
Abstract
Cortactin and fascin-1 are important factors in tumor progression. We tested the hypothesis that cortactin and fascin-1 expression correlates with clinicopathological parameters of gastric adenocarcinoma. Immunohistochemical analysis of cortactin and fascin-1 was done using tissue microarrays of 100 surgical specimens, including 20 well-differentiated, 20 moderately differentiated, and 60 poorly differentiated gastric adenocarcinomas. Among the 20 well-differentiated gastric adenocarcinomas, 15 cases (75%) showed negative or weak staining (1+); 5 cases (25%) had moderate (2+) or strong (3+) cortactin expression. Among the 60 poorly differentiated gastric adenocarcinomas, more than three-quarters of the cases (76.7%) had moderate or strong cortactin expression; 14 cases (23.3%) had weak staining. Of 20 well-differentiated gastric adenocarcinoma cases, 14 (70%) showed negative or weak staining of fascin-1, whereas nearly one-third (30%) had moderate or strong expression. Among the 60 poorly differentiated gastric adenocarcinomas, 32 (53.3%) exhibited moderate or strong fascin-1 expression; fewer than half of the cases showed negative or weak staining. Higher intensity of cortactin and fascin-1 staining correlated directly with more-advanced cancer stages (TNM) and inversely with survival rates. Our findings suggest the possibility that pharmacological inhibitors of cortactin and fascin-1 activity may slow down tumor progression and prolong survival time in patients with gastric adenocarcinomas.
G
Recent studies indicate that enhancement of cell motility and loss of cell-cell adhesion is essential to tumor progression (Matsudaira 1994; Otto 1994; Tilney et al. 1998). Cortactin and fascin-1 are two important components among these actin cross-linking proteins (Hashimoto et al. 2005; Luo et al. 2006). Identification of mechanisms promoting tumor cell invasion may help direct creation of new therapies that can arrest local invasion and metastatic spread of gastric adenocarcinoma.
Cortactin is an actin-binding protein that activates the Arp2/3 complex to regulate the actin cytoskeleton (Daly 2004; van Rossum et al. 2006) and inhibit debranching of dendritic actin networks (Weaver et al. 2001). The gene responsible for cortactin expression is in the chromosome 11q13 region and is frequently amplified in some human cancers, such as breast and head/neck carcinomas (Schuuring 1995; Ormandy et al. 2003). Remodeling of the actin cytoskeleton has effects on cell migration, motility, and adhesion, as well as on tumor invasion and metastasis (van Rossum et al. 2006). In some studies, the amplification of 11q13 and overexpression of cortactin correlate with poor prognosis for patients with lymph node metastasis (Schuuring et al. 1992; Schuuring 1995; Ormandy et al. 2003). However, the relationship between cortactin expression and clinicopathological parameters of gastric adenocarcinoma remains vague.
Fascin, an actin-binding protein, is involved in the rearrangement of the cytoskeleton and promotes cellular motility (Roma and Prayson 2005). Fascin-actin interactions are regulated by the extracellular matrix, peptide factors, and other actin-binding proteins (Adams 2004a). In the human body, the genome encodes three subtypes of the fascin family, including fascin-1, fascin-2, and fascin-3 (Hashimoto et al. 2005). The level of fascin is low or undetectable in normal epithelial cells (Tong et al. 2005). Fascin overexpression has been reported to be associated with several different types of tumors, including breast, colon, brain, esophagus, stomach, lung, urinary bladder, and even hematological malignancies (Grothey et al. 2000; Fan et al. 2003; Pelosi et al. 2003; Hashimoto et al. 2004; Hashimoto et al. 2005; Roma and Prayson 2005; Xie et al. 2005).
In this study, we tested the hypothesis that higher expression of cortactin and fascin-1 in gastric adenocarcinoma patients correlates with clinicopathological parameters associated with advanced cancer stages and with decreased survival rates. The hypothesis that we set out to test is that increased cortactin and fascin-1 immunostaining intensities correlate with advanced histological grades, advanced clinical stages, and poorer prognosis for gastric adenocarcinoma patients.
Materials and Methods
Paraffin-embedded tumor tissues were obtained and tissue microarray slides were constructed. The tissue microarray included samples from 100 patients with gastric adenocarcinoma, including 20 well-differentiated cases (>95% showing glandular structure), 20 moderately differentiated cases (glandular structure seen in 50-95%), and 60 poorly differentiated adenocarcinomas (glandular structure in <50%). The pathological diagnosis of these cases was reviewed by at least two experienced pathologists. The histopathological differentiation of gastric adenocarcinoma was determined according to World Health Organization criteria for tumor classification (Hemilton and Aaltonen 2000). These 100 gastric adenocarcinoma patients comprised 58 males and 42 females. Age distribution ranged from 33 to 89 years; the mean was 66.7. Other information, including histopathological differentiation and staging distribution, is listed in Table 1. All experiments were approved by a human tissue committee.
One core tissue sample was taken from a selected area of each paraffin-embedded tumor tissue, and tissue microarray slides were constructed. Each representative core sample in the tissue microarray slide was 2 mm in diameter. The pathological diagnosis in each case was reviewed by at least two experienced pathologists. No cases had received radiation or chemotherapy before surgery.
