
Abstract
I report on a case of left main bronchus occlusion by an inhaled foreign body at a remote Antarctic scientific base during the austral winter. The dilemmas of on-site treatment and the challenges of aeromedical evacuation from such a remote environment are presented.
Introduction
Foreign body aspiration is a rare occurrence in neurologically intact adults, and the definitive treatment requires specific training and equipment. When this unexpected event happens in a remote environment, with limited access to health care facilities, proper management may not be straightforward, as demonstrated by this case report.
Case Report
In August 2005 at Rothera Research Station, a United Kingdom (UK) base on the Antarctic Peninsula, a 38-year-old member of the SCUBA dive team was assisting scientists preparing for a dive through sea ice about 500 meters from station. The air temperature was around −30°C (−22°F), which introduced a time pressure in order to avoid the SCUBA dive equipment freezing and becoming unusable. A buoyancy control device (BCD) inflation valve was found to be nonfunctional on checks so the protective cover was removed to investigate. While blowing to melt the small collection of ice around the valve, the diver accidentally inhaled the inflation button (a 1-cm-diameter mushroom-shaped portion of plastic). After an initial choking episode with marked cyanosis but no loss of consciousness, he improved and stabilized. First aid back blows were administered on site by the divers during the choking phase. He was transported via Ski-Doo to the station medical room on demand valve oxygen and arrived approximately 5 minutes after the initial event and was seen immediately by the base doctor.
Clinical findings were consistent with a left main bronchus occlusion. He was stable, with oxygen saturations of 94% at rest on air, pulse 106 beats per minute, blood pressure 196/125 mm Hg, respiratory rate 25 breaths per minute, and no expansion, breath sounds, or vocal resonance on the left side. A chest radiograph during inspiration was normal. His voice was altered, but examination of his pharynx and larynx revealed no abnormalities.
His case was discussed over the telephone with the lead clinician of the British Antarctic Survey Medical Unit (BASMU) in the UK. Bronchoscopy was not a possibility with the equipment on station. The decision was made to attempt noninvasive methods of removal for 24 hours. Physiotherapy, postural drainage, and forced coughing were performed as tolerated (on average 3 minutes every 30 minutes) for 6 hours. The procedure was found to be very uncomfortable by the patient and caused significant distress. He then developed a small amount of subcutaneous emphysema of the face, neck, and upper torso, petechial hemorrhages, and minor periorbital edema. A repeat chest radiograph done at this time was unchanged. The next morning the emphysema was much more prominent so conservative measures were halted. The decision was taken by BASMU to arrange an aeromedical evacuation, which at that time was predicted would take approximately 12 days.
The risks to the patient during the aeromedical evacuation were assessed
1
and actions proposed: Clinically, the left lung contained a trapped air space, which posed the threat of expansion injury to the lung on ascent. There was a reasonable chance, despite no radiological evidence, that there was a small pneumothorax on the left with the possibility that this could tension. There was a third trapped air space of subcutaneous emphysema which with expansion could compromise the airway or circulation. Oxygen saturations were labile, and he was certainly at risk of becoming significantly hypoxic at altitude.
Plans for evacuation ensured enough oxygen to maintain a constant 10 L per minute flow for 5 hours, and a demand valve system available to ration oxygen if a longer flight was necessary. A chest drain was to be inserted on the left side just prior to the flight and large bore intravenous access secured. Emergency equipment to secure an airway was to be on hand during the flight.
