
Abstract
To the Editor:
Minimally invasive total hip arthroplasty (THA) is a procedure that has been embraced by some enthusiasts in the orthopedic community. This technique purportedly offers less blood loss, less pain, a shorter hospital stay, 1 and reduced postoperative pain 2 compared to hip arthroplasties performed with a standard incisional approach. Minimally invasive THA is performed using either 1 or 2 smaller incisions. A single-incision THA is designated “minimally invasive” if the incision is less than 10 cm. 3 The 2-incision technique is more controversial and requires greater technical expertise. 3 Using fluoroscopic guidance, 1 incision is made over the femoral neck for insertion of the femoral component while a second is made in the posterior lateral buttock for the acetabular component. Both approaches have been performed successfully on both lean and heavier patients, but this procedure is technically difficult when performed on the obese. 4 This technique avoids muscle and tendon transection, thereby theoretically hastening recovery and allowing a shorter hospital length of stay. 4 Intraoperative and early postoperative complications have been between 1% 4 and 6%, 1 with complications decreasing with the experience of the surgeon. 1 Long-term functional outcomes, beyond the immediate postoperative period, are less often described in the orthopedic literature. One of the authors of this letter had such a procedure and was able to return to mountaineering activities 7 weeks postoperatively.
The author suffered a serious fall while alpine climbing at the age of 21 in the Wind River Range of Wyoming (USA). After the fall, he experienced modest left hip pain. The hip pain resolved within approximately 2 weeks and he recovered completely, continuing to pursue rock-climbing, running, and mountaineering into his 40s. At that time, he began to develop left hip pain with activity and ultimately pain at rest, including nocturnal pain. One year of anti-inflammatory medication did little to alleviate the pain, and he subsequently sought orthopedic care. At physical exam, he had a significantly limited range of motion on internal rotation; external rotation was 15°. Flexion was limited to 110°. Radiograph of the left hip showed severe arthropathy with large osteophytes present medially and inferiorly, while the uninjured right hip was relatively normal.
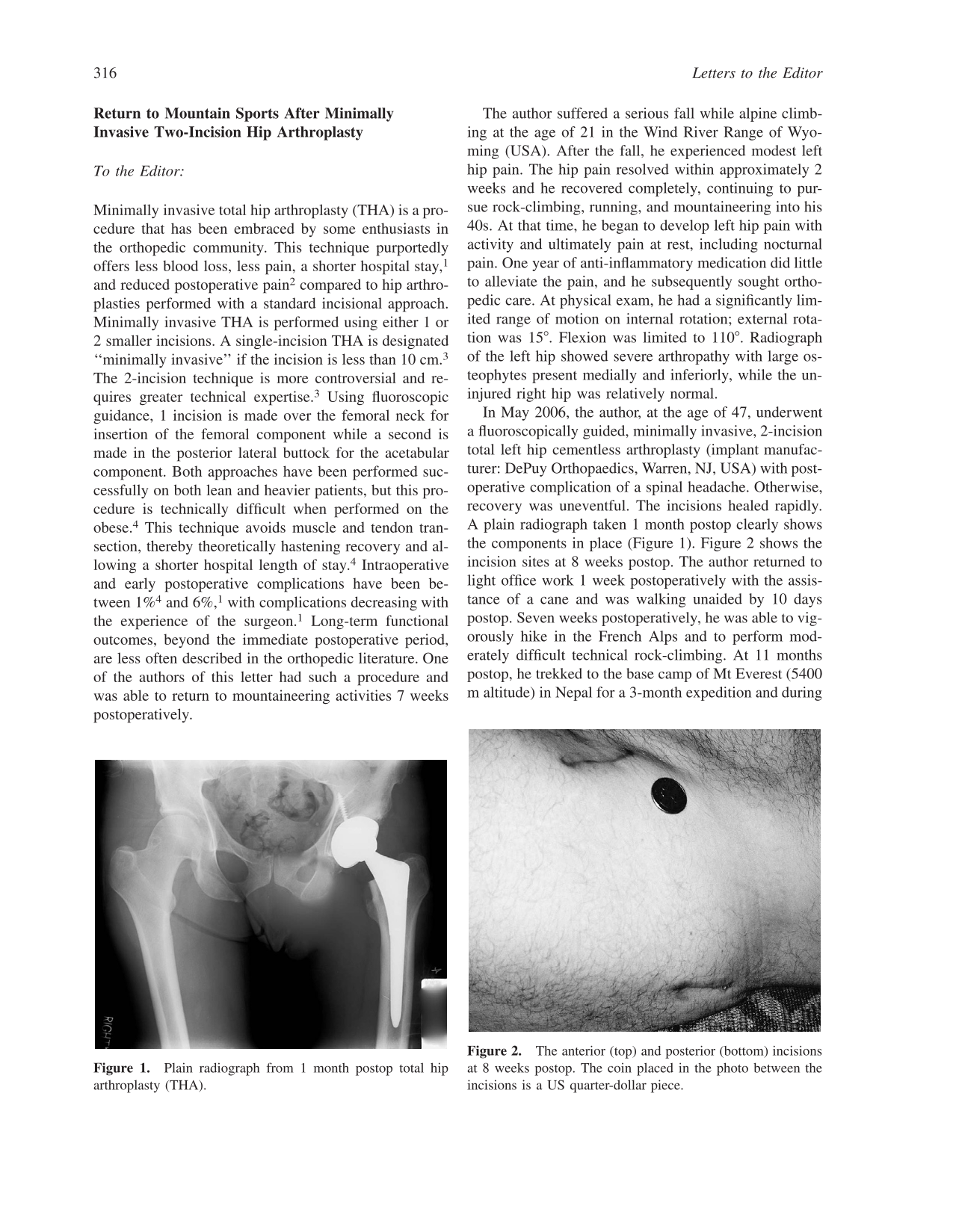
In May 2006, the author, at the age of 47, underwent a fluoroscopically guided, minimally invasive, 2-incision total left hip cementless arthroplasty (implant manufacturer: DePuy Orthopaedics, Warren, NJ, USA) with postoperative complication of a spinal headache. Otherwise, recovery was uneventful. The incisions healed rapidly. A plain radiograph taken 1 month postop clearly shows the components in place (Figure 1). Figure 2 shows the incision sites at 8 weeks postop. The author returned to light office work 1 week postoperatively with the assistance of a cane and was walking unaided by 10 days postop. Seven weeks postoperatively, he was able to vigorously hike in the French Alps and to perform moderately difficult technical rock-climbing. At 11 months postop, he trekked to the base camp of Mt Everest (5400 m altitude) in Nepal for a 3-month expedition and during this time climbed a 6200-m peak unaided. He resumed his preoperative activity of running 9 months postop and is presently able to run pain-free for a distance of 3 miles, 2 to 3 times weekly (in addition to unlimited participation in lower-impact exercise).