Clinicopathologic characteristics of 100 patients with gastric adenocarcinoma
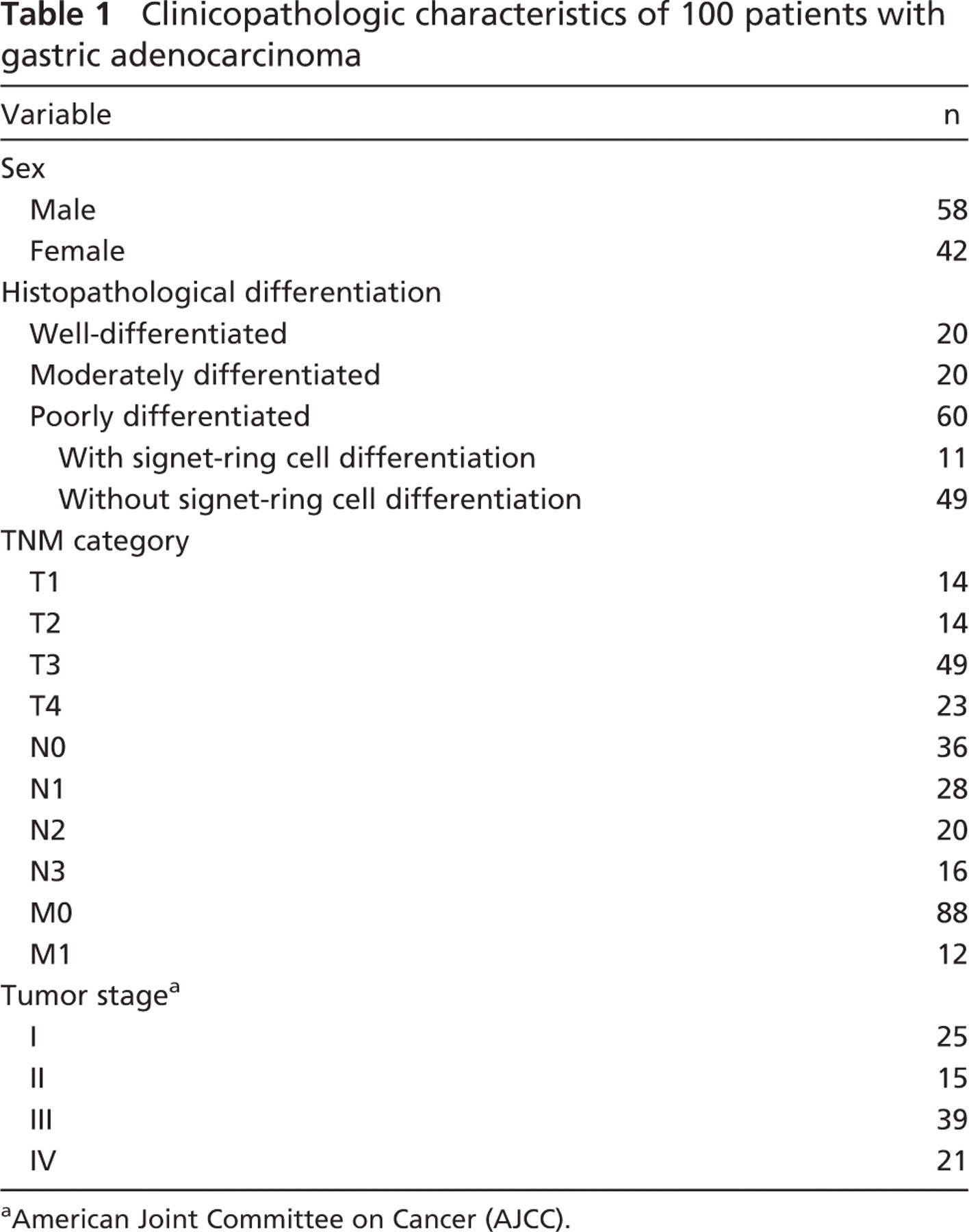
American Joint Committee on Cancer (AJCC).
Immunohistochemistry
Tissue microarray sections were dewaxed in xylene, rehydrated in alcohol, and immersed in 3% hydrogen peroxide for 5 min to suppress endogenous peroxidase activity. Antigen retrieval was performed by heating (at 100C) each section for 30 min in 0.01 mol/l sodium citrate buffer (pH 6.0). After three rinses [each for 5 min in phosphate-buffered saline (PBS)], sections were incubated for 1 hr at room temperature with a polyclonal goat anti-rabbit cortactin antibody (1:100; Santa Cruz Biotechnology, Santa Cruz, CA) and a monoclonal mouse anti-human fascin-1 antibody (1:100; NeoMarkers, Fremont, CA), both diluted in PBS. After three washes (each for 5 min in PBS), sections were incubated with biotin-labeled secondary immunoglobulin (1:100; DAKO, Glostrup, Denmark) for 1 hr at room temperature. After three additional washes, peroxidase activity was developed with AEC+ substrate chromogen (DAKO) at room temperature.
For assessment of cortactin and fascin-1 immunoexpression, we modified the immunoscoring of two published experiments about fascin-1 overexpression in gastric and brain tumors (Hashimoto et al. 2004; Roma and Prayson 2005). The intensities of cytoplasmic and membranous immunostaining were rated on a scale with scores shown as 0 (negative staining for tumor cells), 1+ (positive staining for 5-25% tumor cells), 2+ (positive staining for 26-50% tumor cells), and 3+ (positive staining for more than 50% tumor cells). For these biomarker analyses, tumors with <5% of cells showing cytoplasmic and membranous immunoexpression were considered to be negative for the biomarker.
Statistical Analysis
The immunostaining intensities of cortactin and fascin-1 in gastric adenocarcinomas were compared with normal esophageal squamous epithelium that had been shown to have negative staining for these biomarkers (Luo et al. 2006). Statistical analysis was performed using the Pearson Product Method Correlation test to analyze the relationships between the expression of these two biomarkers and clinicopathological parameters in gastric adenocarcinoma patients.
In addition, survival time was calculated from patients' date of surgery to date of death. Seventy-five gastric adenocarcinoma cases were followed up for 3 years. Cases that were included in survival analysis were divided into four groups reflecting the four possible staining scores, 0, 1, 2, or 3 to allow comparison of survival time with cortactin and fascin-1 immunostaining intensities. Statistical analysis of survival time was done using the Kaplan-Meier survival test.
