
Abstract
Objective
To document the prevalence of hypothermia in a mass participation endurance open water swimming event and to determine demographic and individual factors that may predict failure to finish the race and hypothermia.
Methods
A prospective observational study in competitors in a 19.2-km open water swimming race in Perth, Western Australia. Pre-race information collected included age, sex, training and race experience, medical history, and body mass index (BMI). Body temperatures at 5 minutes postrace were measured using an equilibrated oral- or rectal-reading low-range glass mercury thermometer. Logistic regression was used to develop models predicting hypothermia (defined as a temperature of <35°C) and failure to finish the race.
Results
One hundred and nine competitors (70 male, 39 female) with a combined mean age of 38.4 ± 12.1 years were studied. Hypothermia was the most common race-related illness, identified in 26 of 35 swimmers screened as requiring temperature measurement, including 5 who required short-stay hospital care and 2 who required critical care transfer. Longer race duration (odds ratio [OR] 1.77, 95% CI 1.10–2.84, P = .018) was associated with an increased risk of hypothermia, and higher BMI (OR 0.57, 95% CI 0.41–0.79, P = .001) was associated with a decreased risk of hypothermia. Weak predictors of failure to finish were age (OR 1.06, 95% CI 1.01–1.11, P = .012) and hours spent training (OR 1.08, 95% CI 1.01–1.16, P = .025).
Conclusions
Hypothermia is a common condition affecting mass participation long-distance open water swimmers. Increased BMI appears to be protective against hypothermia, while prolonged duration of the swim predicts an increased risk of hypothermia. The weak predictors of failing to finish are of questionable clinical significance.
Keywords
Introduction
Hypothermia is a recognized medical risk of long-distance open water swimming.1,2 Open water swimming has become increasingly popular worldwide, as represented by its inclusion, for the first time, in the 2008 Beijing Olympics. For race medical organizers this presents challenges in preventing, detecting, and treating illness in race competitors both at elite and mass participation levels. We set out to document the prevalence of hypothermia suffered by solo participants in the Rottnest Channel Swim, one of the world's largest mass participation open water swims, held annually off the coast of Perth, Western Australia. We also prospectively collected demographic data on these participants to identify factors that might predict hypothermia and failure to finish the race.
Setting
The Rottnest Channel Swim takes place over 19.2 km of open water off the west coast of Western Australia, from Cottesloe Beach in Perth to Rottnest Island in the Indian Ocean to the west. Up to 700 swimmers plus their support craft are in the water at any given time. In total there are around 2500 swimmers in teams of 2 and 4 competitors, plus approximately 150 to 180 solo swimmers. Solo competitors complete the event without a swimming break and must race under Federation Internationale de Natation Amateur open water rules. 3 These rules do not allow any flotation devices (including wetsuits). Head protection consists of only a thin latex bathing cap. Competitors commonly smear themselves in animal fats for some degree of insulation, as in other cold-water swimming events.
Methods
This was a prospective observational study conducted at the 2006 Rottnest Channel Swim. It was limited to solo entrants and had the prior approval of the Sir Charles Gairdner Hospital ethics committee.
Prior to the race, a questionnaire was forwarded to all solo entrants requesting information about their weight and height (to allow calculation of body mass index [BMI]), age, past medical history, training history, and previous open water swimming experience. Return of the completed questionnaire was considered indicative of consent to participate in the study.
As part of standard race medical care all solo finishers underwent a brief screening assessment within 1 minute of emerging from the water at the race's end. This assessment was done in the race finishing chute. With the number of finishers at any one time it was necessarily brief. It was conducted by physicians who sought clinical signs of hypothermia, which was considered likely to be the major medical risk of the event. The 4 parameters assessed were gait, presence/absence of shivering, demeanor, and mentation. General examination for other significant illness was also conducted. All swimmers felt to be at risk on the basis of this medical assessment were moved to the race medical tent for more thorough evaluation and treatment, as required. All swimmers assessed in the medical tent had an initial oral temperature measured at approximately 5 minutes post finish using a low-reading glass thermometer placed in the deep sublingual pocket until reading equilibrium occurred (typically 3 minutes). Further readings were taken at the discretion of the attending physician during the swimmer's stay in the medical tent. Participants had rectal temperatures recorded only at the discretion of the attending physician. Details of their diagnosis on discharge and disposition were recorded. Hypothermia was defined as an oral or rectal temperature of <35°C in those swimmers identified as “at risk” based on the brief screening assessment.
