
Abstract
Objective
Expedition activities such as mountaineering, rock climbing, river running, sea kayaking, and canoeing all involve an element of risk. Organizations that provide group wilderness and adventure experiences are responsible for managing the risk of their courses. The leaders and medical providers of these trips must therefore be prepared to anticipate and manage medical problems that may arise. The aim of this study is to provide the medical community with a better understanding of the specific injuries and illnesses that occur on wilderness expeditions.
Methods
A retrospective descriptive study was done examining the medical incidents that occurred on wilderness-based courses during the 3-year period from September 1, 2002, through August 31, 2005. Participants and staff of the National Outdoor Leadership School (NOLS) served as the study population.
Results
Injuries occurred at a rate of 1.18 per 1000 program days, and illnesses at a rate of 1.08 per 1000 program days. There were no fatalities during the time period. Athletic injuries (sprains, strains) and gastrointestinal illnesses were the most common medical incidents. Hypothermia, seizures, appendicitis, heat stroke, and pregnancy occurred but with low frequency. Fractures, dental emergencies, tick fever, athletic injuries, and nonspecific body pains were the conditions most frequently requiring evacuation.
Conclusions
The rate of medical incidents on NOLS courses declined during the 1990s and has remained relatively steady apart from a slight increase in 2004 and 2005. Athletic injuries continue to be a difficulty, as they frequently result in evacuation even though their ultimate outcome is usually benign. Evacuation decisions should be made considering both the potential severity of the medical condition as well as patient comfort. Wilderness medical personnel must be familiar with a diverse range of medical conditions in order to provide optimal care.
Introduction
The business of wilderness and adventure expeditions has seen an enormous growth in the last few decades. Various national and international programs offer experiences such as mountaineering, rock climbing, river running, sea kayaking, and canoeing and range from short river trips to expedition climbing in the Himalaya. The environmental mediums are therefore extensive. Mountains, rivers, and oceans provide the course areas. Many programs also include leadership training and other personal educational goals in their curricula to achieve an experience far beyond that of an ordinary outdoor excursion.
These activities are not without risk, however. While all of these programs strive to be safe, each has a different approach to risk management and a different tolerance to risk. Managing this risk is therefore a vital concern in all outdoor recreation. Injuries or other medical situations in the wilderness often create complex logistical and practical challenges. The remote environments in which these organizations operate make medical care and evacuation challenging or even impossible. Evacuation decisions hinge on a variety of factors including the medical training and experience of the leader(s), available medical supplies, the ability of the patient to tolerate discomfort, the possibility of conducting an evacuation, and available external evacuation resources. Analyzing wilderness injuries and illnesses can lead to a better understanding of the types of incidents that require rescue and how to best manage these evacuations.
The National Outdoor Leadership School (NOLS) is a wilderness education organization based in Lander, Wyoming, which has been teaching leadership in the outdoors since 1965. The school conducts outdoor leadership training and wilderness skills to individuals over the age of 14. The average age of participants is 22 years old. The following environments serve as course areas: the central and northern Rocky Mountains, Alaska, the Pacific Northwest, and southwestern United States; Baja California, Mexico; the Patagonia region of Chile; the Yukon Territory and Coast Ranges of Canada; northwestern Australia; South Island of New Zealand; the Indian Himalaya; and the Amazon River Basin of Brazil. All NOLS instructors have a minimum of Wilderness First Responder medical training. Courses range in length from 2 weeks to 3 months and utilize the activities of high altitude mountaineering, rock climbing, river rafting, kayaking, canoeing, sailing, backpacking, horse packing, and caving. NOLS is one of the largest wilderness education programs. The vast array of activity types, environments, and participants makes NOLS an ideal model through which to study wilderness incidents.
This study examines the medical incidents that occurred on wilderness-based courses of NOLS during the 3-year period from September 1, 2002, through August 31, 2005. By examining this information, we provide the wilderness and medical community with a better understanding of the specific injuries and illnesses that occur on wilderness expeditions. This understanding can be used to direct education toward prevention as well as education for physicians, instructors, and rescuers who are involved with these types of medical incidents.
