
Abstract
The use of immunohistochemistry (IHC) in staging bone marrow in non-Hodgkin's lymphoma (NHL) is largely limited to ambiguous cases, particularly those with lymphoid aggregates. Its role in routine clinical practice remains unestablished. This study aimed to determine whether the routine use of IHC in diffuse large B-cell lymphoma (DLBCL) would improve the detection of lymphomatous involvement in the bone marrow. It also sought to determine the impact of IHC on predicting survival compared with routine histological diagnosis using hematoxylin and eosin (H&E), Giemsa, and reticulin staining. The bone marrow trephines of 156 histologically proven DLBCL cases were assessed on routine histology, and IHC using two T-cell markers (CD45RO and CD3), two B-cell markers (CD20 and CD79a), and κ and λ light chains. IHC detected lymphomatous involvement on an additional 11% cases compared with histology alone. Although both routine histology and IHC were good predictors of survival, IHC was better at predicting survival on stepwise multivariate Cox regression analysis. IHC performed routinely on bone marrow trephines has the ability to improve detection of occult lymphoma in experienced hands. Furthermore, it is a better predictor of survival compared with routine histological examination alone.
Keywords
I
Reported rates of BM involvement in NHL differ based on the subtype of NHL, with low-grade lymphomas having much higher rates of involvement (Harris et al. 1999). The reported rates of BM involvement in diffuse large B-cell lymphoma (DLBCL) vary from 12% to 35% (Conlan et al. 1990; Campbell et al. 2003). Patterns of infiltration vary from subtle focal infiltrates to almost complete effacement by lymphoma cells (Harris et al. 1999). Histological discordance with the presence of large cells in primary tissue and predominantly small cells in the BM is known in DLBCL, with reported rates of ∼50∼70% (Conlan et al. 1990; Campbell et al. 2006; Chung et al. 2007).
The implications of BM involvement also vary depending on the grade of lymphoma. Marrow involvement in DLBCL has implications for prognosis; lymphomatous infiltration in the marrow has been reported to correlate with poor survival (Yan et al. 1995; Campbell et al. 2006). Furthermore, marrow involvement in DLBCL affects the International Prognostic Index (IPI) both by increasing the stage of the disease to stage IV and by being assessed as extranodal involve ment (Shipp et al. 1993). Treatment of high-grade lymphomas, in many centers, may vary depending on the stage of the disease or the IPI.
The role of IHC in staging BM has been upstaged, to some extent, by immunophenotyping by flow cytometry of BM aspirates. This is perhaps because the results obtained with flow cytometry are quantitative and perceived to be less prone to the errors that may be associated with a more subjective diagnostic tool such as IHC, particularly in inexperienced hands. The ready availability of flow cytometric analysis in most laboratories has also led to its widespread use. Indeed, there is recent evidence that flow cytometry plays an important role in staging of DLBCL and has an impact on outcome factors (Talaulikar et al. 2008).
It is well known that BM involvement in NHL is more often apparent on trephine biopsy specimens rather than BM aspirates (Juneja et al. 1990; Horlyck and Thorling 1991; Bain 2001). This is likely to relate to the presence of BM fibrosis causing false-negative results on aspirate samples. It follows that flow cytometric assessment of aspirates can also yield false-negative results (Hanson et al. 1999; Perea et al. 2004; Talaulikar et al. 2008), whereas if flow cytometric assessment of trephine biopsy samples was performed, a greater positivity rate may be obtained. There is no published literature addressing this issue; this may be because using some of the biopsy specimen for flow cytometric analysis could compromise availability of tissue for histological evaluation. In most cases of NHL, it is recognized that biopsy specimens need to be at least 16 mm in length and that several levels require examination for optimal results (Bain 2001; Campbell et al. 2003). Obtaining additional biopsy tissue for flow cytometric analysis may inconvenience the patient significantly. Immunophenotyping on BM trephines using IHC is therefore a logical ancillary study in staging BM.
Most studies have focused on the use of IHC on BM trephines in ambiguous cases to differentiate between benign lymphoid aggregates and malignant infiltration. We are aware that many centers within and outside Australia do not use IHC routinely in staging bone marrows, partly because of the cost involved and partly because of the lack of evidence regarding its use. Other studies have looked at the use of IHC alone but have not reported results for routine morphology and immunostaining separately (Palacio et al. 2001; Mazur et al. 2004).
The role of IHC in routine clinical practice to detect occult lymphoma in the BM and its effect on patient survival is largely unknown. This study aimed to assess the clinical use of routine IHC analysis in staging bone marrows in DLBCL, including its effect on outcome factors such as survival.
Materials and Methods
Patients
One hundred fifty-six retrospective cases diagnosed with histologically proven DLBCL at The Canberra Hospital from 1986 to 2005, on whom staging BM biopsies had been performed, were identified for the purpose of the study. After approval was obtained from the Australian Capital Territory (ACT) Human Research Ethics Committee, clinical information on patients was collected from the Medical Records department at The Canberra Hospital.