Statistical Analysis
Frequency counts and proportions were calculated for categorical data, with differences being assessed using the χ2 test. For continuous data, means, along with their corresponding SDs, were derived and differences determined using the t test. Logistic regression was used to identify predictors for hypothermia and failure to finish, with univariate analysis and clinical reasoning being used to identify those predictor variables considered appropriate for inclusion in the model. The model was also tested for interaction. Odds ratios (ORs) along with their corresponding 95% CIs were reported for the model. Statistical significance was accepted at P < .05.
Results
A total of 172 solo registrants entered the 2006 Rottnest Channel Swim, of which 63 (36.6%) did not return the questionnaire prior to the event and thus were excluded from any further analysis. Baseline characteristics for the remaining total of 109 male and female participants are outlined in Table 1.
Baseline characteristics of participants
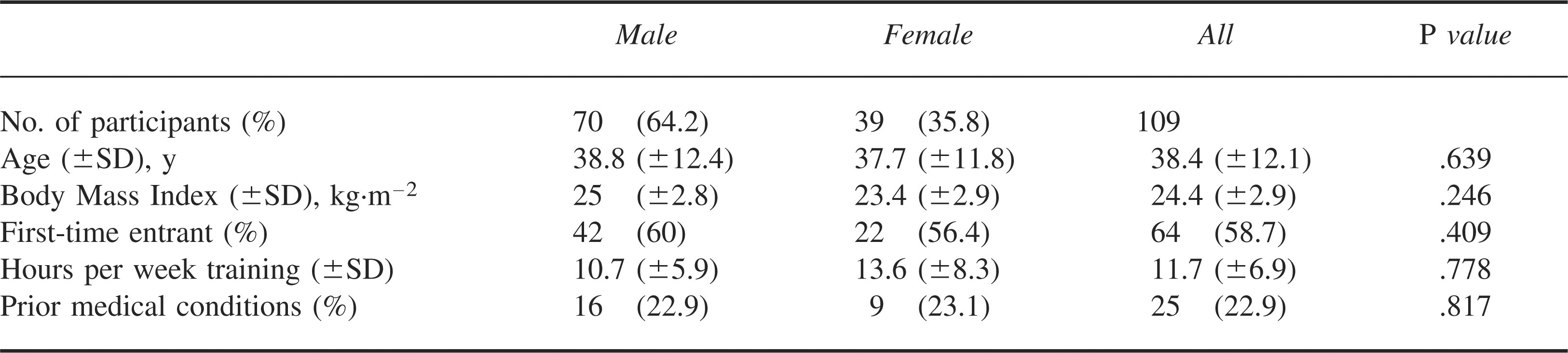
The self-reported prior medical conditions included asthma in 21 participants, ischemic heart disease in 4 participants, and thyroid disease (unspecified) in 3 participants. The mean race time was 7.9 (±1.6) hours and was similar for both males and females. In the 109 participants enrolled into the study, 10 (9.2%) did not start, 21 (19.3%) did not finish, and 3 (2.8%) were disqualified.
Conditions for the race during the study included a water temperature that varied from 19°C to 22°C and an air temperature that ranged between 17°C at the start and 22°C by the time the bulk of the field finished. Wind speeds (predominantly headwinds) ranged from 20 to 35 knots, and swell was up to 3 m. Time in the water varied from approximately 5 hours for the leaders to 12 hours in the last finishers.
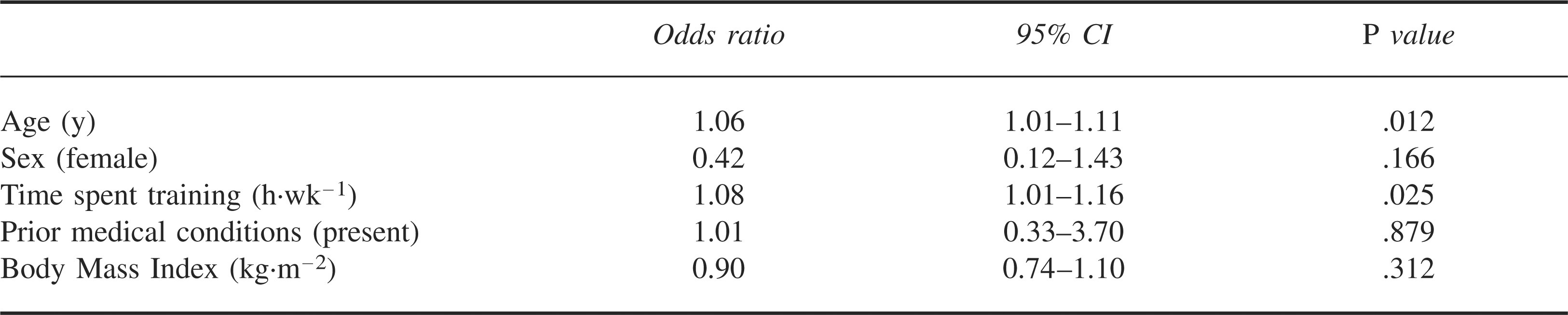
Logistic regression revealed that increasing age and increased time spent training were weak but significant predictors of not completing the race (Table 2).