Results
Immunostaining of Cortactin Correlates With Histological Grades and Clinical Stages of Gastric Adenocarcinomas
Among 20 cases with well-differentiated gastric adenocarcinoma, 4 cases (20%) showed negative staining, 11 cases (55%) presented weak positive staining (1+), 2 cases (10%) revealed moderate staining, and 3 cases (15%) exhibited strong staining of cortactin. Among the 20 cases with moderately differentiated and 60 cases with poorly differentiated gastric adenocarcinomas, no case showed negative staining for cortactin, 4 (20%) and 14 (23.3%) cases presented weak staining, 7 (35%) and 27 (45%) cases revealed moderate staining, and 9 (45%) and 19 (31.7%) cases exhibited strong expression of cortactin, respectively. Using the Pearson Product Method Correlation test, overexpression of cortactin showed a positive correlation with histological grading of gastric adenocarcinomas (p<0.05; Figure 1; Table 2). Negative (0) or weak staining (1+) for cortactin was seen in 9 of 14 cases (64.3%) in T1 stage, in 6 of 14 cases (42.8%) in T2 stage, in 15 of 49 cases (30.7%) in T3 stage, and in 3 of 23 cases (13.1%) in T4 stage. In contrast, moderate (2+) or strong (3+) staining for cortactin was seen in 5 of 14 cases (35.7%) in T1 stage, 8 of 14 cases (57.2%) in T2 stage, 34 of 49 cases (69.4%) in T3 stage, and 20 of 23 cases (86%) in T4 stage. Advanced T stage correlated significantly with higher cortactin immunostaining intensity (p<0.05). Similarly, 15 of 25 cases (60%) in stage 1 had negative (0) or weak staining (1+), but more than half of the cases in stages 2, 3, and 4 showed moderate (2+) to strong (3+) staining for cortactin. Higher immunostaining intensity for cortactin also correlated significantly with advanced clinical stages (p<0.05; Figure 2; Table 2).
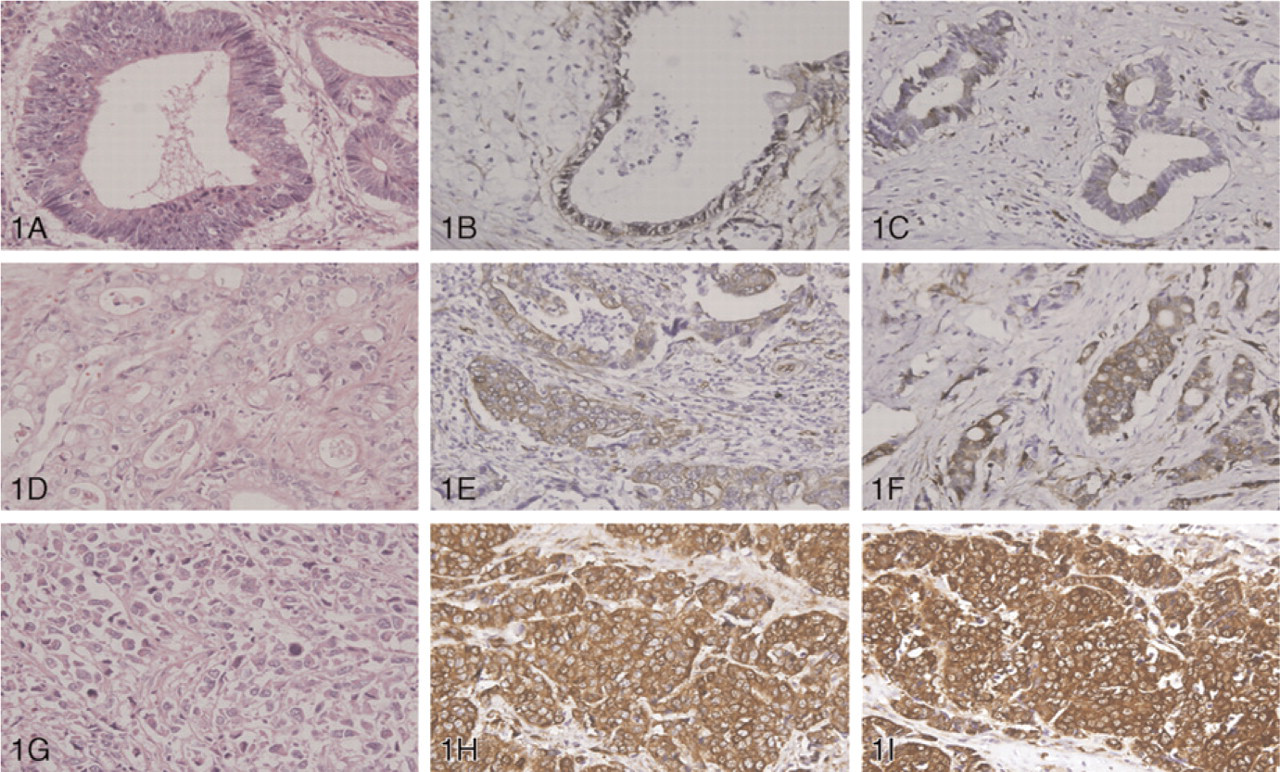
Hematoxylin and eosin staining of well-differentiated (
Immunostaining of Fascin-1 Correlates With Histological Grades and Clinical Stages of Gastric Adenocarcinomas
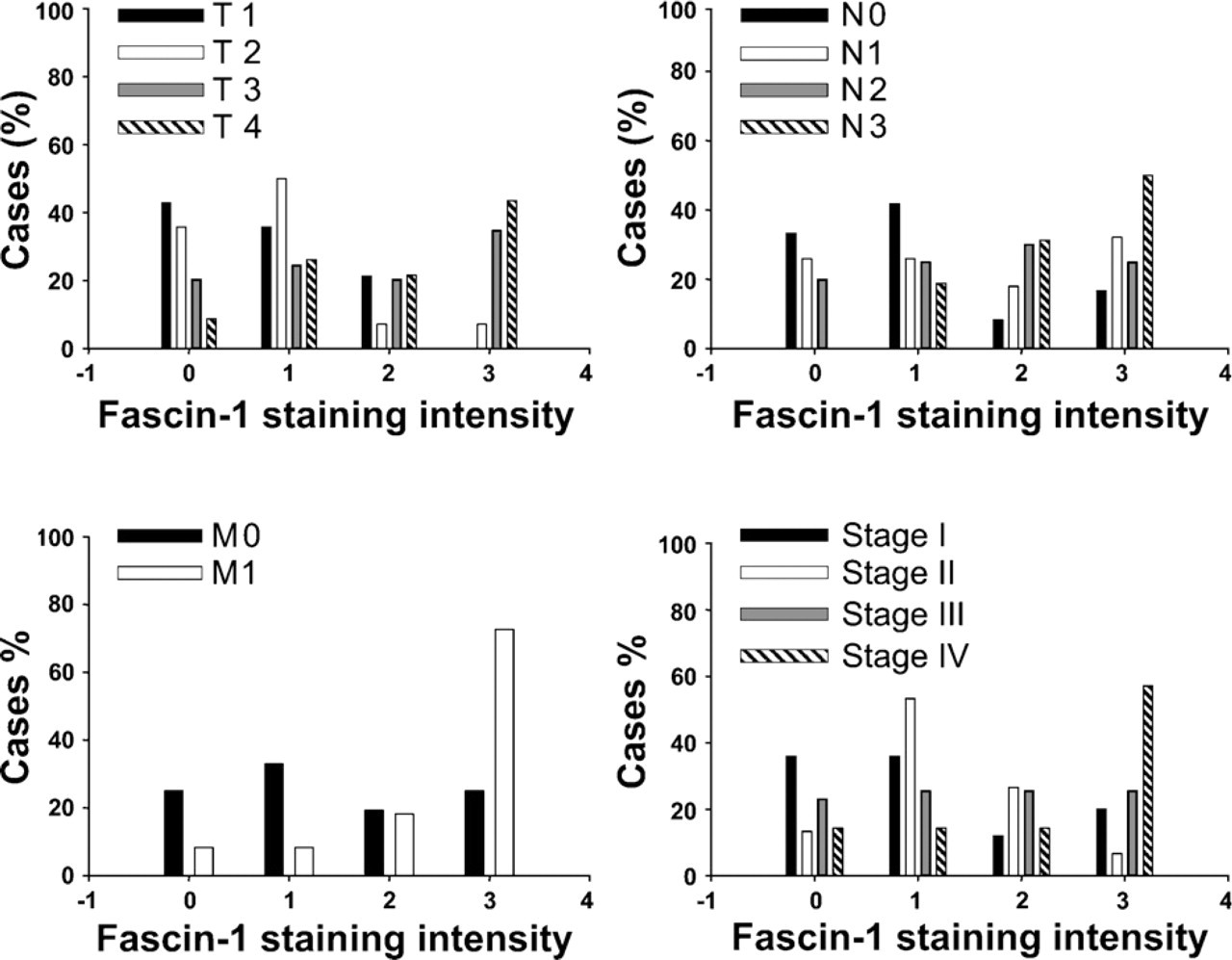
Among the 100 gastric adenocarcinomas, negative (0) or weak (1+) staining was seen in 14 of 20 well-differentiated cases (70%), 11 of 20 moderately differentiated cases (55%), and 28 of 60 poorly differentiated cases (46.7%). In contrast, the percentage of cases showing moderate to strong expression of fascin-1 in well-differentiated gastric adenocarcinomas was lower than the percentage in moderately or poorly differentiated tumors. Statistical analysis showed a positive correlation of