The average age of the patient cohort (known in 154 cases) was 61 years (range, 20-87 years), and the male to female ratio was 1.5:1. Staging data were available in 148 patients. Using routine staging procedures, 37/148 (25%) had Stage I disease; 35/148 (23.6%) had Stage II disease; 45/148 (30.4%) had Stage III disease; and 31/148 (20.9%) had Stage IV disease. Baseline assessment of IPI was possible in 148 patients. Fourteen patients had an IPI of 0 (9.5%), 23 patients had an IPI of 1 (15.5%), and 36 had an IPI of 2 (24.3%). IPIs of 3, 4, and 5 were noted in 46 (31.1%), 22 (14.9%), and 7 patients (4.7%), respectively. The mean baseline IPI of the patient cohort was 2.41 with an SD of 1.3.
Treatment data were available on 142 patients, with almost all patients having been treated with anthracycline-based regimens. Nine patients were treated with palliative intent with steroids alone or in combination with non-anthracycline-based drugs. Only 36 patients (22.2%) received rituximab. The median overall survival of the entire patient group was 58 months [95% confidence interval (CI), 33; 82 months].
BM Histology
BM biopsies are performed as a routine assessment for all cases with NHL at first diagnosis in our institution. Routinely, all trephines are fixed in buffered formalin and acetic acid. Decalcification is performed using 5% nitric acid. Samples are embedded in paraffin, and an attempt is made to stain four sections with hematoxylin and eosin (H&E). Additionally, for one to two sections, a Giemsa stain is performed. Silver impregnation is performed for reticulin. H&E, Giemsa, and reticulin preparations on the trephine biopsy were retrieved for review. The mean trephine length for the patient cohort was 17.6 mm, with a range of 8-36 mm, and the mean number of levels on H&E sections was 3.7 (range, 1-8).
All slides were reviewed blindly by two hematologists, with discrepant cases (n = 20) being reviewed by a third. Cheson criteria were used to classify trephine biopsy samples as positive, negative, or indeterminate (Cheson et al. 1999). Cases with paratrabecular lymphoid aggregates, large-sized aggregates, presence of large cells within aggregates, and increased reticulin response were classified as positive for involvement. Benign lymphoid aggregates were classified as those that were intertrabecular in location, small in size, well circumscribed, and contained predominantly small cells admixed with reactive cells.
IHC
IHC analysis was performed on a Ventana Benchmark NexES machine (Ventana Medical Systems Inc; Tucson, AZ) for all cases on archived formalin-fixed, paraffin-embedded trephine biopsies. The streptavidin-biotin method was used to immunostain sections using the following monoclonal antibodies: CD3 (Dako clone CD3, DakoCytomation Inc, Carpenteria, CA; 1:200 dilution), CD45RO (Novacastra clone UCLH-1, Novacastra Laboratories Ltd, Newcastle, UK; 1:1000 dilution), CD20 (Zymed clone L26, Zymed Laboratories, Invitrogen Immunodetection Corp, Carlsbad, CA; 1:50 dilution), CD79a (Dako clone JCB117, 1:500 dilution), κ (Novacastra clone kp-53, 1:750 dilution), and λ (Novacastra clone Hp-6054, 1:750 dilution). CD20 and CD3 are known to be most sensitive at assigning lineage in diffuse aggressive NHL (Chadburn and Knowles 1994) and are the most commonly used antibodies in our laboratory. The two additional antibodies, CD79a and CD45RO, were selected to maintain consistency because these are the antibodies used for diagnostic tissue sections in our laboratory. Heat retrieval was used for all antibodies, and tonsillar tissue was used as a positive control. A formal system of reporting was developed and was followed for all stains. Staining for each antibody was reported as positive/negative, normal/ abnormal, individual scattered cells/clusters, small/large cells, and percent of biopsy involved (<1%, 1-5%, or >5%). All slides were reported by two pathologists blinded to the previous assessment on histology.
The features described to define abnormality on IHC reflected the Cheson criteria for routine histology, although a fairly conservative approach was adopted by the pathologists to avoid false positives. Overall, location of infiltrates, size of cells, number of cells compared with controls, and nuclear morphology were used.
The presence of clusters of B cells was classified as abnormal or malignant when there were large number of clusters, the clusters were large sized, or they contained disproportionate numbers of larger cells. Scattered malignant cells may be missed quite easily on routine histology (Fraga et al. 1995) but be more easily discernible on IHC analysis. Such cases were classified positive when numbers of B cells were increased compared with controls. These were cases with morphologically normal marrows (n = 6) that were used to create a visual impression of normal amounts of background T and B cells. Overall, a fairly conservative approach was adopted to avoid false positives.
Statistical Analysis
Response and survival data were recorded for each patient. Besides descriptive analysis, Kaplan Meier curves were created with death as outcome. Stepwise (LR) multivariate Cox regression analysis was used to establish how IHC compared with routine histology as a predictor of survival. Similar analysis was also performed to assess whether a revised IPI computed by addition of immunostaining-positive cases was better at predicting survival compared with the baseline IPI. Patients treated with palliative intent were excluded from all survival analyses. All analyses were performed using the software program Statistical Package for Social Sciences (SPSS) version 14.0 (SPSS Inc; Chicago, IL).