Methods
In 1984, NOLS created a comprehensive safety database to record incident data. This database includes all injuries, illnesses, near-miss incidents, and evacuations that occur on courses and is the largest and consistently the longest running in the industry. The following criteria have been predetermined by NOLS management for what constitutes a reportable incident: injury or illness that requires more than simple first aid (for example, blisters, though common and requiring first aid, are reported only if they meet one or more of the additional criteria). injury or illness that requires follow-up care or the use of prescription medications. injury or illness that interferes with active participation for 12 hours. injury or illness that requires evacuation.
When an incident occurs, the instructor team records the details on paper report forms while in the field. These reports are presented to the program management staff at the end of the course at each school location for review and discussion during course debriefing. The program staff then records the incident details into the master database. This database is a custom application built on an Oracle platform and is accessible to NOLS managers via the Internet. The NOLS risk management director reviews all records and standardizes category classifications prior to finalizing the record. Data are exported from the database to another custom application developed in Filemaker Pro Version 6 when analyzing records.
This study uses an emergency medicine classification in which illness is defined as an interruption, cessation, or disorder of body functions, systems, or organs and represents a “medical” problem. Injury is defined as damage, harm, or loss, as a result of an external force and correlates to a “trauma” problem. “Athletic injuries” include strains and sprains of ligaments, muscles, and tendons. “Soft tissue” injuries include contusions, abrasions, and lacerations. “Immersion foot,” also known as trench foot, refers to neurovascular damage occurring after prolonged exposure of damp or wet feet to temperatures of 0 to 10 degrees Celsius. “Gender” illnesses refer to urinary and vaginal infections in women. These definitions were established when the NOLS database was created.
A “program day” is defined as one person on a course for one day. In the illness category, “infection” includes both viral and bacterial infections not associated with soft tissues, and includes eye, ear, and dental infections. “Flu symptoms” include viral syndromes such as general malaise, fatigue, rhinorrhea, and body aches. “Respiratory symptoms,” while often a component of flu symptoms, are distinguished because of their primary pulmonary component. “Gastrointestinal illnesses” include nausea, vomiting, or diarrhea as the chief complaint. An infection associated with a wound is classified as an injury. Otherwise infections are classified as illnesses.
Medical evacuations are defined as a situation in which the patient must leave the field. Evacuations are further classified as assisted or unassisted. Assisted is defined as requiring an additional level of support in order to remove the patient from the field. These may utilize a helicopter, bush plane, horse, boat, or a litter and rescue team. These forms of transport may not be due to urgency but may be the standard transport system in the specific remote area. An unassisted evacuation is one that can be performed by the patient or by the group with minimal resources.
Institutional Review Board Approval and Statistical Analysis
The study was reviewed and approved by the University of Utah Institutional Review Board. SPSS 14.0 (SPSS Inc, Chicago, IL, 2006) was used to analyze data. Logistic regression was used to determine trends in incident rates and to determine odds of evacuation based on medical complaint. All tests were 2-tailed with significance set at 0.05.
Results
During the study period, there were 441 855 program days. A total of 996 medical incidents were recorded. No fatalities occurred during the period. Table 1 reports a summary of the rates of incidents since 1984. Medical incident rates have decreased 3.9% on average each year since data recording was initiated (odds ratio [OR] = 0.961, 95% CI [0.96, 0.97], P < .0005). Incidents decreased 4.5% on average each year (OR = 0.955, 95% CI [0.946, 0.963], P < .0005) during the first 12-year period and increased 1.5% on average each year (OR = 1.015, 95% CI [1.001, 1.030], P = .037) during the second 9-year period. The slopes of incident rates of these 2 time periods are significantly different (P < .0005) (Figure).
