
Abstract
North American rattlesnakes possess venom with primarily cytotoxic and hemotoxic properties. When persons are envenomated by these snakes, thrombocytopenia and coagulopathy commonly occur, yet patients rarely develop severe bleeding. This report describes a 44-year-old Native American man bitten on the index finger by an unknown species of rattlesnake. The man developed massive gastrointestinal hemorrhage that was ultimately treated with recombinant factor VIIa. He presented to an emergency department with a depressed level of consciousness, a blood pressure of 60/20 mm Hg, and heart rate of 148 beats per minute. He was diaphoretic and vomiting bright red blood. Initial laboratory results revealed thrombocytopenia and coagulopathy. Despite aggressive fluid resuscitation and administration of blood and antivenom in the emergency department, the patient continued to have profuse upper gastrointestinal bleeding, with hemoglobin as low as 1.8 g/dL. He received fluids, antivenom, and multiple blood products, with cessation of bleeding after administration of recombinant factor VIIa. Esophagogastroduodenoscopy revealed a single Mallory-Weiss tear as the source of hemorrhage. The patient stabilized after 6 hours of aggressive resuscitation but over the next several days developed several complications, including acute renal failure and gram-negative sepsis. The patient died on hospital day 5. In cases of life-threatening hemorrhage after rattlesnake envenomation in which traditional therapy with antivenom and aggressive supportive measures fail, recombinant factor VIIa should be considered as an additional therapeutic option to achieve hemostasis.
Introduction
North American rattlesnakes possess venom with primarily cytotoxic and hemotoxic properties. When persons are envenomated by these snakes, thrombocytopenia and/or coagulopathy commonly occur and are frequently associated with oozing of serosanguineous fluid from puncture wounds at the bite site. Extreme drops in both platelets and fibrinogen may occur. Yet even under these circumstances patients rarely develop severe bleeding.1,2,3 The following report describes a patient with massive gastrointestinal hemorrhage after a bite to the index finger by an unknown species of rattlesnake. Resolution of bleeding was temporally associated with administration of recombinant factor VIIa.
Case report
A 44-year-old Native American man was bitten on the right index finger by a rattlesnake while cleaning a chicken coop. His past medical history included alcohol-related liver disease, anemia, and thrombocytopenia, with a reported platelet count of 46 K/mm3 1 month earlier. He presented within 15 minutes to a rural emergency department with a depressed level of consciousness, a blood pressure of 60/20 mm Hg, and heart rate of 148 bpm. He was diaphoretic and vomiting bright red blood. A puncture wound was present on the right index finger, and there was mild swelling of the hand.
He was initially treated with solumedrol 80 mg intravenously and 0.5 mg subcutaneous epinephrine, due to concern that he was having an anaphylactoid reaction to the venom. Two liters of normal saline were infused intravenously, which resulted in a transient improvement in systolic blood pressure to 106 mm Hg. A nasogastric tube was placed with output of 1 L of blood over the next 90 minutes. Initial laboratory studies revealed hemoglobin 13.1 g/dL, hematocrit 37.6%, platelets 10 K/mm3, prothrombin time 56 seconds, and fibrin split products <5 μg/mL. There were no red blood cell fragments noted on peripheral smear. Fibrinogen level was not available.
Persistent hypotension developed, and he was administered normal saline, dopamine, and blood products. A total of 3 L of intravenous fluids, 2 units of packed red blood cells, 1 unit of fresh frozen plasma, and 4 vials of Crotalidae polyvalent immune Fab rattlesnake antivenom were administered in the emergency department. The hospital did not have additional antivenom or the capacity to manage this unstable patient. The patient was then transferred by fixed-wing aircraft to our toxicology center. At the time of transfer he was awake but drowsy. During transfer, the patient lost another 2 L of blood through the nasogastric tube. A norepinephrine infusion had been added, and an additional 2 L of intravenous fluids was given. Prochlorperazine 10 mg had been given intravenously for vomiting and diazepam, 10 mg was given intravenously for agitation.