Results
Histology
Of the 156 cases on which BMs could be evaluated, 24 were noted to be positive on routine histology; 6 cases were reported as indeterminate using Cheson criteria. Rather than using immunostaining to aid diagnosis, an attempt was made to resolve these on consensual review of routine H&E slides; all cases were agreed on as being positive for involvement on consensual review. H&E stains showed no evidence of involvement in 126 cases.
IHC
Paraffin-embedded blocks were available in 154 cases. IHC using T- and B-cell markers showed involvement in 43 cases. Of these, routine H&E slides were unavailable for comparison in one case. Of the remaining, routine histology showed involvement in 25 cases, whereas 17 cases were reported as not involved. In other words, use of IHC routinely on all cases detected 17 additional cases (11.0%) with BM involvement. Of the remaining 112 cases, 10 were reported initially as possible for involvement. Using a fairly conservative approach, all cases were classified as negative on consensual review. Of the remaining 102, 5 were reported as involved on H&E, including 2 cases that were previously reported as indeterminate. IHC results were reviewed again after being unblinded to routine histology results and showed that there were small involved areas on routine histology slides that were not apparent on deeper sections taken for IHC. Together, routine histology and IHC detected involvement in 48 cases. Variable expression was noted on the two B-cell markers CD20 and CD79a, with CD20 showing more consistent and strong expression.
IHC results on individual T-cell and B-cell antibodies
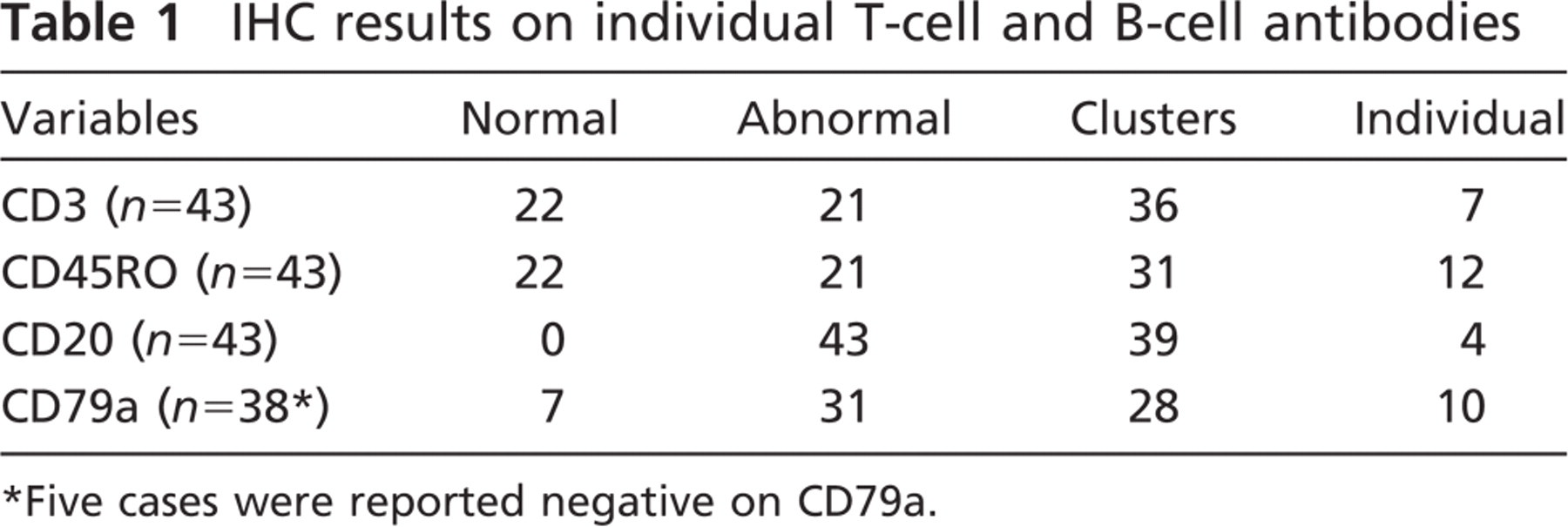
Five cases were reported negative on CD79a.
The IHC findings for individual antibodies are listed in Table 1. Eleven (25.6%) of the 43 involved cases had small cells, whereas the remaining 32 (74.4%) had large cells. Fourteen (32.6%), 10 (23.3%), and 19 cases (44.2%) had <1%, 1-5%, and >5% of B cells infiltrating the marrow, whereas T-cell infiltration was as follows: 32 (74.4%) cases with <1%, 4 (9.3%) cases with 1-5%, and 7 (16.3%) cases with >5% infiltration. Of all cases reported as positive on B-cell markers, only 15 showed clear evidence of light chain restriction. Twenty-three cases showed no light chain restriction.
