
To the Editor:
We were fascinated by the evaluation by Platts-Mills et al of various methods to warm intravenous (IV) fluid in the field. 1 The capacity of cool IV fluid to lower core temperature is concerning. 2 When IV fluid is needed in the field, we need a way to give it without doing harm. We noted their comment that many have suggested using body heat to warm fluid but can find no reference to whether this works or not. We decided to see whether we could warm cool fluid next to the body and whether we could maintain the temperature of previously warmed fluid in a cold wilderness environment.
The experiment was done in Lilburn Cave in Kings Canyon National Park as part of an expedition of the Cave Research Foundation. The cave is at an elevation of 1500 m and is a constant 8°C throughout. All the IV fluid and the thermometer were placed in the cave the night before to reach temperature equilibrium. Temperatures were measured using a Traceable® 4045 digital thermometer with a penetrating thermistor probe (Control Company, Friendswood, TX). It was calibrated by measuring the temperature at boiling water at 100 m elevation.
The next day, 6 volunteers each placed a 500 mL bag of normal saline (Hospira Inc., Lake Forest, IL) in a thin fleece pouch that maintained it on their abdomen or in their axilla of choice. The pouch was worn over a thin underwear layer. Three volunteers took saline that had been in the cave overnight, while the other 3 took bags of fluid that had been warmed together in a pot of water heated on a woodstove to 75°C and then transported into the cave. After measuring ambient air temperature, baseline fluid temperature was taken in each bag by piercing it with the probe. The probe was placed in the middle of the fluid for at least 15 seconds or until the temperature stabilized. The punctured bag was then sealed with duct tape and placed in the pouch. Each bag was stripped of its outer packaging but kept in a self-sealing plastic bag to avoid leakage. Each participant wore whatever layers he or she felt appropriate on top of this. Typically, this was a layer of fleece covered by a ballistics cloth cave suit. Temperature measurements were repeated after 1 and 2 hours of moving through and working in the cave.
The next day, the procedure was repeated with cool fluid only by 4 volunteers hiking out. The saline was removed from the cave 1 hour prior to hiking. Temperatures were taken at the start of the hike and at 2 hours. A 1-hour measurement was skipped because the group was hiking out in a cold rain. Again, the fluid was kept in a pouch on top of 1 layer. At the 2-hour point, the hikers had walked 8 km and gained 250 m in elevation.
Measurements (Figure) confirmed the constancy of the ambient temperature in the cave. The first reading near the entrance was slightly higher because the cave was drawing outside air at the time. Mean temperature of the cool saline increased from 6.2°C at baseline to 15.0°C at 1 hour and 19.2°C at 2 hours. The warmed fluid was significantly warmer than the intended 45°C, despite a 15-minute delay to get it inside the cave. Its temperature declined from 58.4°C to 42.2°C to 34.9°C. Despite the hotter-than-intended temperature, volunteers were quite pleased to carry it next to their body inside the cave.
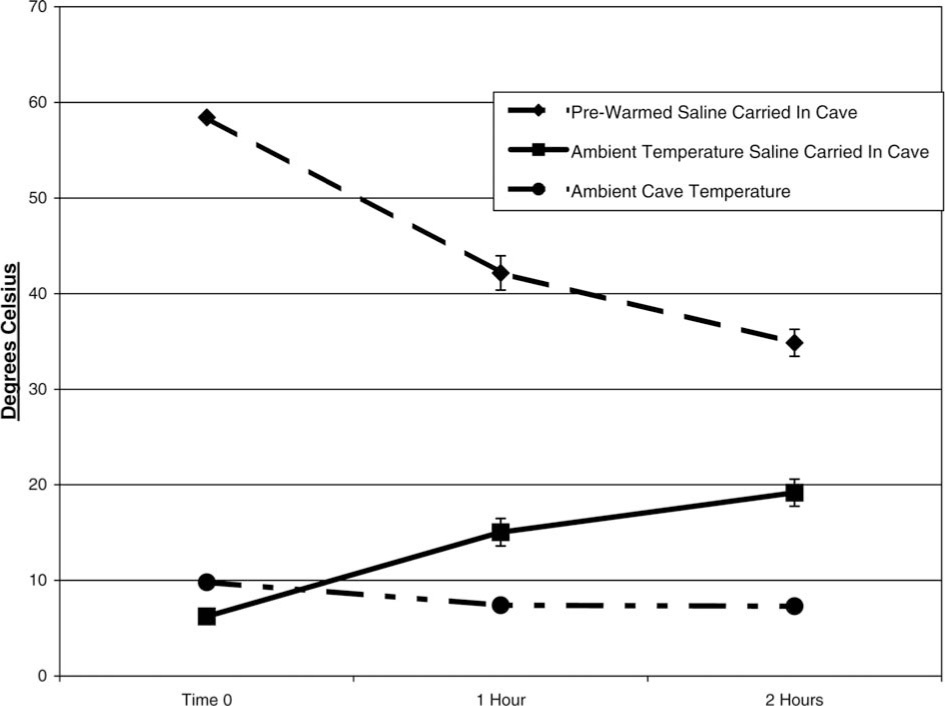
Temperature change over time.
Outside, the ambient temperature varied. At the end of the hike, it was 5.8°C. Fluid temperature increased from 9.4°C to 17.6°C after 2 hours of hiking.
From these findings, we drew 3 conclusions. First, carrying IV fluid next to the body while transporting it in a cold wilderness setting is better than doing nothing. It cannot, however, be counted on to raise the temperature to a level that will avoid further core temperature decreases when infused. If core temperature drop will be important, then rescuers need a more definite plan on how to raise fluid temperature higher once at the patient. Partial warming is moot if the fluid is to be warmed on a camp stove at the scene, as suggested by Platts-Mills et al, but might be helpful if it will be further warmed there with chemical heat packs. Carrying overly warmed fluid next to the body anticipating a temperature drop might be appropriate, but predicting when it will reach appropriate infusion temperature will be difficult.
Second, as one might expect, temperature rise was proportional to the number of insulating layers worn over the fluid. Just wearing it next to the body with nothing over it had little effect.
Third, the results of heating IV fluid on a stove will vary by technique. Platts-Mills et al measured temperature at the end of infusion tubing and not in the bag itself, so our results are not directly comparable; however, we were surprised that our fluid temperature was 58°C and not close to 40°C, as we were expecting. Any rescue group intending to use this technique needs to experiment with the material that they will really use in the field to be sure that temperatures are appropriate.
Finally, we note in the article by Platts-Mills et al that they measured temperatures at the end of standard infusion tubing in their cold room. An alternative that may avoid temperature drop in the tubing is to use bags of IV fluid that have been bled of all air then placed in a pneumatic pressure infuser. Placed next to the patient under appropriate packaging, a litter patient could receive a continuous infusion with less temperature drop than hanging in the air. Perhaps this should be the next line of investigation.