and are part of the referral network for victims requiring treatment in a better equipped center. Such workshops facilitate understanding of the role of each part of the health system responsible for snakebite management, from the doctor in the initial medical center, who is to administer the initial dose of ASV to envenomed patients, up through the referral center, where advanced techniques (eg, mechanical ventilation) are provided. Often a doctor is not available when the victim arrives, and nursing staff will make the initial interventions. Workshops also allow distribution of locally developed posters covering guidelines for snake identification, first aid, and treatment. These can be displayed by the bedside and thus provide a convenient reference for care providers. Care providers who attended the workshops prior to this study reported significantly increased confidence in all aspects of snakebite management, particularly in areas of known concern, such as dealing with adverse reactions to ASV. 13 In addition, confidence in the use of the new protocol, with rational time frames for ASV usage, led to the clinical observation that patient time in hospital was reduced from approximately 5 days to 2 days.
It is essential that protocols and training be developed in a relevant, contextual way and particularly related to the local conditions. It is interesting that one of the very few training courses that purport to deal with international toxicology and snakebite, “international” defined in this case as being outside Australia, has not a single member of the faculty from the developing world. 44 The separation of recommendations from the context in which they will be used underpins such approaches and is misguided. It is not surprising, therefore, that the mismatch between the Western approach to snakebites and the reality of the problem in the developing world are so far removed. In the textbook accompanying this course, the guidelines for ASV administration in the region contradict the regional guidelines.9,16 Understandably, doctors are therefore unclear about when ASV should be administered.
The same drawbacks can be seen in the “syndromic approach” proposed by developed world experts for use in developing world locations.9,12 They are underpinned by many false assumptions, such as marked local swelling serving as a definitive sign of viperine envenomation.9,12 In addition, locally medically significant species, such as the saw-scaled viper (Echis carinatus) and hump-nosed pitviper (Hypnale hypnale), are not included, and therefore misdiagnosis is a real possibility. Furthermore, doctors in busy district and primary care hospitals simply do not have time to refer to or interpret complex syndromic flowcharts.9,12,45
Training is needed to disseminate local protocols. This should commence with medical curricula mirroring the local protocols. 46 Such a change was recently made in Pakistan, ensuring that future health officials and doctors are aware of local treatment methods and basic drug and equipment profiles for use in snakebite management in basic health settings. Governments need to be engaged by health institutions, such as the World Health Organization, and snakebite experts and made aware of the shortfall in current medical education.
Epidemiology of Snakebite in the Study Area
The finding of 28 deaths during the protocol period translates to an estimated mortality rate of 0.3 deaths per 100 000 population, which is significantly different from previous findings based on surveys in West Bengal and widely used in epidemiology reports.1,47 Although there are undoubtedly some number of mortally wounded victims who do not report to medical care and are thus not reported as fatalities, this figure would need to be 55 times the number who do report to generate the previous average of 16.4/100 000. 1
The delay in presentation of some victims in our study is related to the use of traditional medical systems, known as “Ozhas” in West Bengal. These “healers” have often been considered the only locally available alternative because primary health centers and community health centers previously did not treat snakebite. The use of local protocols and training of doctors in these facilities ensures that a credible allopathic alternative is locally available and encourages victims to seek such treatment first. Patient mortality was thus virtually eliminated in patients who presented to the hospital early. Neurotoxic envenomings account for the most significant percentage of mortality due to the rapidity of onset of the symptoms and the likelihood of respiratory failure during the journey.
Of all bites in the study area, 40% occurred on the upper limb or other parts of the body excluding the lower limb (Table 3). The site of the bite varies considerably depending on agricultural profile, snake species, and activity. Some authors have reported percentages of bites to other than the lower limbs of 23%, 47%, 52%, 20%, and 38%.1,19,48–50 The finding that 20% of bites occur on other than the upper or lower limbs represents bites incurred mainly while sleeping. The time of the actual bite also varies considerably. Some authors have reported key bite periods of 6
Analysis of bite time and nature of bite*

The variety of bite-related data clearly indicates the futility in attempting to generalize data from single locations, such as “In India, 75% of all snakebites occur below the knee,” to all of India and similar environments.51,52
The percentage of male vs female bites also varies considerably. In this study, 61% vs 39% was reported, whereas others have reported 55% vs 45%, 68% vs 32%, and 53% vs 47%.1,19,49
What is important is that doctors in areas with a high incidence of snakebites record circumstances of bites in patients reporting to the hospital, analyze the profile, and provide guidance to the local community as to the key risk activities in their particular area.
It is interesting to note that 2 victims in our study exhibited incoagulable blood, measured by the 20-minute whole blood clotting test, in a new, clean, dry, glass tube and visible neurotoxic signs (eg, ptosis). The most likely species responsible is the D russelii, which has been reported as causing both antihemostatic and neurological findings in Sri Lanka and south India. Clearly, the area for which this species can exhibit these mixed venom effects is larger than previously reported.11,53
The limitations of this study include the reliance on historical controls for comparison with the protocol-derived data. Ideally, both sets of data would have been gathered prospectively, but the introduction of the new protocol made that impossible. There are certainly potential drawbacks in comparing prospective and retrospective data (eg, overall levels of envenomation or general population health could be slightly different for each period). To minimize this effect, 2 periods of similar length of 1 year were selected to ensure that the seasonality factor was encompassed. However, we believe the number of victims was sufficiently large, particularly in the prospective phase, to render any such effect minimal. Further larger studies could also be undertaken to refine the statistical significance of the reduction in mortality.
Conclusions
Although training of doctors in snakebite management has been referred to in the literature, this study shows for the first time that nationally developed protocols implemented locally that include training and management techniques can significantly improve outcomes in terms of significant reductions in overall ASV utilization through reduced waste and show a trend towards decreased mortality. These findings have implications for policy makers and planners in the provision of both training and supplies of ASV. It is recommended that effective ASV usage protocols be developed and made a key priority of health administrators and organizations, such as the World Health Organization. It is further recommended that efforts to produce more ASV be made only when reliable forecasts including effective ASV usage are available.
Footnotes
Acknowledgment
The authors acknowledge the support and encouragement provided by the Honorable Health Minister of the Government of West Bengal, Dr Surjya Kanta Mishra.