From day 1, he was placed on amoxicillin 500 mg 3 times daily for prevention of lower respiratory tract infection. On discussion with the cardiothoracic surgeons in the UK, he was also placed on levofloxacin prophylactically against mediastinitis in light of the subcutaneous emphysema and assumed pneumomediastinum. He remained stable throughout the wait for the evacuation with saturations of 95% at rest on room air, dropping to the mid-80s on any exercise and associated with dizziness, headache, and near fainting. Similarly, pulse and respiratory rate were 100 and 15 per minute at rest, rising to over 150 and 25, respectively, on slow walking. He remained without fever except for borderline temperatures of 37.6°C (99.7°F) on day 2, and 37.3°C (99.1°F) on days 4 and 8. His subcutaneous emphysema began to improve after day 3. Serial chest radiographs showed progressive collapse of the left lower lobe and expansion and air trapping in the left upper lobe (see Figure 1). On 2 occasions during the first 10 days, slight breath sounds could be heard in the left upper zone, although usually there was nothing heard.
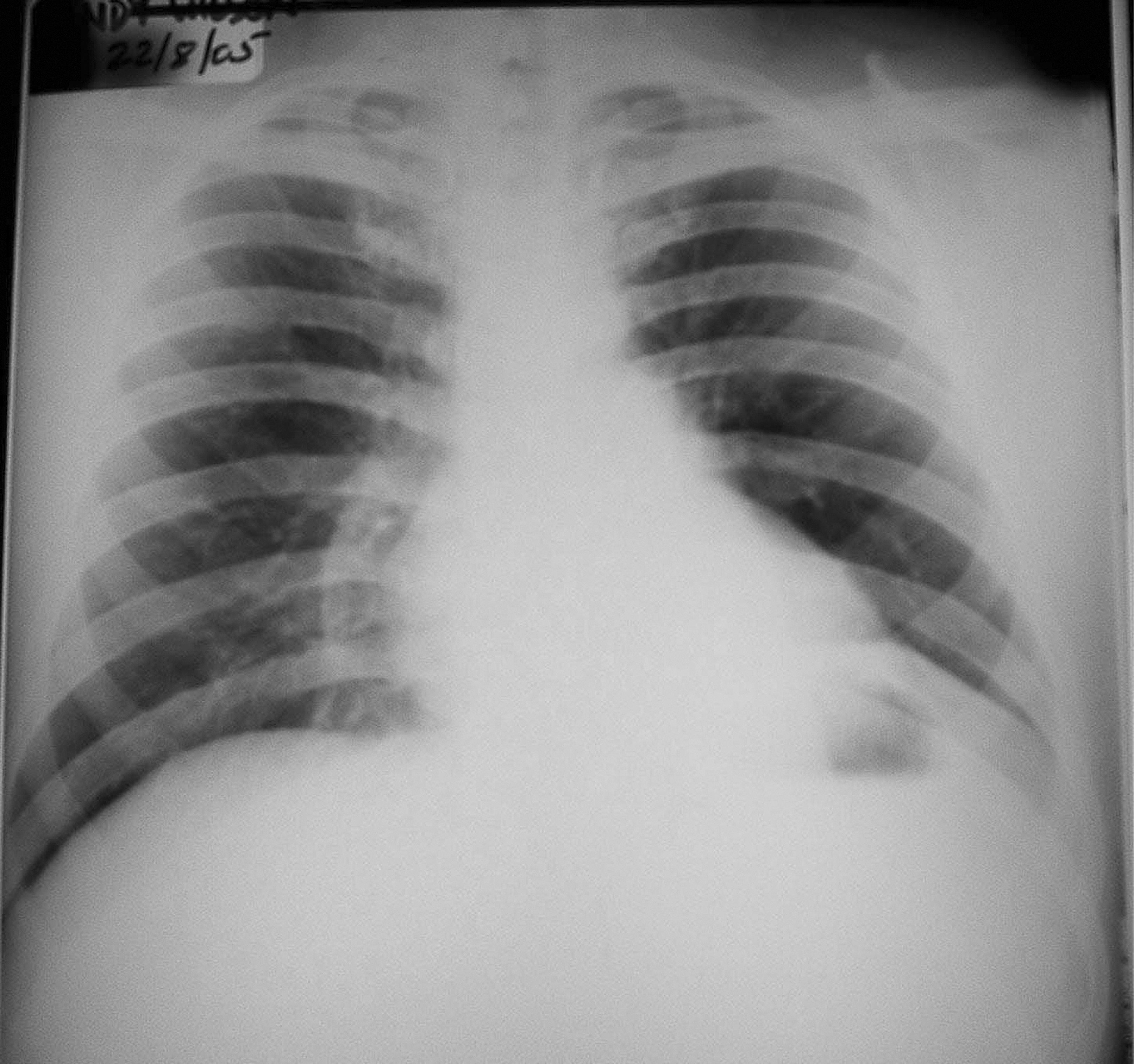
Chest radiograph on day 10 showing collapse of the left lower lobe.