Effect on Outcome
IPI
The results of IHC were added to those of routine histology to redefine BM involvement. A new revised IPI (rIPI) was computed for all cases based on the IHC results. Changes to the IPI essentially occurred when stage of disease was upgraded from Stage 1 or 2 to Stage 4 disease. Marrow involvement was also calculated as an additional extranodal site of involvement, further changing the IPI in some cases. Of 144 cases where rIPI was assessable, 9 cases had an rIPI of 0, 18 had an rIPI of 1, and 33 had an rIPI of 2. Forty, 31, and 13 cases had an rIPI of 3, 4, and 5, respectively.
Survival
Kaplan-Meier curves were created to assess the impact of BM involvement on overall survival. When routine histology alone was used to define BM involvement on H&E staining, the difference in median survival between patients with and without involvement was 40 vs 81 months (p=0.02; Figure 1). Using positivity on IHC to define BM involvement, the median survival of patients with lymphoma in their BM was 28 vs 82 months (p<0.0001; Figure 2).
Kaplan-Meier curves were created to assess the impact of small cell vs large cell infiltration, and the degree of B-cell infiltration. The median survival times for cases with discordant (small cell) involvement were better than those for concordant or large cell involvement (33 and 22 months), although the difference was not significantly significant (p = 0.7). The median survival of cases with <1%, 1-5%, and >5% B-cell infiltration was 40, 33, and 15 months. In other words, prognosis seemed to worsen with increased B-cell infiltration, although this again was not statistically significant (p = 0.7).
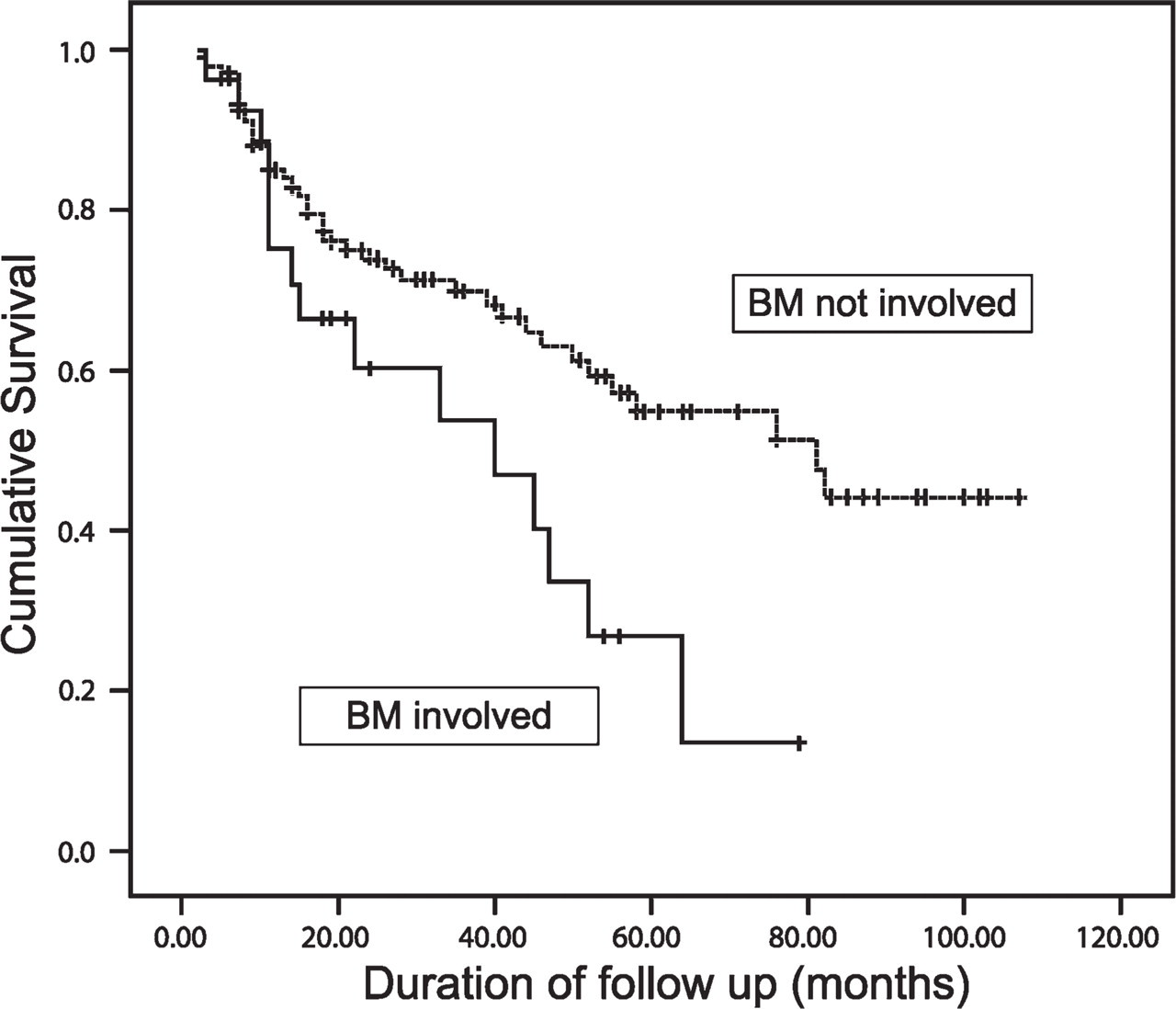
When routine histology on trephine biopsies was used to look for bone marrow involvement, the difference in survival between patients with and without involvement was 40 vs 81 months (p = 0.02).