Incident numbers and rates (1984–2005)
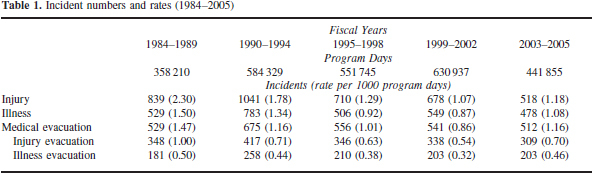
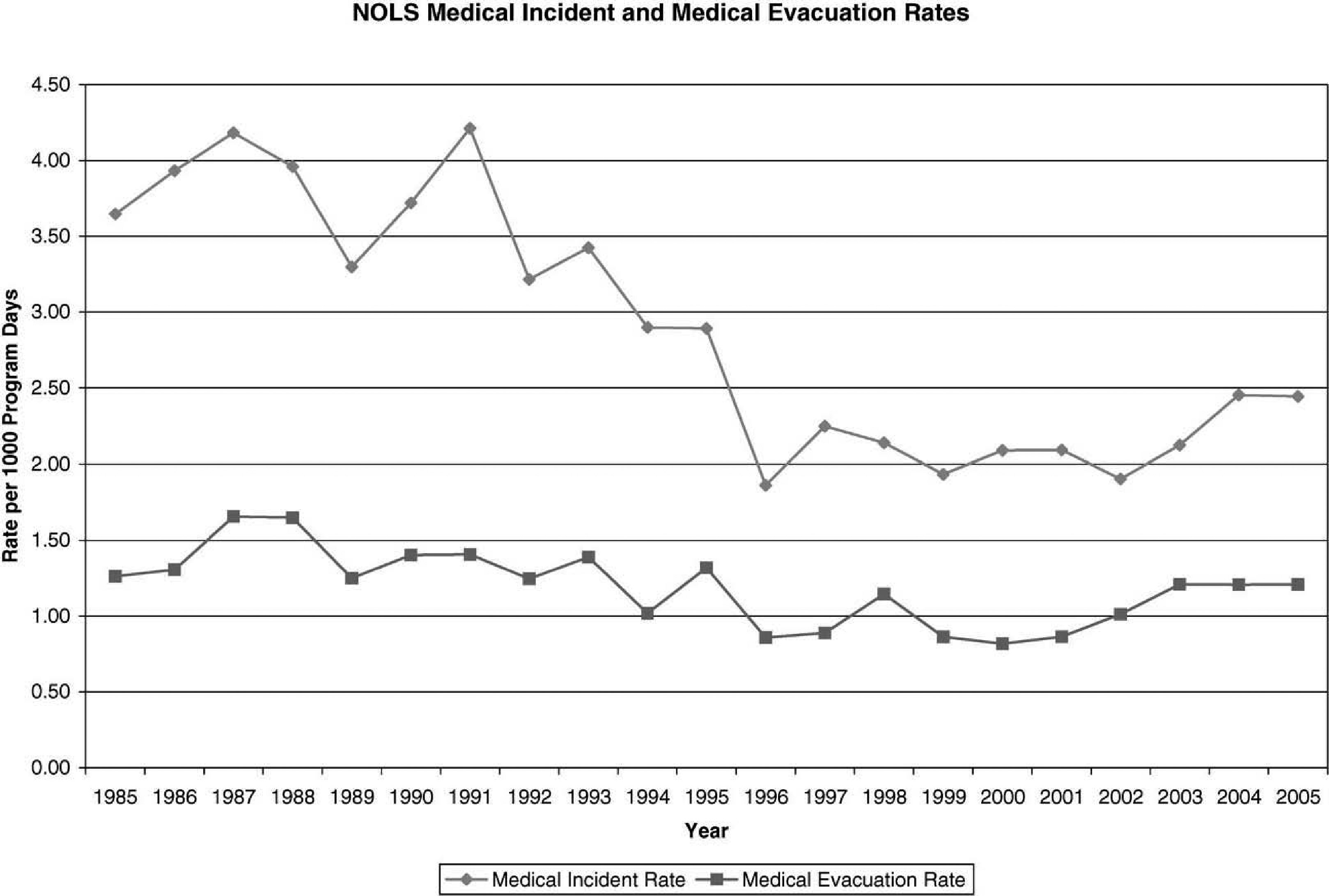
Rates of medical incidents and evacuations on NOLS courses from 1985 through 2005.
Students were involved in the majority of incidents (870). Staff was involved in fewer incidents (126). Of the 996 incidents, 555 (56%) involved males and 441 (44%) females. The average age of participants with incidents was 22 years old. Incidents occurred at a mean of 27 days spent in the field (median = 19 days, 5% trimmed mean = 25 days) when their incident occurred.