On day 11, he experienced a particularly violent coughing fit and felt something briefly in his throat. Examination immediately following revealed breath sounds and expansion of the left upper zone, but no breath sounds or expansion on the right side of the chest. Oxygen saturations were 90% on air and respiratory rate 25 breaths per minute. After further coughing and expectoration of thick yellow mucus, breath sounds were present in both sides with signs settling to an oxygen saturation of 94% on air and respiratory rate of 15 breaths per minute. Doubt initially still remained as to the whereabouts of the plastic, with the possible diagnoses being either movement of the plastic further down into the left lower lobe bronchus clearing the left upper lobe, or coughing up and then swallowing of the plastic, with dislodged mucus from the left side temporarily blocking the right main bronchus. Twenty-four hours later, however, the plastic object was passed in the stool. At this point, examination revealed a monophonic wheeze in the left upper zone and coarse crepitations in the left lower zone. Oxygen saturations on air, blood pressure, and pulse were still very labile with exercise. A chest radiograph showed the left lower lobe starting to re-expand.
On day 14, he was evacuated to the hospital in Montevideo, Uruguay, by Dash 7 aircraft (see Figure 2), and then to the UK by commercial flight. He was accompanied by a doctor from BASMU. On assessment after the clinical improvement on day 13, it was felt that there was no longer evidence of trapped air in the left upper lobe, repeated radiographs had shown no pneumothorax and there was no clinical evidence of such, and the subcutaneous emphysema was much reduced. The patient, therefore, received supplemental oxygen on ascent and performed the rest of the journey on air with intermittent clinical checks and saturation monitoring. A chest drain was not inserted. The evacuation was uneventful.