The patient arrived at our intensive care unit approximately 5 hours after the bite occurred. His blood pressure was 87/44 mm Hg, heart rate 133 bpm, respiratory rate 21 bpm, and core temperature 91°F. Ventilatory effort was poor, and pulse oximetry was 94% on an oxygen nonrebreather facemask. The patient was comatose and without purposeful movement, and there was continued profuse loss of bright red blood via his nasogastric tube. Heart sounds were normal and lungs were clear to auscultation. Swelling of the hand was moderate and had progressed to involve the forearm. The right arm was ecchymotic with soft compartments, and a small hemorrhagic bleb was forming on the finger at the site of fang entry. There was some blood oozing from other puncture sites on the extremities. There was no evidence of tissue infarction on the skin or extremities. A Foley catheter was placed without return of urine.
The patient was orotracheally intubated after administration of vecuronium and midazolam intravenously. Simultaneous treatment with packed red blood cells and fresh frozen plasma, antivenom, sodium bicarbonate boluses, intravenous fluids, vasopressors (including epinephrine, norepinephrine, and dopamine), and thiamine was instituted immediately. A detailed account of blood products, fluid boluses, and antivenom administration over the first 30 hours is presented in the Table. Octreotide 50 mcg was given intravenously. Arterial blood gases showed pH 6.85, pCO2 62 mm Hg, pO2 272 mm Hg, bicarbonate 10 mEq/L, and base deficit 21 mEq/L on FIO2 1.0. Other laboratory values on arrival to the intensive care unit included hemoglobin 3.9 g/dL, platelets 7 K/mm3, prothrombin time 46.7 seconds, partial thromboplastin time >150 seconds, fibrinogen 35 mg/dL, sodium 145 mmol/L, potassium 4.2 mmol/L, blood urea nitrogen 4 mg/dL, creatinine 1.1 mg/dL, lactic acid 21 meq/L, creatinine kinase 66 U/L, ammonia 160 μmol/L, and ethanol 104 mg/dL. Initial studies included a chest radiograph that was negative for effusions or infiltrates. Electrocardiogram was significant for a sinus tachycardia at a rate of 134 bpm, inferior Q waves, QRS 92 msec, and QTc 460 ms. An echocardiogram was negative for cardiac tamponade, pericardial effusion, or thrombus and showed normal contractility with an ejection fraction of 65%.