fascin-1 immunostaining intensity with histological grading (p<0.05; Figure 1; Table 3). In addition, the percentage of cases in T1 (78.6%) and T2 (85.7%) stages of gastric adenocarcinoma showing negative or weak staining of fascin-1 were higher than the percentage of cases in T3 (44.9%) and T4 (34.8%) stages. T stages correlated significantly with higher fascin-1 immunostaining intensity (p<0.05; Figure 3; Table 3). Similarly, 18 of 25 cases (72%) with stage 1 and 10 of 15 cases (66.6%) with stage 2 had negative (0) or weak (1+) staining, but more than half of stage 3 (51.2%) and stage 4 (71.5%) cases showed moderate (2+) to strong (3+) staining for fascin-1. Higher immunostaining intensity for fascin-1 also correlated significantly with advanced clinical stages (p<0.05; Table 3). Similarly, the more-advanced N stage also had higher immunostaining intensity (p<0.05; Figure 3; Table 3).
The intensity of cortactin immunostaining and clinicopatholigcal parameters of gastric adenocarcinoma
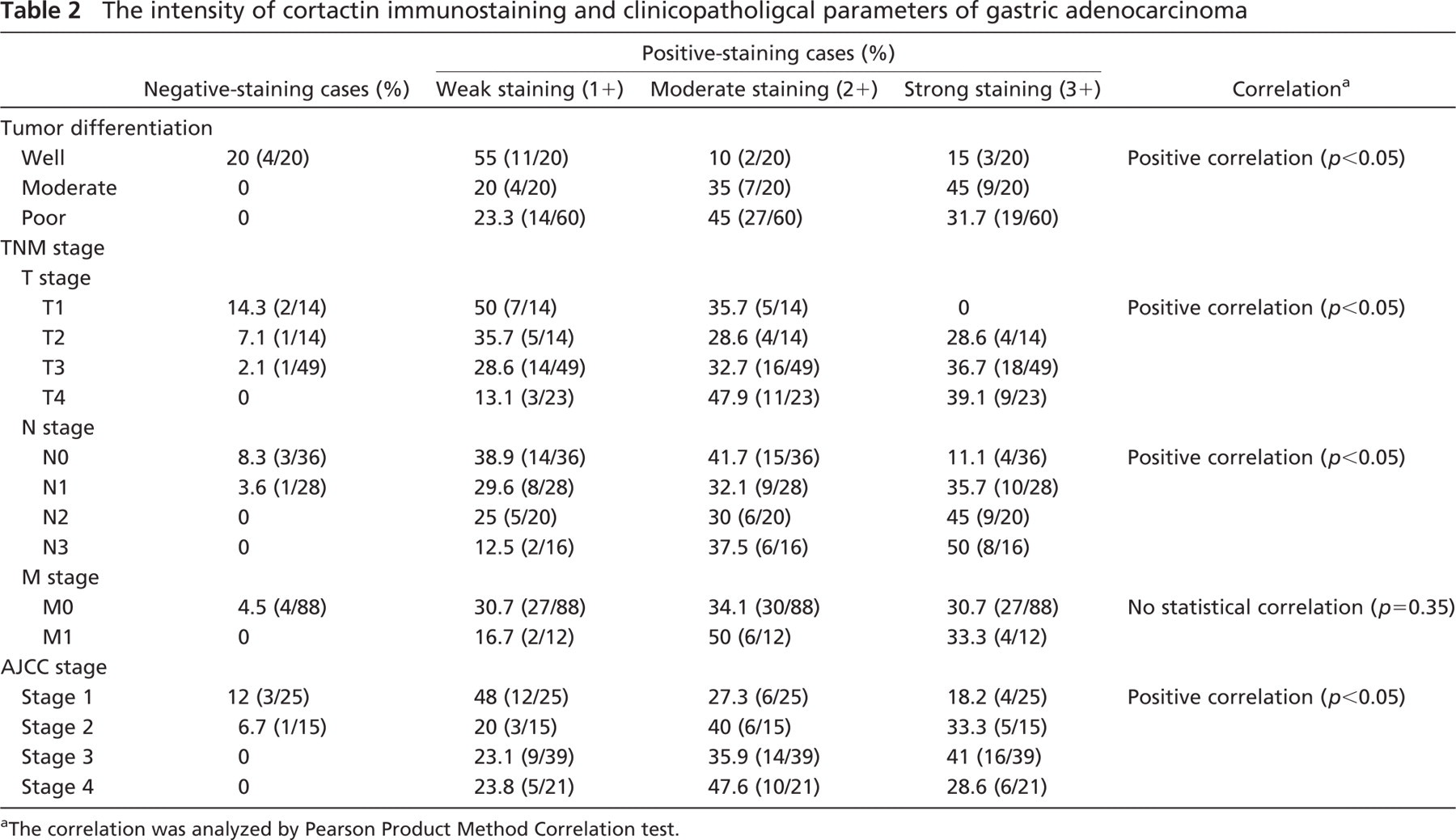
The correlation was analyzed by Pearson Product Method Correlation test.
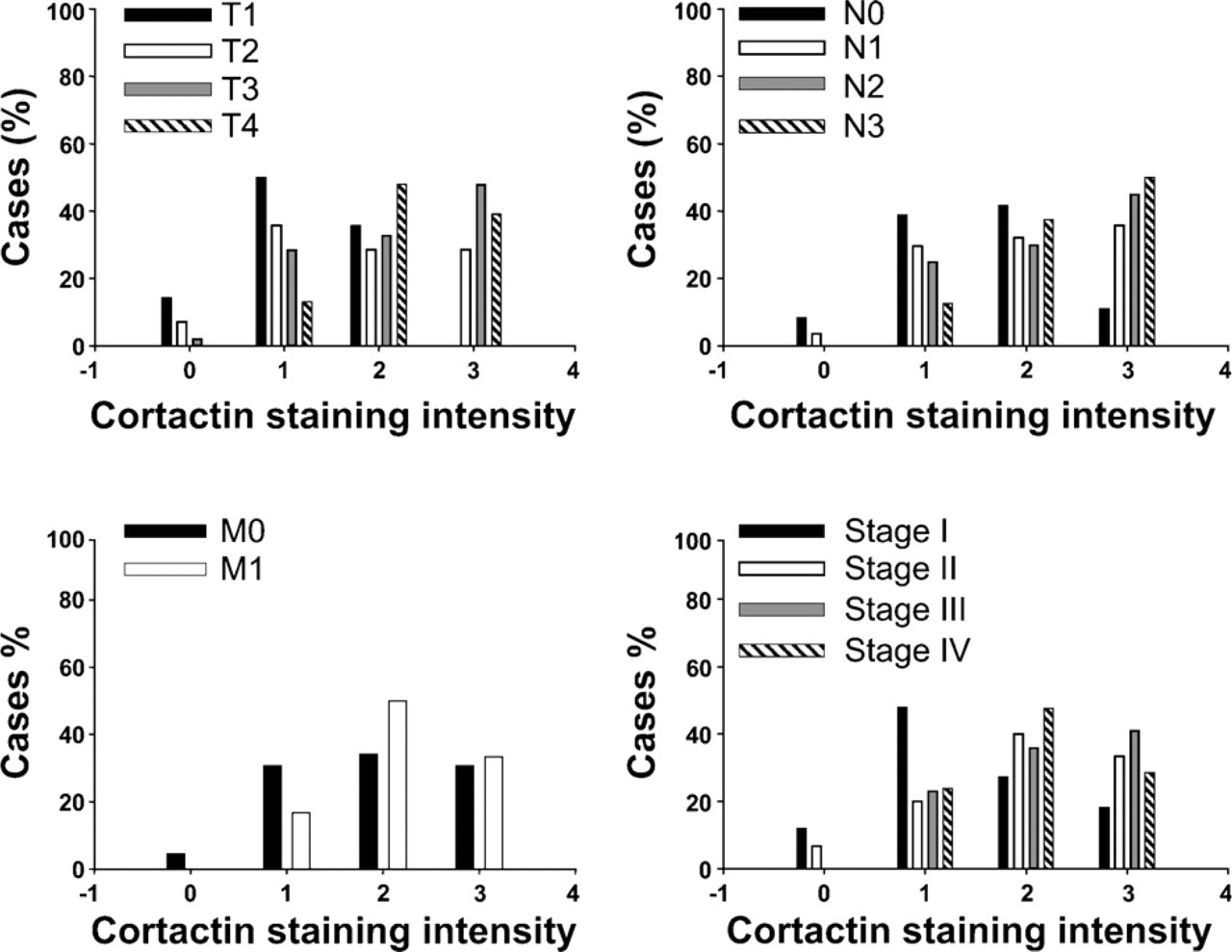
Correlation between clinicopathological data and cortactin immunostaining intensity in gastric adenocarcinoma.