The Dash 7 aircraft landing at Rothera Research Station in winter 2005.
Bronchoscopy approximately 1 week after leaving Antarctica was normal (see Figures 3 and 4). He is now completely well and, 3 months after the event, was working back in the Antarctic.
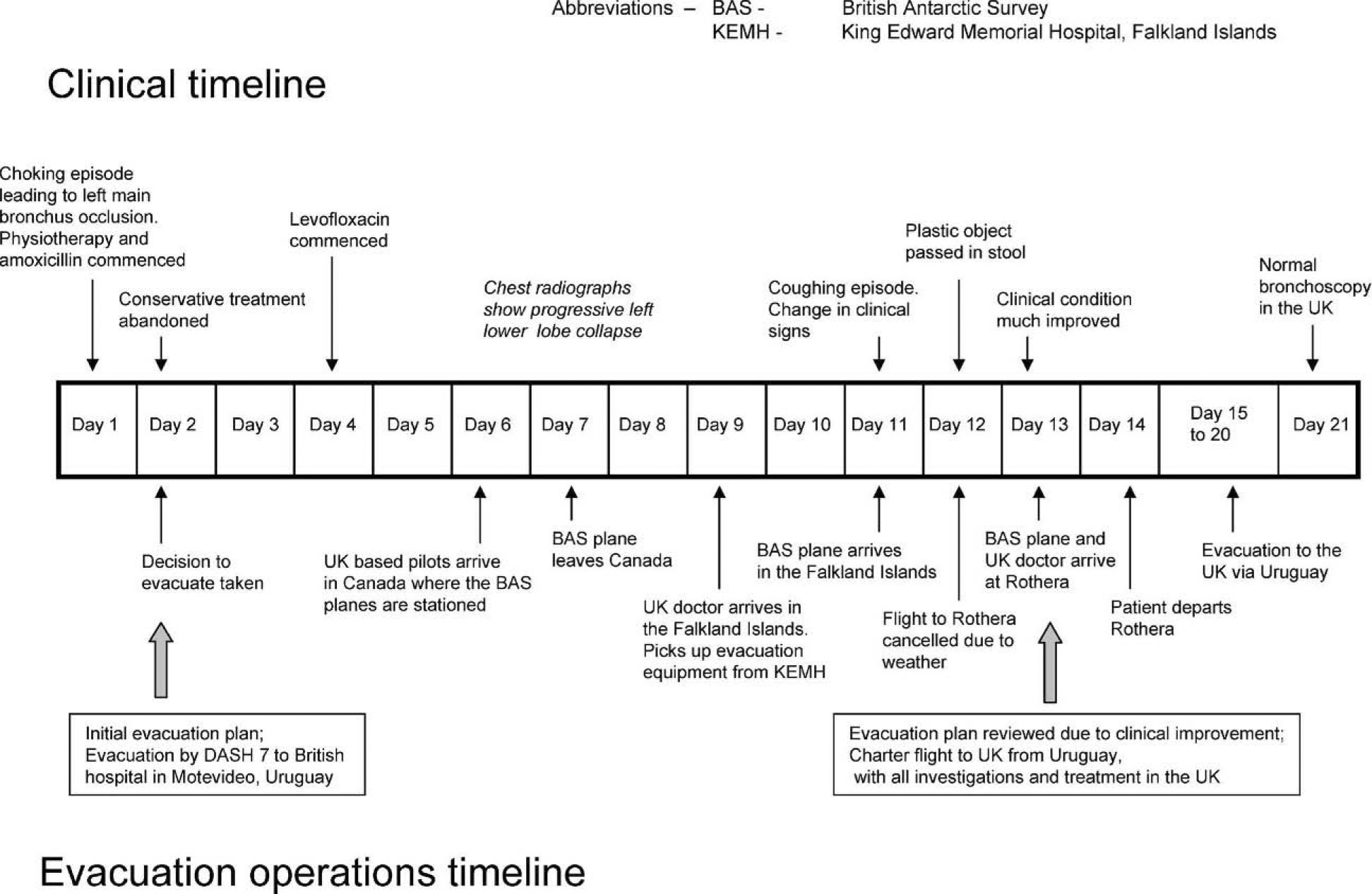
Timeline detailing the clinical course and the evacuation operations.

British Antarctic Survey Stations. Map courtesy of the British Antarctic Survey and reprinted with permission.
Discussion
Antarctica is a remote environment in which to practice medicine. That “remoteness” is greatly influenced by season, station or camp facilities, location, and weather. The British Antarctic Survey (BAS) base has a gravel runway that is used by aircraft. There is a wharf, with usually 2 scheduled visits from BAS ships per season. During the 7 1/2 months of winter the runway is buried in snow, sea ice surrounds the station, and all BAS ships and planes are stationed in the northern hemisphere. There are 21 people on station for that period, including a doctor, and diving continues throughout the winter. Medical facilities include a recompression chamber, a doctors office, and a treatment room with the capacity to support emergency surgery and 1 ventilated patient for a short time.
Although there has been 1 previous unscheduled winter flight at this base to retrieve a dead body, this was the first aeromedical evacuation performed at either of BAS's continental bases during winter, and one of only a handful on the continent as a whole.
The doctor on base is supported by BASMU. The first contact is made to a team of emergency physicians based at Derriford Hospital, Plymouth, UK, and through them referrals can also be made to any hospital specialty and a diving diseases center. Twenty-four-hour telephone links and internet access make the transfer of information, including digital images of radiographs and patients, very easy.