Logistic regression for predictors of not completing the race
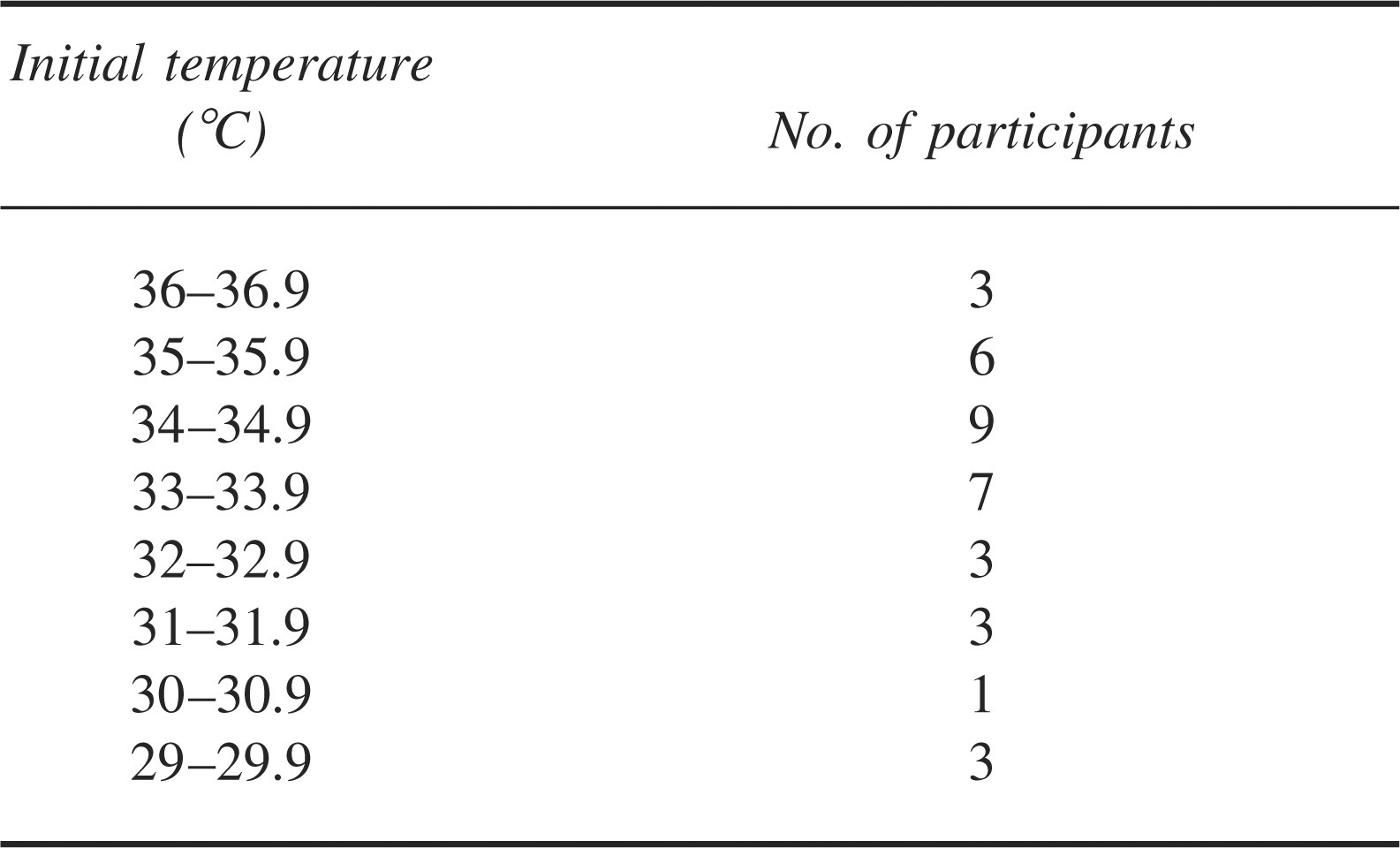
There were 35 race participants who were determined to be at risk on the basis of the clinical screen and had either oral (n = 31) or rectal (n = 2) or both (n = 2) temperatures taken at the completion of the race or following withdrawal from the race. Hypothermia was identified in 26 (18 males and 8 females) of the 35 who had temperatures measured. These 26 cases represent 22.9% of the 109 study participants overall. No temperatures were recorded for those who were clinically assessed but not considered to require further treatment or investigation. The temperature ranges recorded are shown in Table 3. Two swimmers had only rectal temperatures that were only measured because of altered mental state (30.0°C and 29.4°C, respectively). Two swimmers had both oral and rectal temperatures measured, and the oral value was used for consistency. In one of these swimmers the oral temperature was 29.5°C and the rectal temperature was 31.0°C. In the other the oral temperature was 29.6°C and the rectal temperature 33.8°C.