Multivariate Analysis
Using a multivariate forward stepwise (likelihood ratio method) Cox regression, marrow involvement as defined by three different methods was competitively considered for the contribution to predicting survival. The three definitions used were positivity on histology alone (H), positivity on immunostaining alone (I), and positivity on histology or immunostaining (H + I). In the analysis, it was found that the definition using immunostaining alone (I) contributed significantly more to explaining survival than the other two and that, after the immunostaining model was included in the regression model, the definitions using histology alone and that using both modalities together did not significantly contribute to predicting survival (p = 0.1, 0.66; Table 2). Degree of malignant infiltration on the biopsy and concordant vs discordant involvement was also included in the model but did not significantly contribute over and above the listed variables (p = 0.95 and p = 0.56).
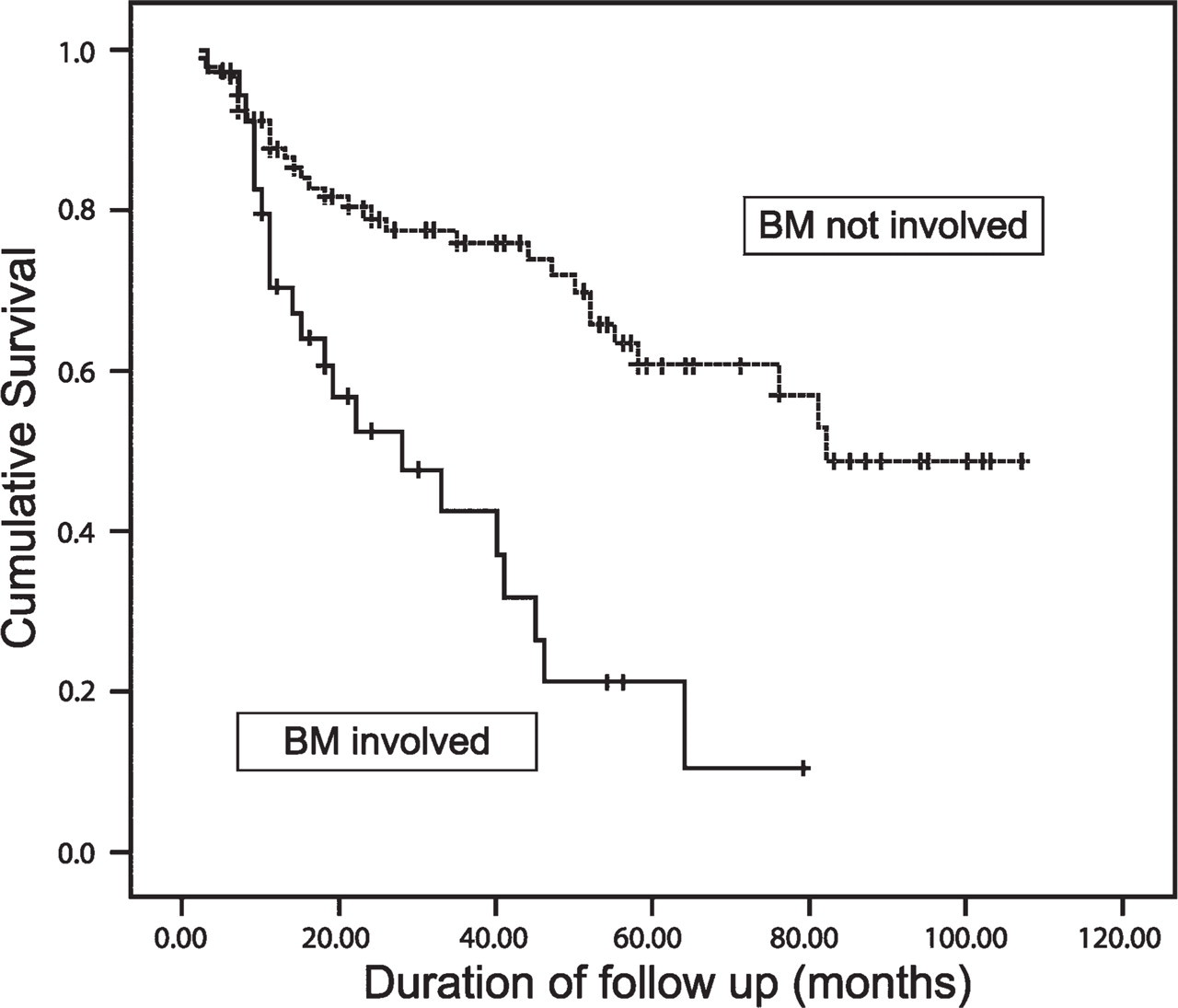
When immunostaining was used as a routine in all cases, the difference in survival between patients with and without marrow involvement was 28 vs 81 months (p<0.0001).