Foreign body aspiration is rare in neurologically intact adults, the vast majority of cases occurring in children below 3 years old.
There is little ambiguity in the literature that bronchoscopy by a practiced operator is the treatment of choice in a case such as this, allowing swift removal of the foreign body in a controlled manner and the simultaneous assessment of any damage to the bronchial tree. 2 –4 Immediate treatment for obstructing foreign bodies with apnea is abdominal thrusts and back blows. 5 Conservative treatments of nonobstructing foreign bodies, such as postural drainage and chest physiotherapy, are discouraged due to the possibility of moving the foreign body to a potentially obstructing location thus making the situation much worse. 6 Although this conservative treatment was carried out in a medical unit equipped with advanced airway aids, anesthetic machine, and ventilator, there is only 1 doctor present in winter, who in this case was not an experienced anesthetist, and any airway obstruction would therefore have been difficult to manage. In a remote setting, the risk benefit ratio will be different. Landing an aircraft in Antarctica can only be done in good weather, and doing this during the winter is undoubtedly a potential risk. Waiting for this “window” of good weather might take several weeks, during which time complications of a foreign body could occur. If the foreign body could be expelled quickly, these risks and complications could be avoided. In published cases, the spontaneous expelling of the foreign body is a rare conclusion (although the true rate of this is hard to study as spontaneous resolution may be much more common in patients who never present to doctors, or who present but don’t reach bronchoscopy, so are not included in the retrospective studies). 7
In our case, the only complication of the conservative management was subcutaneous emphysema presumably from the forced coughing and chest physiotherapy against a blocked airway and escaped alveolar air tracking along the tissue planes. 8 There is a small possibility in this case that a laryngeal or tracheal tear could have been caused by the foreign body leading to the emphysema, especially in light of the altered voice at presentation. The literature states that no specific treatment is needed for subcutaneous emphysema and pneumomediastinum unless life-threatening complications develop (respiratory failure, airway compromise, tension phenomena—in which case the airway is secured and/or the air is evacuated percutaneously as dictated clinically), rather that treatment is aimed at the underlying cause, if appropriate.9,10 Broad spectrum antibiotics are standard management in dental related subcutaneous emphysema and pneumomediastinum because of contamination of the emphysematous spaces by oral flora and potentially colonized dental tubing 11 but is not standard treatment in respiratory tract cases. In a remote environment such as this, however, one can understand the extreme caution and use of prophylactic antibiotics in this respiratory case.
The 3 phases of an aspirated foreign body are: The initial phase of choking, gasping, coughing, and airway obstruction. The “asymptomatic” phase as the object lodges in the airways. There is a reduction or cessation of symptoms for hours to weeks. The complications phase due to erosion or obstruction leading to persistent or recurrent pneumonia, focal bronchiectasis, lung abscess, bronchopulmonary fistula, obstruction following movement of the foreign body, or hemoptysis.
12
In this case, there was a very clear initial choking phase in the history, but many adult cases of aspirated foreign body have a delayed presentation because of this phase being minor and overlooked. Therefore, a high index of suspicion should be maintained as to the possibility of an aspirated foreign body when a well person presents with a minor, short-lived choking history or one sees lung pathology not responding to the usual treatments. Radiographic appearances initially may be subtle such as air trapping (sometimes seen only on the expiratory film), possibly the foreign body itself (however, many are not visible), 13 and atelectasis. Later, the radiographic appearances may reflect the late complications.
The complication rate depends on the site, nature of foreign body (organic or inorganic), and time elapsed before removal. However, it is clear that there is a wide spectrum of clinical presentations, and it is very difficult to predict the outcome for an individual.