Patient details
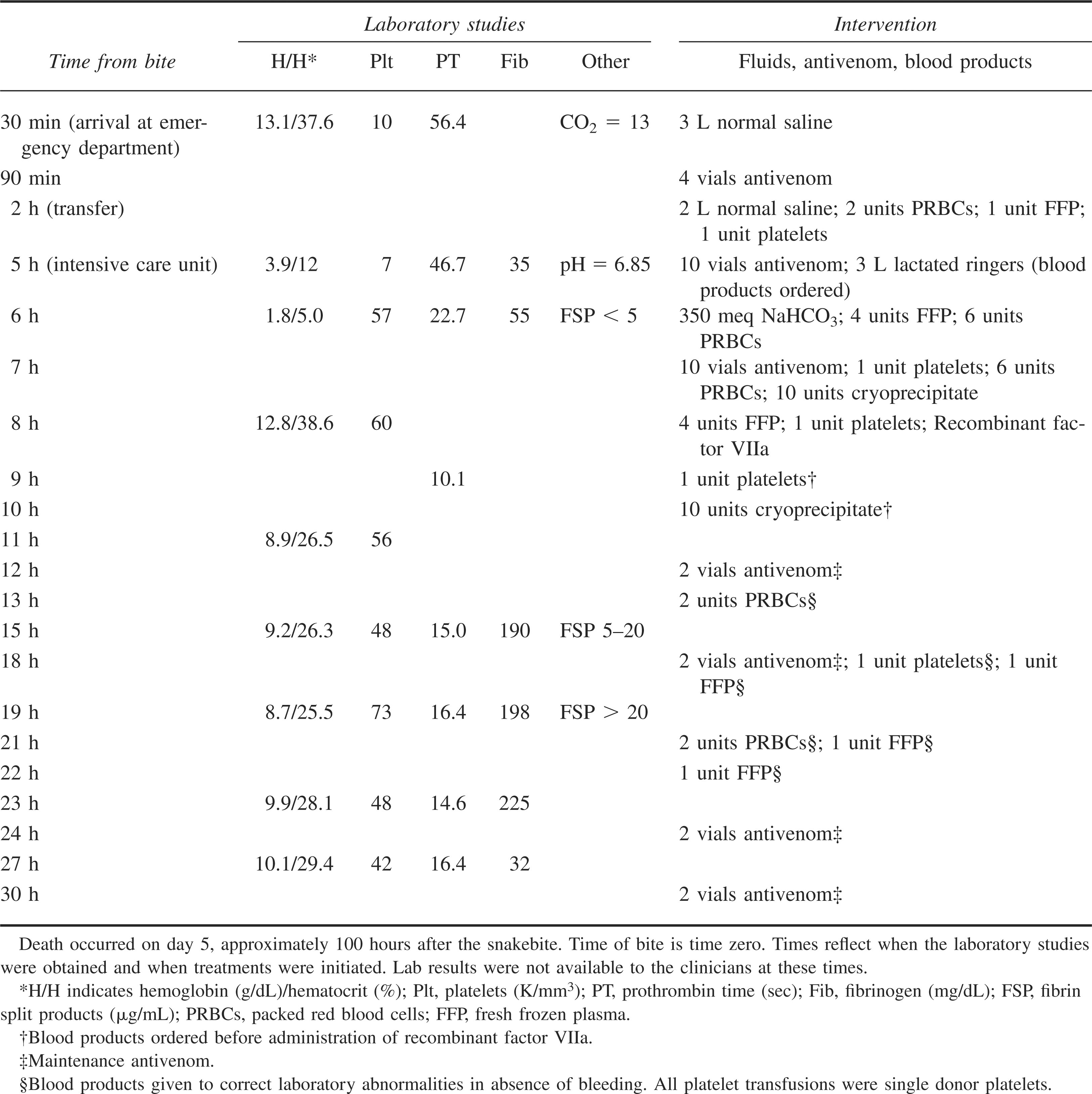
Within 1 hour of arrival, the patient had lost an additional 6 L of blood through his nasogastric tube. Repeat laboratory studies at this time revealed Hg of 1.8 g/dL and hematocrit of 5%. Platelets had risen to 57 K/mm3. Three more liters of blood were lost over the next two hours. Over the first 4 hours of intensive care unit resuscitation, the patient received 5 L of intravenous fluids, 350 meq of intravenous sodium bicarbonate, 20 vials of Crotalidae polyvalent immune Fab rattlesnake antivenom, 12 units of packed red blood cells, 8 units of fresh frozen plasma, 2 units of platelets, and 10 units of cryoprecipitate (Table).
Because severe hemorrhage continued from the upper gastrointestinal tract despite the above therapy, the patient was treated with 7.2 mg recombinant factor VIIa intravenously, after which bleeding ceased almost immediately. He then stabilized with a heart rate of 60 bpm, systolic blood pressure of 110 mm Hg off vasopressors, and hemoglobin oxygen saturation of 99% on 1.0 F
Computed tomography scan of the brain was obtained and was negative for the presence of blood but positive for fluid in the sinuses. Esophagogastroduodenoscopy revealed a Mallory-Weiss tear responsible for the bleeding and was negative for esophageal varices, which had originally been suspected to be present.
In the first 36 hours after initial stabilization and cessation of hemorrhage, there was no further bleeding noted, but the coagulopathy and thrombocytopenia persisted. It was unclear if these were due to venom, the large volume resuscitation and acidosis the patient had experienced, or both. Additional blood products were given in an attempt to completely reverse coagulopathy and keep hemoglobin higher than 10 g/dL. Maintenance doses of antivenom were given every 6 hours beyond the usual 3 doses recommended by the manufacturer, in order to maintain elevated antivenom levels and prevent recurrent venom-induced coagulopathy and thrombocytopenia.