To study the effect of treatment with rituximab on survival, this too was considered, but not found to contribute significantly to the Cox regression model (p = 0.8).
However, when a similar Cox regression analysis was performed to compare revised and baseline IPI, rIPI did not contribute significantly to survival over and above baseline IPI (p = 0.4). Although the mean rIPI among patients who did not survive was higher than the mean baseline IPI [3.22 (95% CI, 2.87, 3.57) vs 2.92 (95% CI, 2.59, 3.25)], this was also the case in patients who were alive at the time of analysis [2.38 (95% CI, 2.01, 2.63) vs 2.03 (95% CI, 1.73, 2.32)].
Discussion
This study looked at the role of routine IHC in staging DLBCL at initial diagnosis. Our results indicate that, in experienced hands, use of immunostaining surpasses routine histology by detecting occult disease in ∼10% of cases. Moreover, immunostaining alone is a stronger predictor of survival than routine histology.
Detection of occult BM involvement by lymphoma hinges on the adequacy of both routine histological diagnosis and IHC analysis. There are several variables that affect adequacy of routine histological diagnosis on BMs. It was previously believed that bilateral trephine biopsies increased the yield from staging BMs in NHL (Juneja et al. 1990). However, it is now established that bilateral sampling is not required if adequate tissue (including adequate trephine length and number of levels examined) is available for diagnosis (Campbell et al. 2003). Our mean trephine length was reasonable at 17.6 mm, with a range of 8-36 mm. Fifty-five cases had a less than recommended trephine length of <16 mm, although only 7 had a length <10 mm. This may have contributed to some extent to the negative results obtained on routine histology. However, practically, it is often not possible to obtain larger samples in some cases. An attempt to compensate for this is made in our institution by assessing more levels in smaller trephine biopsy specimens.
Cox regression model showing the effect of different definitions of bone marrow involvement on survival after adjusting for age and performance status ∗
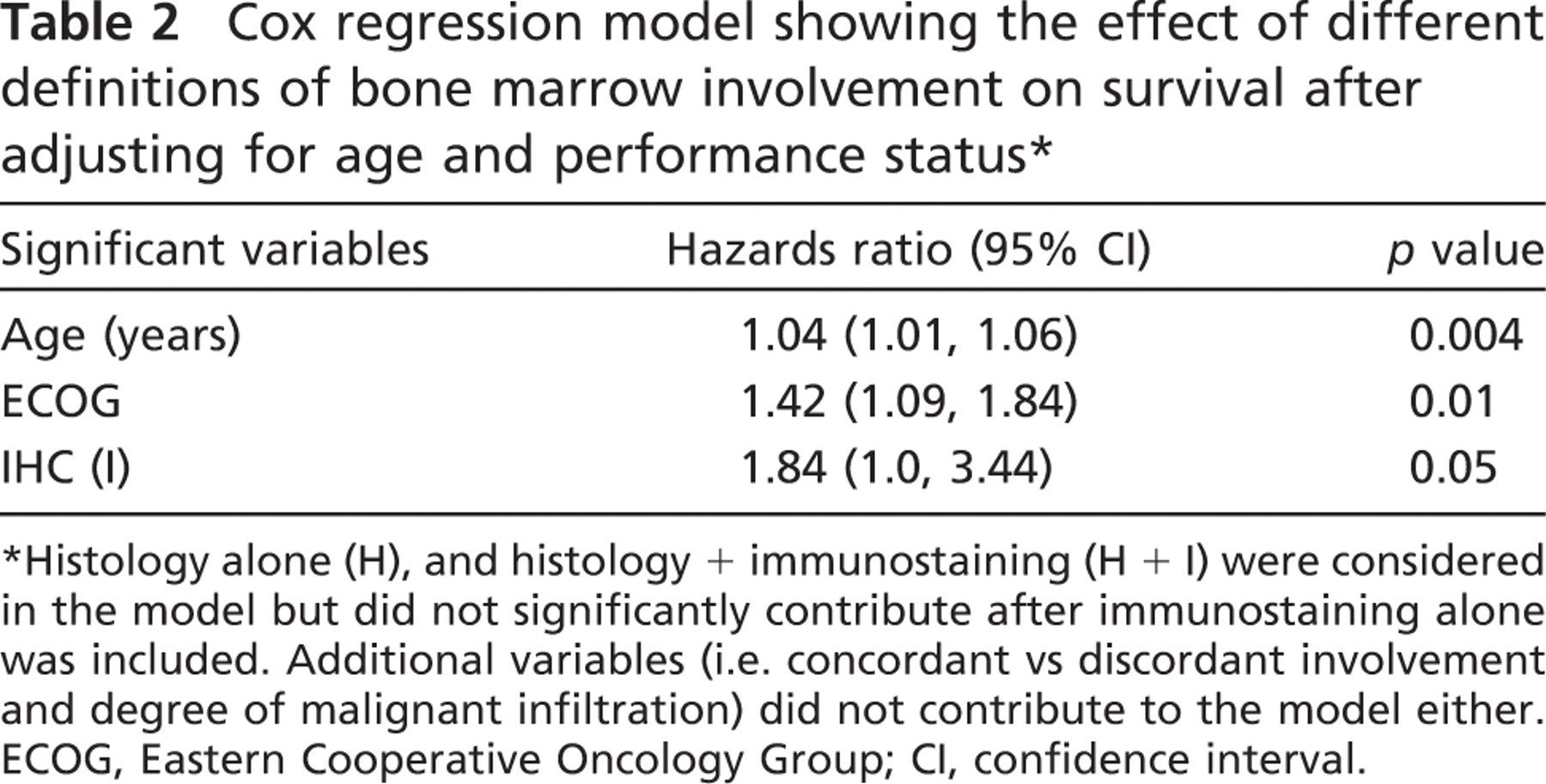
Histology alone (H), and histology + immunostaining (H + I) were considered in the model but did not significantly contribute after immunostaining alone was included. Additional variables (i.e. concordant vs discordant involvement and degree of malignant infiltration) did not contribute to the model either. ECOG, Eastern Cooperative Oncology Group; CI, confidence interval.