Injuries
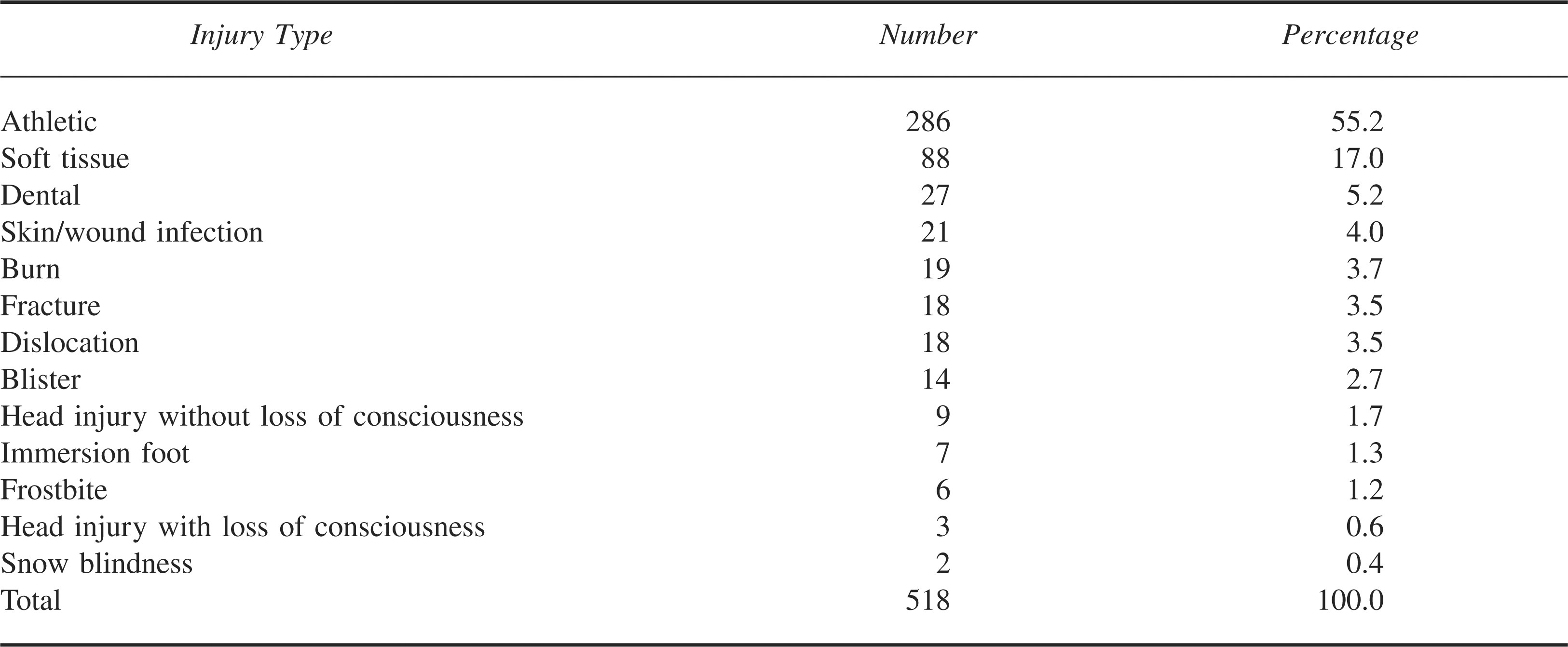
Table 2 reports the types of injuries sustained. The vast majority were strains and sprains. External trauma including skin and soft tissue injuries comprised the second largest group. Relatively few incidents involved bony injuries, including fractures and dislocations. Fifty-eight percent of injuries occurred in males. All of the burns occurred while cooking or near camp stoves. Of the 518 injuries, 308 (59.5%) required evacuation from the field. Of the participants who were injured, 22% represented re-injury or exacerbation of a previous injury on the course (verified by review of past medical screening history).