Although the patient did not exhibit further hemorrhage, a groin hematoma was noted at the site of a central venous catheter placement on hospital day 2. A computed tomographic scan of the abdomen and pelvis was obtained to look for retroperitoneal hemorrhage, and this was negative. Early on hospital day 3, a transient episode of epistaxis occurred, along with passage of a single melenotic stool. This was treated by housestaff with placement of anterior nasal packs and administration of packed red cells, platelets, fresh frozen plasma, and an additional dose of recombinant factor VIIa. Repeat laboratory testing at this time revealed hemoglobin 11.2 g/ dL, platelets 47 K/mm3, prothrombin time 13.8 seconds, and fibrinogen 276 mg/dL. Instructions not to administer further blood products were given at this time.
Over the next 2 days, the patient developed acute respiratory distress syndrome, acute renal failure, lactic acidosis, and abdominal compartment syndrome. Sepsis was suspected, and antibiotics were initiated. Family members did not wish for additional aggressive measures to be taken, and the patient died on day 5 after care was withdrawn. Blood cultures ultimately revealed Escherichia coli, presumably originating from ischemic bowel.
Discussion
Hematologic abnormalities, including thrombocytopenia and coagulopathy, are well-known effects of rattlesnake envenomation. 1 –4 Rattlesnake venom includes a variety of hemotoxic components, including thrombin-like enzymes, phospholipases, and serine proteases. Thrombin-like enzymes incompletely cleave fibrinogen, leading to the formation of an unstable fibrin clot. Because the fibrin formed is not cross-linked and is easily degraded, intravascular clotting does not occur.2,3,5 Even severe derangements in fibrinogen or prothrombin time after envenomation rarely result in significant bleeding. 1 –3
Mechanisms for development of thrombocytopenia are not well elucidated but appear to involve various venom components, including phospholipases that may damage platelet membranes. The exact effects of venom on platelets may be species dependent and also involve interaction with other venom components. 5 Venom-induced thrombocytopenia is not typically associated with bleeding. 1 –3
Coagulopathy and thrombocytopenia due to rattlesnake envenomation are best managed with antivenom. Only in the setting of active bleeding are blood products indicated, and administration of blood products should be concurrent with antivenom administration. 1 –3 Our patient received 4 vials of antivenom, as well as packed red blood cells shortly after presentation to the emergency department. Although the recommended initial dose for Crotalidae polyvalent immune Fab is 4 to 6 vials, this dose has only been studied in minimal to moderate envenomations. 6 When patients present to our service who are critically ill from their envenomation, our routine practice is to administer an initial dose of 10 vials of antivenom, because we have found that these patients ultimately receive multiple back-to-back loading doses equivalent to at least this amount. We administer this 10-vial dose over 1 hour or more rapidly if tolerated.
In the intensive care unit, the patient received multiple blood products and antivenom but continued to bleed, even after his platelets were documented to have risen to 57 K/mm3. It was not until he received recombinant factor VIIa that the bleeding stopped. Experience with recombinant factor VIIa for treatment of severe bleeding has been increasing in recent years. It is thought to act at the site of tissue injury and vascular wall disruption by binding exposed tissue factor, generating thrombin, and ultimately leading to platelet activation and further activation of coagulation. 7 –9 Recombinant factor VIIa has been used in the settings of gastrointestinal hemorrhage, severe thrombocytopenia, and coagulopathy.7,10 This is the first report of use of recombinant factor VIIa in the treatment of hemorrhage associated with rattlesnake envenomation.
This patient had multiple reasons for developing coagulopathy and thrombocytopenia. Although he clearly had severe venom-induced thrombocytopenia and coagulopathy, he also had a history of thrombocytopenia and liver disease due to alcohol abuse, and profuse hemorrhage surely led to further consumption of platelets and clotting factors. When he arrived to the intensive care unit, he had severe metabolic acidosis and hypothermia, each of which may lead to coagulopathy. 9 Finally, large volume resuscitation would also produce a dilutional coagulopathy. 9 Many of these contributing factors may have made him an ideal candidate for use of recombinant factor VIIa. Even though his platelets had increased, they were likely dysfunctional, and recombinant factor VIIa may have allowed platelet activation through thrombin generation by binding to tissue factor, leading to increased platelet-platelet interactions and aggregation and ability to form a stable fibrin clot.8,9 In addition, recombinant factor VIIa may be able to accomplish this in the absence of some clotting factors, making it useful in such situations as liver disease, where there may be decreased synthesis of clotting factors, or dilutional coagulopathy, where clotting factors are deficient and platelets are dysfunctional.8,9
Recombinant factor VIIa may be ineffective in the presence of severe acidosis. 9 Our patient had been treated with sodium bicarbonate and large amounts of intravenous fluids, which likely led to an improvement in his acidosis before administration of recombinant factor VIIa. Additionally, it is recommended that alternative blood products be administered to achieve a hematocrit >24%, platelets >50 000/mm3, and fibrinogen >100 mg/dL before using recombinant factor VIIa. 9 A large amount of blood products were administered to our patient before he received recombinant factor VIIa, with the hematocrit and platelets reaching recommended thresholds. Although the fibrinogen was not documented at this time, the 10 units of cryoprecipitate that had been given likely transiently increased the fibrinogen to more than 100 mg/dL.