The mean number of levels examined on H&E sections was 3.7 (range, 1-8). Fifty cases had less than four levels examined; of these, 12 had three levels examined, 37 had two levels examined, and only one had a single level examined. Including a single level each on Giemsa stain and silver reticulin stain, only one case had less than four levels. It is possible that some of the positive results on immunostaining seen in our study were related to examination of more tissue. Two examples where discrete populations of large B cells were noted on immunostaining that were not apparent on careful review of routine histology slides are shown in Figure 3. A previous study by Campbell et al. (2003) established that four levels is the optimal number that need to be examined for routine morphological assessment in staging DLBCL. A similar study is required to assess how much of the benefit obtained on immunostaining is caused by examination of multiple levels.
It is acknowledged that the detection of lymphoma in the marrow is subjective and depends on the experience and skill of the observers, particularly in interpretation of lymphoid aggregates as being benign or malignant. The use of standardized criteria is now therefore recommended for classifying cases as positive, negative, or indeterminate for involvement with lymphoma (Cheson et al. 1999). This was followed in our study and may have been responsible for more cases being classified as negative. Another likely factor that may have contributed is that the investigators were blinded to the flow cytometry results on BM aspirates. Hanson et al. (1999) have previously reported no benefit from flow cytometry or immunostaining to routine histological diagnosis in all subtypes of NHL. Interestingly, the concordance between histology and flow cytometry in their study was very high at 91.4%. Of the 15 cases that showed discordance between the two diagnostic modalities, there were twice the number of cases (n = 10) positive on histology and negative on flow cytometry than those that were flow positive and histology negative (n = 5). In other words, most cases positive on flow cytometry were also reported as positive on histology (Hanson et al. 1999). We believe that being blinded to flow cytometry results may have allowed a better correlation of routine histology and IHC in this study. We did not analyze the flow cytometry results in a more comprehensive fashion in this study. However, previous results comparing flow cytometry and morphology showed slightly lower concordance rates of 83% (Talaulikar et al. 2008).
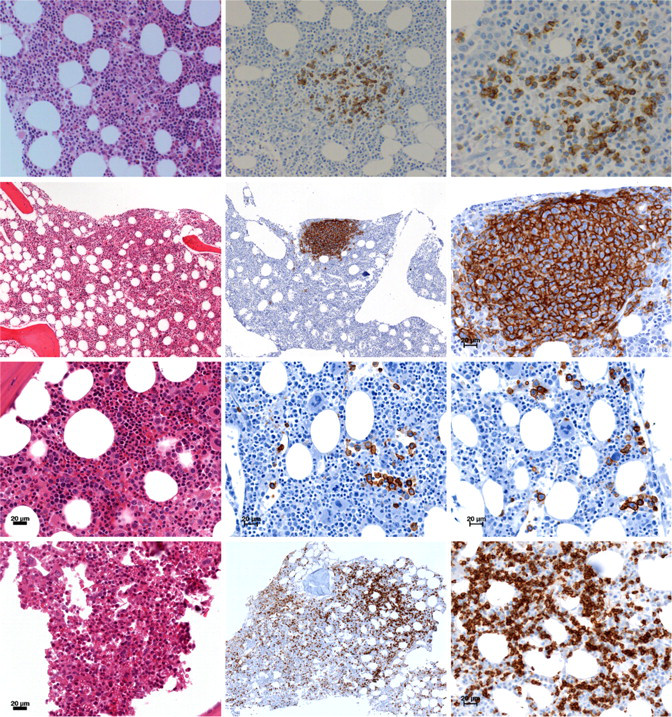
Examples in which routine histology showed no evidence of involvement. Horizontally, top and second panels show cases where, when further sections were cut for IHC analysis, discrete populations of large B cells were noted. Third panel shows a case where routine histology failed to detect scattered large abnormal lymphoid cells that were picked up on IHC. Bottom panel shows a case with scattered small cell disease on IHC with B-cell clusters.