The decision to evacuate a patient during winter is unprecedented in BAS history. Previously, the understanding of medical staff and station members alike was that they were effectively physically isolated for the duration of the austral winter as immediately life-threatening cases would be helped little by an evacuation that would take at least 2 weeks, and more minor cases could be treated on site. With this in mind, stations are equipped to perform many surgical and medical procedures and the medical officers trained accordingly. This case had specific factors prompting the consideration of a medical evacuation: There were no effective resources on station to treat the patient (bronchoscope and trained operator were needed). There had already been complications (subcutaneous emphysema and, later, left lower lobe collapse), and if the foreign body remained lodged (as all available evidence indicated it would) further life-threatening complications could be expected within the remaining weeks of winter until normal summer air operations commenced (10 weeks). The patient was stable and had a high chance of remaining stable until evacuation could be attempted.
The evacuation was expensive, but this was a potentially life-saving action, and there was no question of finances halting the operation.
The decision was taken to arrange evacuation early in the course of the event; however, delays were incurred. The pilots resident in the UK had to get to Canada, fly the BAS Dash 7 to the Falklands, then await a break in the weather, which fortuitously happened 2 days after they arrived. Therefore, 13 days approximates to the minimum wait to be expected using that route, but it could be considerably longer if the weather were not favorable. There is a potential that the delay could have been reduced if a plane and pilots had been chartered from South America.
The considerations regarding transport options for medical evacuations are as follows: Pressurized aircraft vs unpressurized. The practical altitude of unpressurized aircraft is 13 000 feet (3962 m) unless oxygen is supplied for the crew. Pressurized aircraft, although flying at higher altitudes, maintain a cabin environment with a theoretical minimum pressure equivalent to an altitude of 8000 feet (2438 m); they therefore have much more versatility in avoiding weather systems. Plane specifications such as engine type, number of engines, and fuel loading capacity. These factors affect range, speed, and safety, for example a 5-hour flight in a 4-propeller plane may take 8 hours in a 2-propeller plane, and both are much safer than a single propeller plane. Wheels only vs dual wheel and ski capability, thereby dictating runway preparation requirements and choice of alternative landing sites. Patient care area. The greater the area the easier it is to perform interventions en route and transport adequate equipment and oxygen.
The fascinating twist to this story is that unexpectedly the patient expelled the foreign body and was clinically much improved by the time the plane had arrived in the Falklands. The need for evacuation was reassessed at that point. It is fair to say that if the planes had not got that far the evacuation would not have been performed, but they had, and the patient still had significant changes on his chest radiograph, the continuous broad spectrum antibiotic use could have masked latent infection, and there was a potential undiagnosed laryngeal/tracheal injury. The recommendation of BASMU was still to evacuate, although he was now well enough to be brought straight back to the UK for investigation. The urgency of the operation had also changed and marginal weather conditions were now not acceptable. The argument that 4 more lives were put at risk (the crew of the aircraft and the UK doctor) and the evacuation should not have been attempted is an important one. This would have been much more of an issue if the patient's condition was such that hours and days would affect outcome, causing the pilots to feel personal and institutional pressure to fly in marginal conditions. However, in this case the pilots were able to wait until the weather conditions were good, and the flight to Rothera posed a similar risk to Antarctic flights in the summer months.
Conclusion
Although BAS has now performed a successful medical evacuation during winter from one of its continental stations, this was a very specific clinical situation. The practice of remote medicine during the austral winter, and the preparation and training this requires, still remain. What this case shows however is that medical evacuations in winter are a possibility, and should open the debate among the Antarctic community about when they are appropriate and how best to perform them.
Footnotes
Acknowledgments
For Dr Henry R Guly, MBBS, FRCP, FFAEM, Derriford Hospital, Plymouth, UK; Dr Fionn Bellis, MA, MBBS, MRCS, Dipl SEM, Truro Hospital, Truro, UK; and Mr Iain Grant, MB, FRCSEd, FFAEM, Derriford Hospital, Plymouth, UK: The author would like to thank Mr Grant and Dr Guly for their medical advice and support during the period of the evacuation, and Dr Bellis for flying into the Antarctic winter to transport the patient home. I would like to thank all 3 for their comments on this manuscript and their support.