Injury profile (2002–2005)
Illnesses
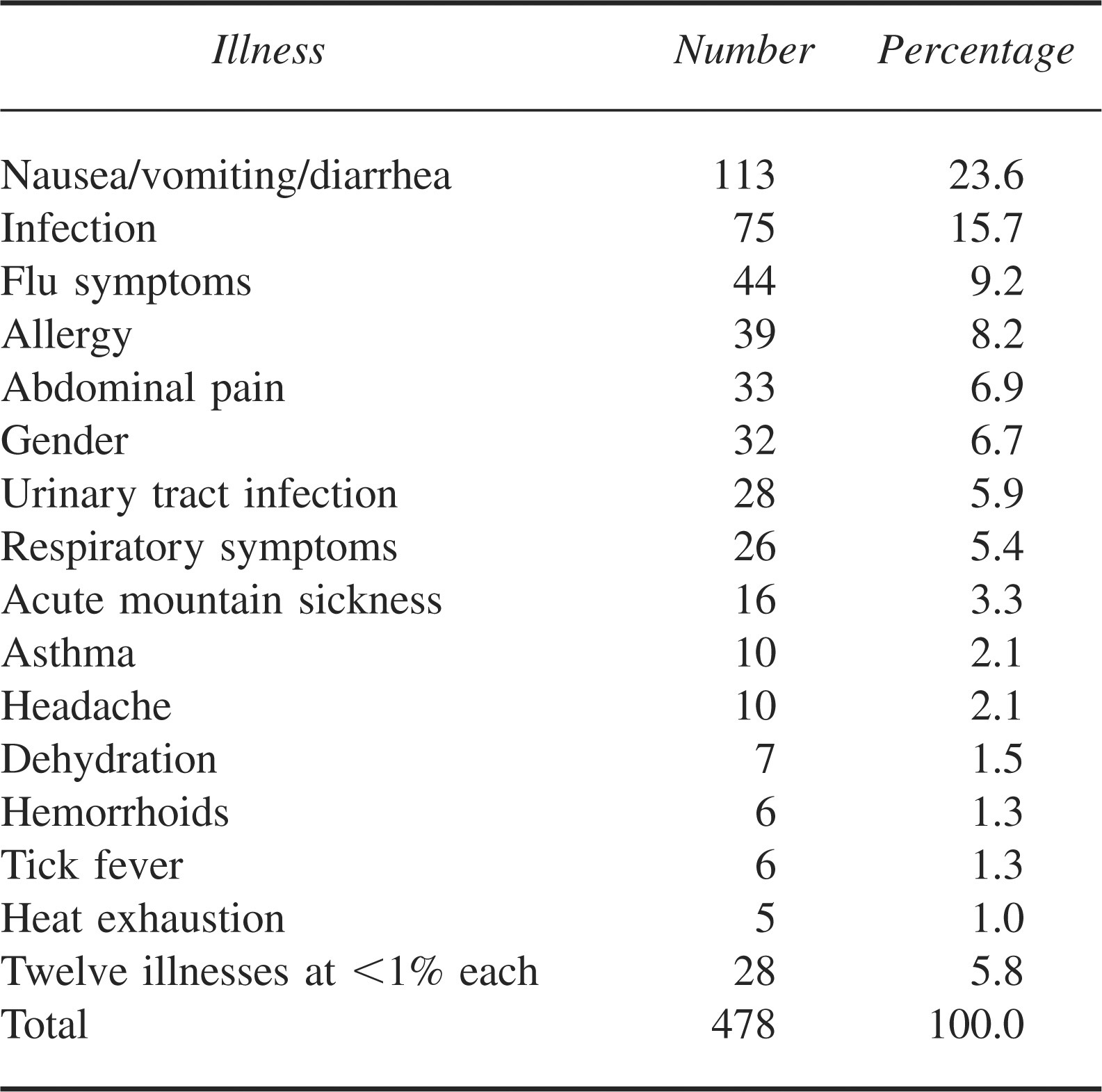
Table 3 shows the types of illnesses acquired. There were 478 reported illnesses during the study period. Of these, 113 (23.6%) were gastrointestinal incidents. There were 75 (15.7%) infections and 44 (9.2%) incidents of flu symptoms. When combined, the respiratory and flu symptom illnesses make up 70 (14.6%) of the illness-related incidents. A total of 204 (42.7%) illness-related incidents required evacuation. Hypothermia, seizures, appendicitis, and heat stroke were observed during the study period and each comprised less than 1% of total illnesses.