The intensity of fascin-1 immunostaining and clinicopatholigcal parameters of gastric adenocarcinoma
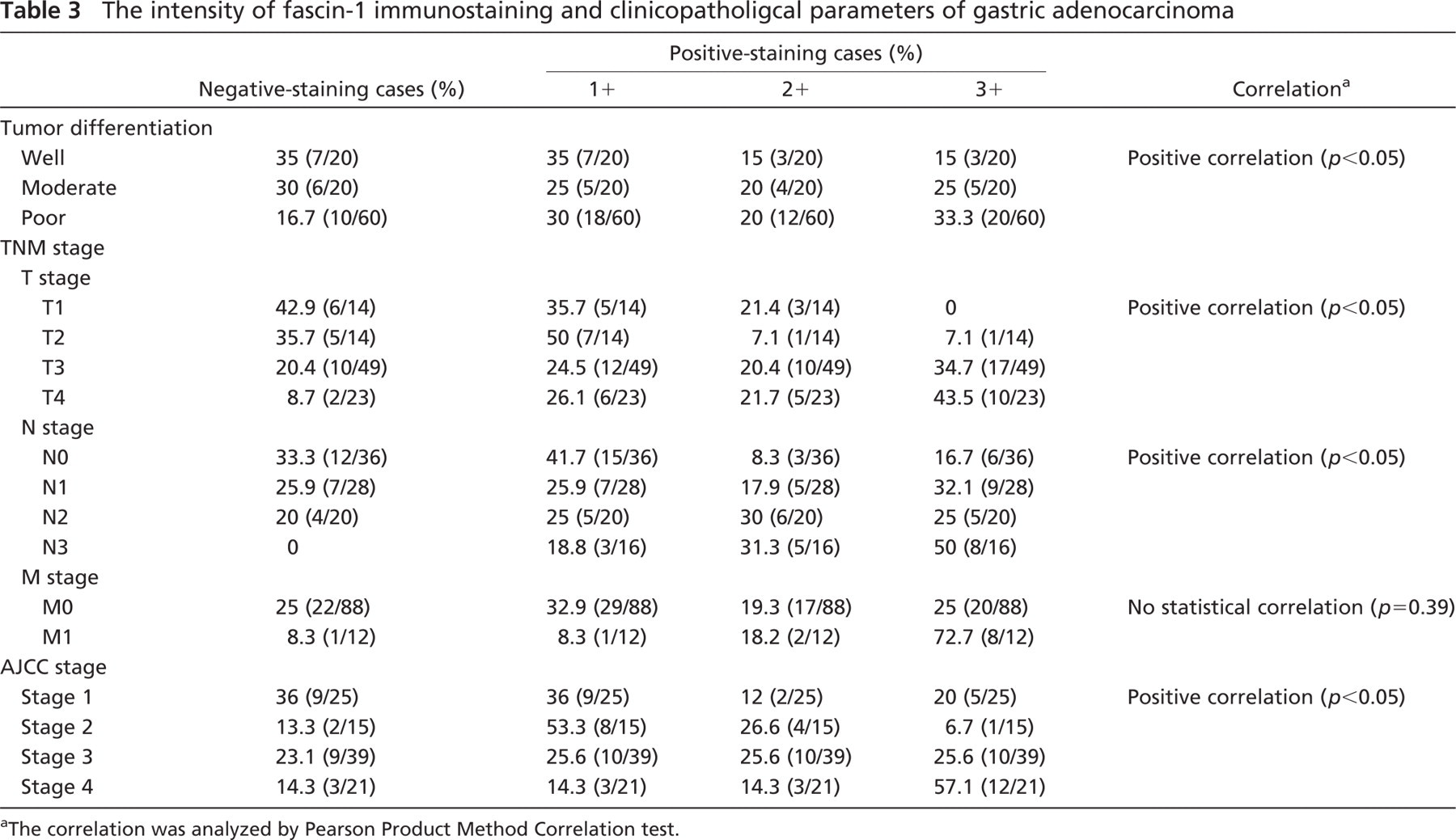
The correlation was analyzed by Pearson Product Method Correlation test.
Correlation between clinicopathological data and fascin-1 immunostaining intensity in gastric adenocarcinoma.
Relationship Between Immunostaining for Cortactin and Fascin-1 and Survival Time
The 75 gastric adenocarcinoma cases receiving 3-year follow-up were divided into four groups based on the immunostaining intensities of cortactin and fascin-1. Using cortactin and fascin-1 immunostaining intensities as independent variables, higher intensities for these biomarkers were associated with a poorer prognosis (Figures 4 and 5).
Discussion
Gastric adenocarcinoma is one of the most prevalent cancers worldwide, and clinical management leads to mostly unsatisfactory outcomes. Partial or total gastrectomy is the curative treatment, but tumor recurrence or metastasis often causes treatment to fail. Gastric adenocarcinoma spreads by direct tumor invasion, metastasis, and peritoneal dissemination (Hemilton and Aaltonen 2000). Some precursor lesions of gastric adenocarcinoma have been identified, such as atrophic gastritis, intestinal metaplasia, adenoma, polyp, and intraepithelial neoplasia (Hemilton and Aaltonen 2000). In recent studies, abnormal expression of the cell adhesion protein E-cadherin led to tumor progression of gastric adenocarcinoma (Gayther et al. 1998; Guilford et al. 1999). The prognosis for patients with gastric adenocarcinoma depends on the depth of tumor invasion and American Joint Committee on Cancer (AJCC) staging system (Hemilton and Aaltonen 2000).