Plain radiograph from 1 month postop total hip arthroplasty (THA)

The anterior (top) and posterior (bottom) incisions at 8 weeks postop. The coin placed in the photo between the incisions is a US quarter-dollar piece
In 2003, Peters 5 described another case report of a 69-year-old with bilateral cementless standard THA having participated in mountain sports 5 to 7 months postoperatively. Although it is generally recommended that high-impact sports such as this be delayed until at least 4 to 6 months after standard hip replacement 5 as a result of the risk of aseptic loosening, the literature contains little mention of long-term outcomes of the minimally invasive procedure. In addition, conflicting evidence exists regarding the outcomes of this procedure in the scant extant published work on the subject. Ogonda and colleagues 2 performed a randomized, blinded single-surgeon study of 219 patients comparing minimal vs standard incision techniques for early postoperative outcomes of THA, including pain, analgesia use, early walking ability, and functional outcome at 6 weeks. No significant differences were detected. Similarly, in a prospective, randomized trial, Lawlor and colleagues 6 compared single-incision minimally invasive THA (<10 cm) with standard incision surgery (16 cm) with respect to functionality and mobility in the early (2-day) postoperative period in 219 patients with a mean age between 67.4 (minimal incision) and 65.9 (standard incision) years. A single surgeon performed all surgeries. Lawlor and colleagues found no significant benefit in the ability to mobilize and perform functional tasks necessary for hospital discharge, nor was there a difference in the postoperative pain scores. In addition, there was no significant difference in ambulation velocity 6 weeks postsurgery. A somewhat different picture emerges in a study described by Berger. 4 This prospective work involved 100 patients undergoing minimally invasive THA who, with the help of a rapid rehabilitation program, were able to return to work in 8 days, resume activities of daily living in 10 days, and walk one half mile in 16 days. On the contrary, Pagnano and co-workers 7 described modest outcomes and substantial postoperative complications of minimally invasive THA in a cohort of older, more-typical arthroplasty patients with a mean age of 70.5 years.
Although this letter in no way endorses disregard for individual physicians’ recommendations, the author was advised to “let pain be your guide,” given the dearth of long-term outcome research for this technique. The benefits of this procedure in the immediate postoperative period and the muscle-sparing nature of minimally invasive THA have the potential to benefit those who intend to use the prosthesis for high-risk occupational and recreational activities such as mountaineering. However, research on short-term outcomes is conflicted and does not consistently bear this out, while there is little long-term outcome research to guide the surgeon and patient.
This author enjoyed a rapid return to full and high-risk activities after minimally invasive THA, and nearly 2 years after this procedure has experienced no complications that require curtailment of these recreational pursuits.