Illness profile (2002–2005)
Evacuations
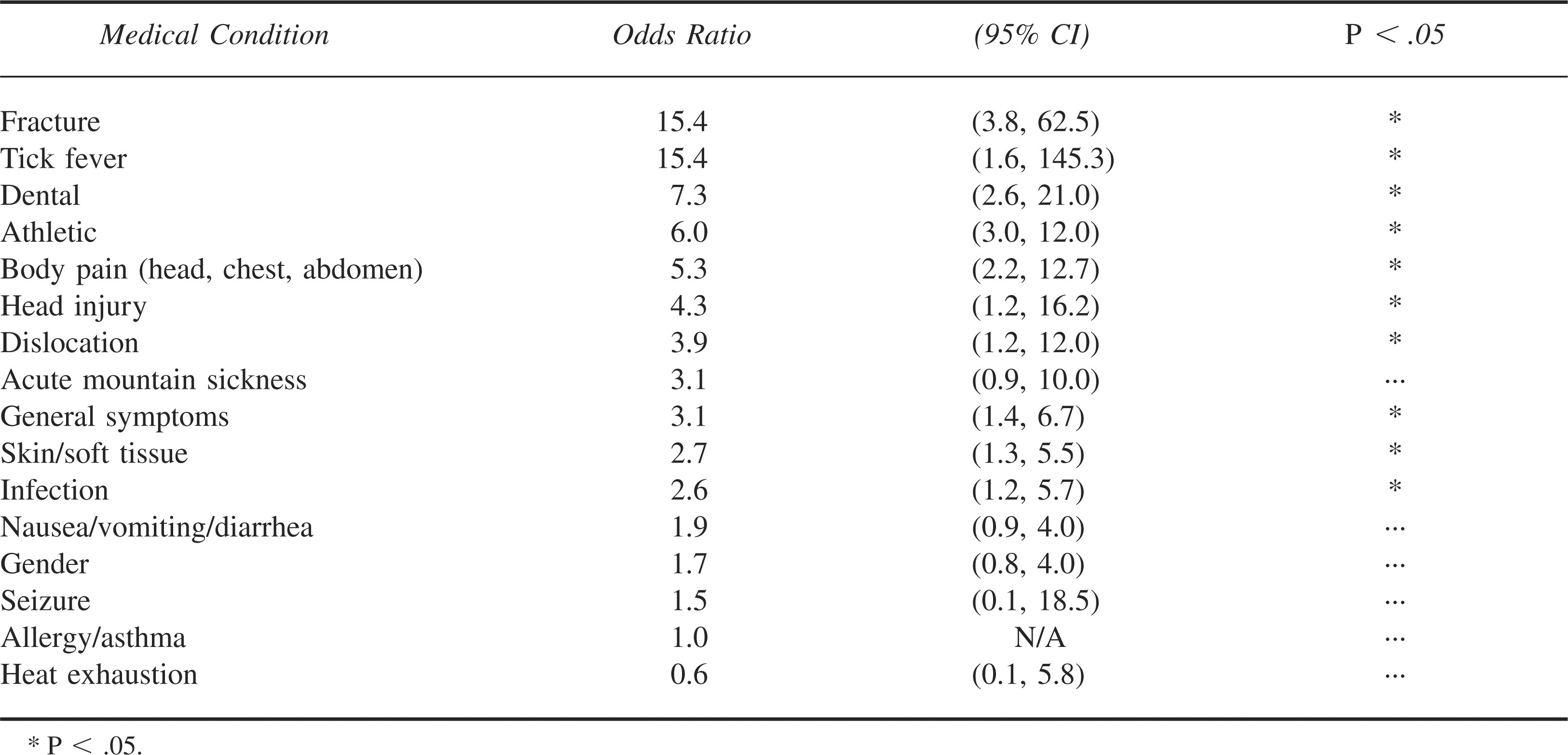
Just over half (51.4%) of all incidents resulted in evacuation from the field. Of the evacuations, 204 (39.8%) were related to illnesses and 308 (60.2%) were related to injuries. Of the injury evacuations, 78 (25%) were “assisted.” Forty-six (22%) of the illness evacuations were assisted. Table 4 shows odds ratios for evacuation based on medical category.
Evacuation odds ratios (2002–2005)
Hospitalized
Forty-one (4.1%) of the total incidents required admission to the hospital. Twenty-three (56.1%) of these cases were injuries and the remainder were illnesses.