Temperatures measured at 5 minutes postrace
Short-stay medical care at the island nursing post for rewarming was required for 5 patients. A further 2 patients required transfer for mainland intensive care unit management. One suffered hypothermia, atrial fibrillation, and immersion syndrome. The other suffered an asystolic, hypothermic cardiac arrest with a documented 40-minute period of pulselessness that finally responded to advanced life support. Both made full functional recoveries. All other patients were managed in the race medical tent.
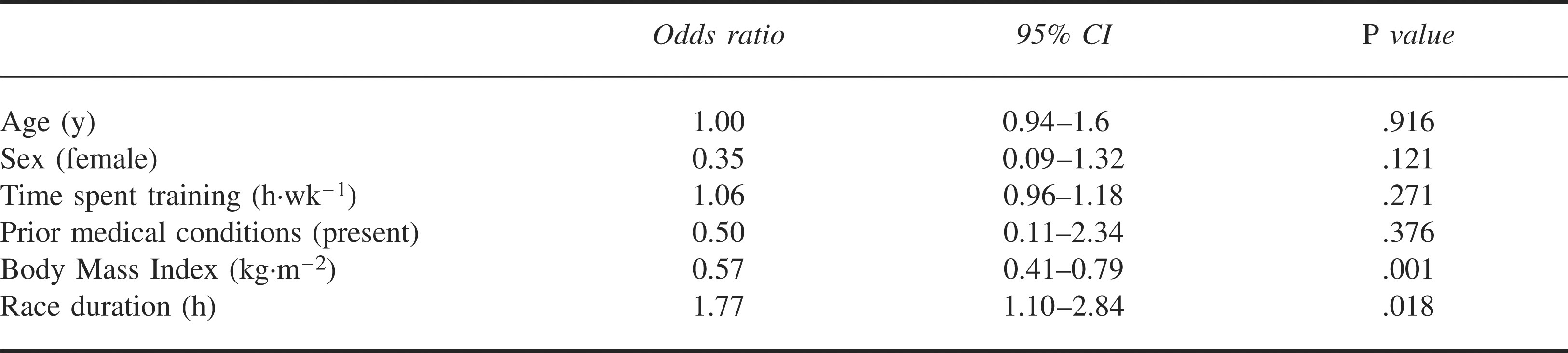
Logistic regression was used to identify predictors of hypothermia. The predictor variables of age (years), sex (male/female), race duration (hours), time spent training (h·wk−1), BMI (kg·m−2), and previous medical conditions (yes/no) were entered into the model. Body mass index (OR 0.57; P = .001) and race duration (OR 1.77; P = .018) were the only predictors to reach statistical significance. An elevated BMI was identified to be protective against hypothermia, in that for each whole-unit increase in BMI, the likelihood of hypothermia was reduced by 43%. Conversely, for every hour that the race participant was in the water during the race the odds of hypothermia increased by 77%. These data are summarized in Table 4.
Logistic regression for predictors of hypothermia
Discussion
The major, though not unexpected, finding of our study is that hypothermia is common in open water swimming and is more frequent with increasing race time and less frequent with increasing BMI. To date this is the largest study of hypothermia in open water swimming, with previous studies involving case reports, 4 shorter swims, smaller cohorts, 1 or controlled environments. 5 We enrolled nearly two thirds of all the event solo entrants in our study and have no reason to believe that our volunteers are not representative of competitors as a whole.