Many blood products were administered in this case, and it is impossible to know whether the combination of therapies, even without recombinant factor VIIa, would have led to cessation of bleeding. The hemorrhage did appear to respond temporally to recombinant factor VIIa, however, and it makes sense mechanistically that this therapy might be helpful in this setting. This is a very expensive treatment, though, with the hospital cost of the dose given to our patient approximating $7000, and should be reserved for severe bleeding unresponsive to more conservative and standard therapy.
Although this patient's clinical presentation was dramatic, the initial coagulopathy and thrombocytopenia that occurred were not unusual. These laboratory findings are common in patients with rattlesnake envenomation, generally reversed with antivenom, and usually not associated with bleeding. 1 –3 Although the influence of chronic alcohol use or liver disease on outcome after snake envenomation has not been studied, many of the patients admitted to our service with thrombocytopenia and/or coagulopathy after rattlesnake bite have these pre-existing conditions, and we have rarely observed serious bleeding in these patients. It certainly makes sense that such conditions might predispose to bleeding disorders, however.
We do not feel that this patient had disseminated intravascular coagulation. Severe bleeding may occur in the setting of overt disseminated intravascular coagulation and occurs very rarely after North American rattlesnake envenomation.3,11 The mechanism for development of disseminated intravascular coagulation in such cases may be related to endothelial injury associated with direct intravascular injection of venom and activation of the coagulation cascade.2,3,11,12 In such cases, hemorrhage is generally diffuse and involves multiple organ systems, and organ infarction often occurs.2,11,12 Isolated upper gastrointestinal bleeding would not be expected.
It was initially suspected that esophageal varices were the source of the patient's bleeding, considering his history of ethanol abuse. Surprisingly, no varices were found on endoscopy. The hemorrhage arose from a single Mallory-Weiss tear. It is unknown whether this tear developed secondary to vomiting from alcohol consumption or after the envenomation. The severe uncontrolled bleeding almost certainly occurred as a result of the effects of venom on the patient's hematologic system in conjunction with the tear. We have seen Mallory-Weiss tears in other patients with rattlesnake bite.
Although we were initially able to resuscitate this patient, he developed several severe complications that were ultimately terminal. It is likely that the combined effects of the envenomation (shock, coagulopathy, and thrombocytopenia) and his pre-existing medical conditions (thrombocytopenia, alcohol dependence, and liver disease) predisposed this patient to a fatal outcome after development of a Mallory-Weiss tear. Although we cannot say for sure that recombinant factor VIIa was responsible for stopping the patient's acute hemorrhage, cessation of bleeding was temporally related to its administration. We believe this therapy should be reserved for the rare patient with severe, life-threatening hemorrhage after rattlesnake envenomation, in whom aggressive antivenom therapy and necessary blood products have failed. Although this is a single case report, we believe recombinant factor VIIa is a potentially useful tool for clinicians to be aware of if faced with similar cases.
Conclusion
Life-threatening hemorrhage after envenomation by a North American rattlesnake is uncommon. We report a case of upper gastrointestinal bleeding after rattlesnake envenomation, in which bleeding was controlled after administration of recombinant factor VIIa. This therapy should be considered in similar cases of life-threatening hemorrhage after rattlesnake envenomation that is resistant to traditional therapies.
Footnotes
*
Previously presented in poster form at the North American Congress of Clinical Toxicology annual meeting in San Francisco, CA, October 2006.