Wilderness Activities
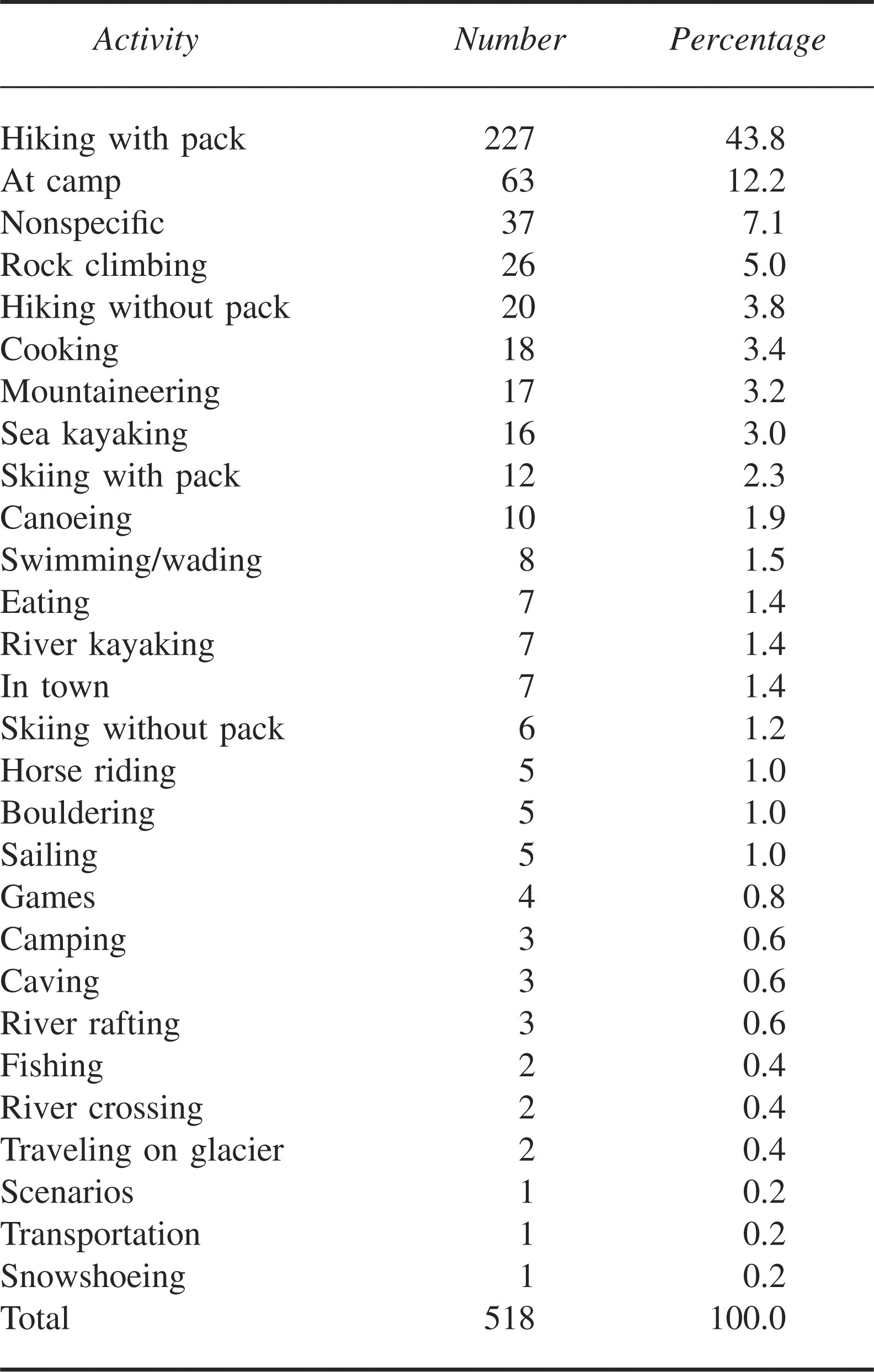
Hiking was the most common activity during which people were injured and comprised 247 (47.7%) of the activities at the time of injury. Seventy (13.5%) of the injuries occurred while people were at or around camp. Fifty-one (9.8%) of the injuries took place during water-related activities and 50 (9.7%) occurred while participants were taking part in a mountaineering activity. Table 5 displays the complete list of activities during which injuries occurred.
Activity during injury (2002–2005)
Discussion
Injury, illness, and evacuation rates in this study were low overall and have been decreasing over the years. Rates were lower than those in the 1980s and similar to those from 1995–2002. 1 All types of medical incidences during this study period showed small increases compared with the previous study period of 1999–2002.1,2 However, no large increases in any of the incident categories were demonstrated. It is possible that incident rates on NOLS courses reached a nadir in 1996 and are undergoing a baseline fluctuation. Ongoing analysis of incident rates will help illuminate these questions.