We defined hypothermia as an oral or rectal temperature of less than 35°C in those identified as being at risk based on our screening assessment. Our use of oral readings as a measurement standard can be challenged and may call into question our diagnosis of hypothermia. Low oral temperatures occurring independent of significant compromise are of relatively low value. Such concerns are highlighted by our 2 cases in which paired rectal and oral temperatures were recorded. Although the correct diagnosis (hypothermia, by our definition) was made in both cases, the actual numerical differences are substantial. This is important in establishing the magnitude of hypothermia experienced in the race. It is not necessarily as important in establishing incidence or guiding management, both of which are directed by clinical assessment as much as by the absolute measured temperature. That hypothermia is a real and apparent clinical risk in this event is demonstrated by the more serious cases we noted, including, at the extreme, the case of an asystolic hypothermic cardiac arrest.
We considered research methodologies that used alternative methods of temperature measurement, such as routine rectal readings. The privacy issues created by a public beachfront environment and our aim to study a large cohort of swimmers over a short time in a real race setting made alternatives impractical. Initially we had planned to also use tympanic thermometers, but these substantially overestimated the severity and prevalence of hypothermia, as we have reported previously. 6 Although not part of our study protocol, we noted that the oral temperatures we recorded seemed to correlate well with both our volunteers’ clinical presentation (such as absence of initial shivering at temperatures below 33°C) and clinical course, with observed rewarming rates of 1°C to 3°C per hour once shivering developed.
There remains some debate regarding the most accurate site for measurement of representative core temperature. 7 Balancing practicality and optimum core temperature measurement, a logical future research approach in this area would be the use of ingestible temperature-measuring capsules (eg, CorTemp Ingestible Core Body Thermometer Pill, HQInc, Palmetto, FL) to collect more accurate core temperature readings. Such commercially available devices require each competitor to either wear a data logger (which may be difficult to provide for a large field of entrants) or to swim within 1 m of the logger, which presents real difficulties in the open ocean. Nevertheless, such measurements within the abdominal cavity are much more likely to approximate the true core temperature at rectal or esophageal sites.
We recognize that a weakness of our study is that we only measured temperatures in those swimmers who were considered to be at risk on the basis of the physician finish line screening assessment. It is quite possible that the true prevalence of hypothermia in the race was substantially higher than our data demonstrate, representing a group of clinically asymptomatic finishers. That 26 of 35 finishers who our clinical screen assessed as being at risk of hypothermia subsequently proved to be so using our temperature measures indicates that either our clinical screen was effective or that almost all finishers are indeed hypothermic. Further studies looking at both those deemed worthy of further assessment on the clinical screen and those regarded as asymptomatic, potentially even all starters, would help clarify this question. In addition, those who did not finish were not routinely screened. As the only group of health care providers on this isolated island that day, in regular contact with all emergency services, we can be certain that no unrecognized hypothermics presented to other health care providers, and so no serious cases of hypothermia were missed. However, it is likely that we did miss cases of mild hypothermia that would be likely to be able to be self treated in this otherwise-healthy population. There is also a possibility that we have overestimated the prevalence of hypothermia as a result of our use of oral temperatures as our standard, as discussed above.
Our results demonstrate that increased BMI appears to be significantly protective against hypothermia in the context of open water swimming. This confirms what one would intuitively expect and has been suggested in previous work in different circumstances.8,9 Notably, although they did not demonstrate a higher prevalence of hypothermia, Keatinge et al 2 found that “swimmers with less subcutaneous fat terminated their swims after significantly less time in the water than those with thicker skinfold differences.” We did not use skinfold thickness measurements in our pre-race assessments, which may have provided a more accurate assessment of insulation. Similarly, the correlation between increasing race time and hypothermia is again intuitive and has been described before. 10
The finding of increasing age and increased time spent training as predictors for not completing the race were weak ones and were of doubtful clinical significance. Such a finding is counterintuitive and may reflect the idiosyncrasies of the much smaller cohort (21 swimmers) of nonfinishers compared with the larger group of finishers (75 swimmers). Again, in-race assessment of the core temperatures of swimmers may help to delineate whether hypothermia is a frequent problem in nonfinishers.
Every open water swimming race is different in terms of length, swell, current, wind, and water temperature. We cannot be certain that our results can be generalized to other events. Nevertheless, we believe that the 2 most important issues for organizers and medical support staff to consider are race length and insulation. Races should have sensible cut-off times that are matched to the ambient conditions and the likely time of onset of hypothermia. Serious consideration should be given by Federation Internationale de Natation Amateur to a rule change to allow the wearing of wetsuits, despite the buoyancy they may provide. Precedents for this already exist in competitive triathlons, and if all competitors are allowed to wear wetsuits, it merely shifts the competitive factors rather than giving some participants an unfair advantage. Hypothermia appears to be frequent in open water swimming and if allowed to progress may be life threatening.
Footnotes
1
The authors have no competing interests to declare.