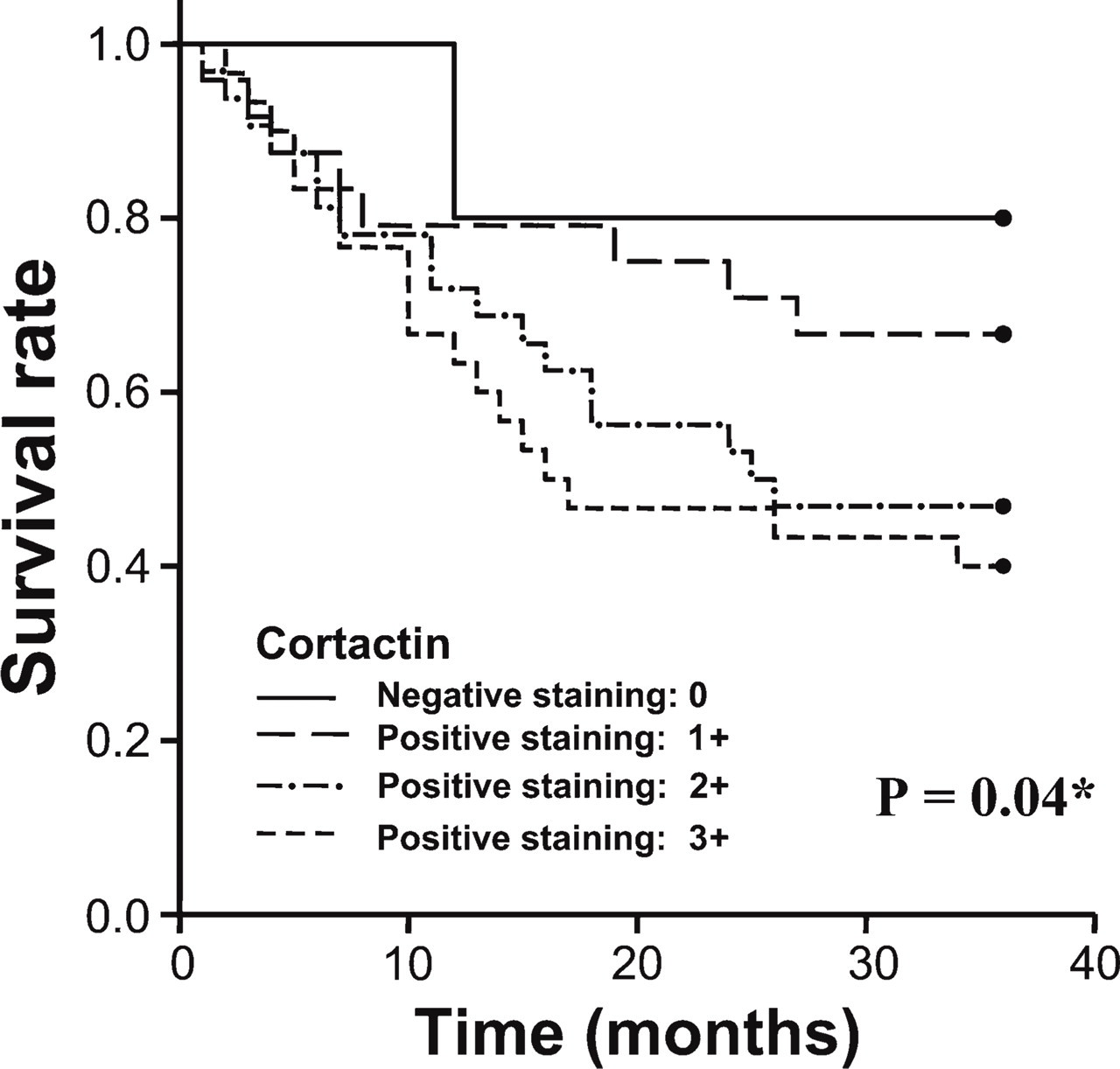
Overall survival of 75 patients with gastric adenocarcinoma. Higher cortactin immunostaining intensities were associated with worse survival. Survival rates were analyzed using the Kaplan-Meier survival test (∗ p<0.05).
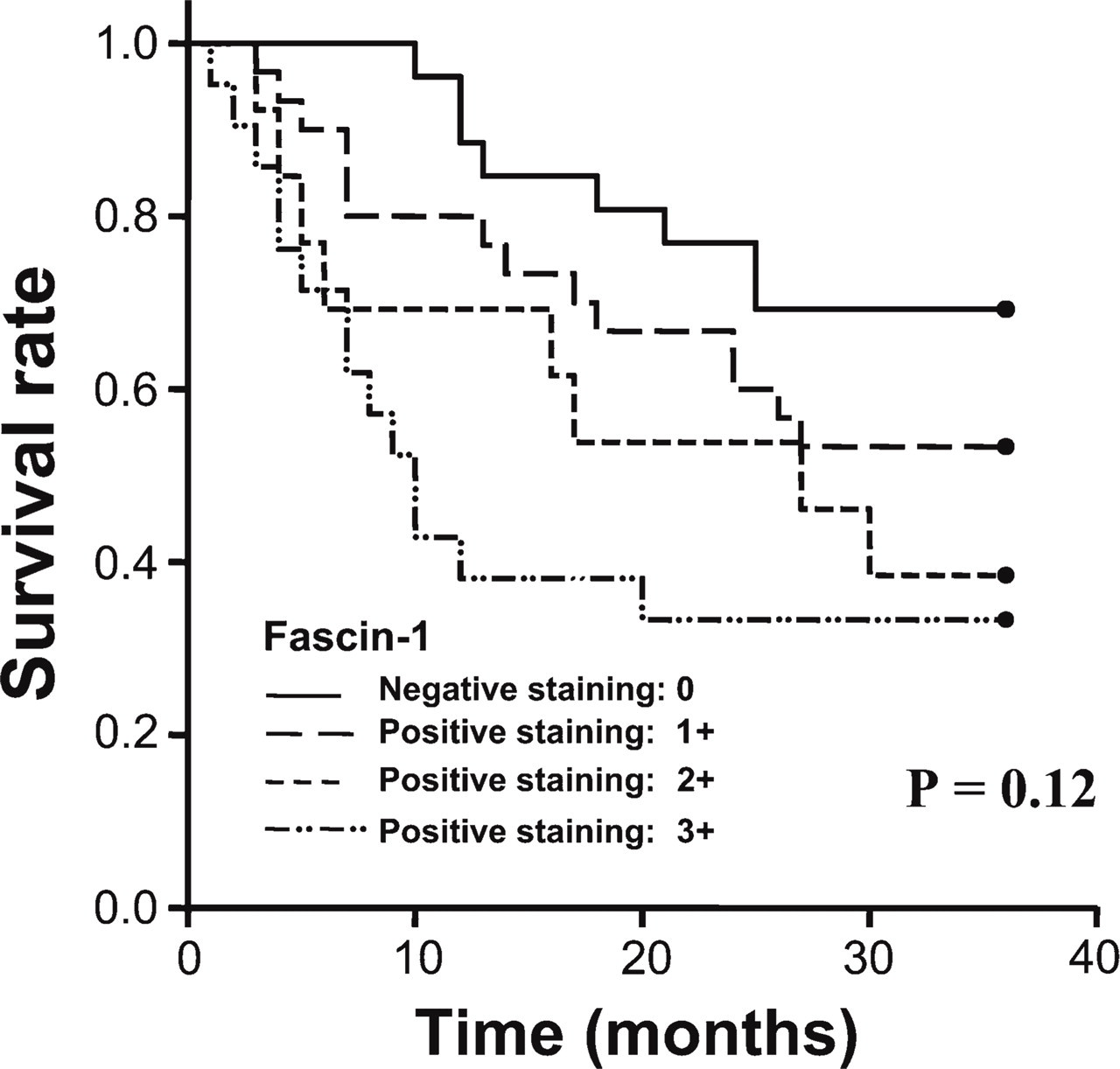
Overall survival of 75 patients with gastric adenocarcinoma. Higher fascin-1 immunostaining intensities were associated with worse survival, but did not reach statistical significance. Survival rates were analyzed using the Kaplan-Meier survival test (p>0.05).