Athletic injuries continue to make up the majority of incidents that occur in the backcountry. These data are consistent with past NOLS studies as well as other reported wilderness expedition studies.3,4 With the high prevalence of athletic injuries, strategies to prevent their occurrence are vital. NOLS prevention strategies include reducing pack weights, carefully planning course routes to avoid overly demanding terrain early in a trip, emphasizing warm-up and stretching before hiking and strenuous activities, and deliberately teaching students how to hike on rugged and uneven terrain. NOLS is also experimenting with a series of “lightweight” backpacking courses in which students carry 25 lb (11.3 kg) packs vs the standard 50 lbs (22.6 kg). Injury rates from these courses will help determine whether lighter pack loads decrease the number of athletic injuries.
Athletic injuries were also some of the most frequently evacuated medical conditions in this study. On an active expedition, a sufficient amount of rest to heal an athletic injury is rarely possible. In addition, the discomfort of any medical problem is amplified in the wilderness. Patient tolerance for adversity is an important factor in the decision to remain in the field or evacuate. Even though athletic injuries themselves are not frequently serious, they continue to be a significant source of logistical challenges and lost course time.
A notable percentage of participants who suffered athletic injuries had a history of the specific injury prior to course start. Medical screening is an important aspect of wilderness courses. Previous injuries demand a thorough investigation to determine whether or not the injury will cause difficulties during the course. However, the recency and types of injuries that should generate red flags during the screening process have not been delineated. This remains an important topic for further study.
Wounds are common on wilderness courses and can be challenging to care for on prolonged expeditions. Most wounds do not warrant evacuation and therefore must be protected and kept clean under potentially unhygienic conditions. Formerly a problem at NOLS, wound infection rates have been declining. Wound infections decreased from a rate of 0.10 per 1000 participant days during the 1984–1989 time period 1 to 0.02 and 0.04 per 1000 participant days during the 1999–2002 2 and 2002–2005 times periods, respectively. 2 This decline is likely the result of better staff training in wound care as well as awareness of the potential for wound infections.
Similar to athletic injuries, gastrointestinal illnesses continue to be the leading cause of illness in wilderness settings. These results are consistent with past NOLS database analyses as well as other reported expedition illness profiles.3,4 Strict hand-washing techniques, water disinfection, and washing of common cooking utensils are the primary methods to decrease incidents of nonspecific gastrointestinal illnesses. These methods have been emphasized by NOLS, especially after early studies 1 revealed the relatively high prevalence of gastrointestinal illnesses. Gastrointestinal illnesses have decreased from a rate of 0.44 per 1000 participant days during the 1984–1989 time period 1 to 0.20 and 0.26 per 1000 participant days during the 1999–2002 2 and 2002–2005 times periods, respectively. 2 Compliance is always a problem in the wilderness. Pretrip travel and cultural encounters during a course present hygiene challenges as well. Fortunately, in most cases gastrointestinal illnesses can be managed in the field without evacuation.
Wilderness medicine is defined as the care of patients in environments farther than 1 hour away from definitive medical care. 5 Typically wilderness medicine involves longer patient contact times, challenging environments, limited resources and equipment, and independent decision making. As shown in this study, the wilderness provider must be familiar with a diverse range of medical complaints and conditions. A gap in this knowledge set could prove detrimental to the patient and expedition overall. While providers might not always know the complete medical treatment, they must be able to initially diagnose and manage all of these medical conditions.
Limitations
There are several limitations to this study. First, its retrospective nature limits the available data to that predetermined by the NOLS database. Second, the individual instructor team must decide whether or not to define a situation as an incident and to report it, potentially introducing reporting bias. Third, nonevacuated illnesses are likely frequently underreported, as many typically resolve without treatment and may not prompt an alteration of the course or potential evacuation. Fourth, data are derived from one organization. Despite these limitations, to our knowledge the NOLS database is the most comprehensive record of wilderness medical problems available.
Conclusions
The low and declining medical incident rates on NOLS courses are evidence that risk in the wilderness can be managed effectively. The wilderness environment offers additional challenges of difficult diagnoses, treatment limitations, and rescue decisions to normal urban medical practice. Wilderness instructors must have a broad understanding of the conditions described in this article in order to provide competent medical care on expeditions. While risk can never be completely eliminated from wilderness expeditions, it can be mitigated by proper prevention and management.
Footnotes
Acknowledgments
Two of the coauthors (DL and TS) are employed by NOLS.