Cortactin regulates the actin cytoskeleton through its involvement in several processes, including cell motility, adhesion, polarization, contraction, and others (Weed and Parsons 2001; Daly 2004; van Rossum et al. 2005a). The activation of actin-related (Arp) 2/3 protein complex and neuronal Wiscott-Aldrich Syndrome protein (N-Wasp) by cortactin nucleates actin polymerization and promotes cellular motility (Greer et al. in press). Cortactin is a p80/p85 multidomain actin filament-binding protein (Schuuring et al. 1993) and was first identified as an src kinase substrate in chicken fibroblasts (Wu et al. 1991). Human cortactin maps to chromosome 11q13 (Luo et al. 2006). The amplification of chromosome 11q13 has been reported in several human carcinomas as has increased expression of cortactin (van Rossum et al. 2005b). Overexpression of cortactin induces cell motility and migration, inhibits cell-cell adhesion, and accelerates tumor spreading (van Rossum et al. 2006). In addition, the effect of cortactin may be related to the expression of E-cadherin and its effects on intercellular adhesion (Kovacs et al. 2002; Helwani et al. 2004; Verma et al. 2004). In some in vitro studies, cortactin overexpression induced tumor invasion, and metastasis has been shownto be associated with esophageal and head/neck squamous cell carcinomas (Luo et al. 2006; Rothschild et al. 2006). However, direct evidence is still lacking to establish a relationship between cortactin overexpression and tumor progression and metastasis in gastric adenocarcinoma.
Fascin-1, a 55-kDa globular protein, aggregates F actin into parallel bundles to rearrange the cytoskeleton and promote cellular motility (Kureishy et al. 2002; Adams 2004a). It plays important roles in cellular protrusion and migration, and extracellular matrix adhesion (Adams 2004b). The gene encoding fascin-1 in humans is located at chromosome 7q22 (Hashimoto et al. 2005). Fascin-1 expression in normal gastric epithelia was shown to be undetectable (Pelosi et al. 2003). Overexpression of fascin-1 is associated with tumor progression and invasion in lung, gastric, esophageal, and breast carcinomas (Grothey et al. 2000; Hu et al. 2000; Fan et al. 2003; Jawhari et al. 2003; Pelosi et al. 2003). Our results suggest that the expression of fascin-1 may be effective in predicting tumor clinicopathological parameters of gastric adenocarcinoma in Chinese patients.
Average immunostaining intensity for cortactin and fascin has a significant positive correlation with T, N, and AJCC stages, but not with M stage. However, in our results, a greater percentage of M1 stage cases had stronger immunostaining intensity for these biomarkers than did the M0 stage. The fact that gastric adenocarcinoma cases in the M0 stage outnumbered those in M1-stage cases may have made it difficult to show statistical significance.
Until now, direct evidence has been lacking to establish a relationship between cortactin overexpression and survival rate in gastric adenocarcinoma. In our study, we successfully demonstrated that cortactin immunostaining intensity correlates with clinicopathological parameters and prognosis in gastric adenocarcinoma patients. To our knowledge, this is the first report to evaluate the association between cortactin expression and tumor progression in gastric adenocarcinoma patients. Similarly, greater immunostaining intensity of fascin-1 also correlated with higher histological grading, AJCC staging, and poorer prognosis in Chinese patients with gastric adenocarcinoma. The expression of fascin-1 in gastric adenocarcinoma in Chinese patients was similar to that in the results of a previous Japanese study (Hashimoto et al. 2004). Our results support the hypothesis that these two biomarkers are important prognostic factors for gastric adenocarcinoma.
In conclusion, higher cortactin and fascin immunostaining intensities in gastric adenocarcinoma tumor tissues are associated with shorter survival time and more-advanced TNM stages. Although multiple factors contribute to tumor progression, we show that cortactin and fascin-1 are satisfactory biomarkers for predicting clinical outcomes in gastric adenocarcinoma. Moreover, there is the possibility that development of pharmacological agents that inhibit cortactin and fascin-1 pathways may prolong survival time and arrest tumor progression in gastric adenocarcinoma patients.
Footnotes
Acknowledgements
This study was supported by grants from the National Science Council (NSC95-2320-B-016-024) and Tri-Service General Hospital (TSGH-C96-14-S01 and TSGH-C96-90), Taiwan, R. O. C.