There are other differences between our study and that of Hanson et al. (1999). They included cases of all subtypes of NHL of which only 74 cases were DLBCL (42.2%). They reported 6% BM involvement. This is much lower than published rates of involvement in DLBCL (Conlan et al. 1990; Campbell et al. 2003) and those found in our patient population (30/156, 19.2%). Moreover, in the study by Hanson et al. (1999), only 107/175 cases related to initial presentation; the rest were restaging marrows. This may have had an impact on the final outcome. The mean trephine length of biopsies is not indicated in the study of Hanson et al. (1999). However, bilateral biopsies were performed in all cases, and at least three levels per biopsy were examined. This indicates that routine histological analysis was more comprehensive; however, this, in our experience, is often not practically possible.
Adequacy of IHC analysis is a contentious issue prone to the same subjective errors as routine histology. We used two B-cell and two T-cell markers to corroborate our findings. CD20 and CD3 have been shown to be most sensitive at assigning lineage in diffuse aggressive NHL (Chadburn and Knowles 1994) and are the most commonly used antibodies in our laboratory. The two additional antibodies, CD79a and CD45RO, were selected to maintain consistency because these are the antibodies used in diagnostic tissue sections. CD79a has an advantage over PAX5 in that it helps to differentiate T cell-rich B-cell lymphomas from Hodgkin Reed Sternberg cells (Isaacson 2007). CD45RO was preferred over CD5 as a T-cell marker because of reports that CD5 expression can occur in DLBCL and may have prognostic significance (Taniguchi et al. 1998; Harada et al. 1999). All results were assessed by two reviewers. Standardized criteria were established and used to classify cases as positive or negative as described in the Materials and Methods section. Furthermore, we believe that our survival data showing that immunostaining alone is better at predicting survival (compared with routine histology) indicates that our immunostaining results are likely to be rigorous.
We found in our series of patients that, of the 43 cases detected to have involvement on IHC, 11 (25.6%) had small cells, whereas the majority (32, 74.4%) had large cells. This is a higher degree of concordant involvement than has been reported by Chung et al. (2007) (∼50%) and Campbell et al. (2006) (∼28%) and may be caused by involvement being measured on IHC rather than routine histology. Although a trend toward better survival was noted with discordant rather than concordant involvement, this was not statistically significant and may be because of the small numbers, especially when cases treated with palliative intent were excluded. Similarly, the degree of malignant infiltration did not impact on survival. Also, contrary to the findings of Campbell et al. (2006), we did not find a significant association between the degree of infiltration and concordant involvement (X 2: 3.8, df: 2, p = 0.15). This is likely to be because we defined positive cases on IHC rather than routine histology.
A few studies have addressed the issue of detection of histologically inapparent disease using immunostaining. Fraga et al. (1995) reported that in a case series (n = 42) of anaplastic large cell lymphoma, routine histology detected marrow involvement in 17% cases. Routine IHC analysis using CD30 detected occult disease in a further 23% cases (Fraga et al. 1995). We found BM involvement on routine histology in 19.2%, with a more modest 11.1% rate of occult involvement. The authors of the previous study postulated that the inability of routine histology to detect low level disease was related to the scarcity of malignant cells among normal hemopoietic cells and the difficulty in distinguishing them from immature hemopoietic cells. They recommended the systematic use of immunostaining to detect BM involvement in anaplastic lymphoma, which they reported as a poor prognostic factor. We believe a similar phenomenon occurs with low level marrow involvement in large cell lymphoma. The other major reason we postulate for detection of histologically inapparent disease in the BM by IHC is the examination of additional sections. This was reflected in our series by the cases that showed clusters of B cells on IHC that were not seen on routine histology.
Some technical issues were also highlighted by the study and deserve comment. Variable expression was noted on the two B-cell markers CD20 and CD79a. Previous studies have reported that decalcification, particularly with 5% nitric acid, has negative effects of certain clones of CD20, CD79a, CD5, and CD43 (Miller et al. 2000). This may have been responsible, along with other factors, for the weak expression of CD79a. We were unable to find any other published observations that may be responsible for this phenomenon.
We were able to establish clonality in only one third of cases (15/42, 35.7%). There is some literature to suggest that flow cytometry may show variable expression of antigens from different anatomic sites in cases of NHL (Gervasi et al. 2004). Whether this is related to technical issues or a true loss of antigen expression as a result of a biological phenomenon remains to be established. However, because strong positivity was noted on external and internal (plasma cells stained positive) controls, we believe the latter is more likely. Similar variability of expression of some antigens has also been reported to occur over time in B-cell NHL (Echeverri et al. 2002). However, that is unlikely to be responsible for the results in our study because all biopsy samples were from initial diagnosis.
There are a number of advantages to use of routine immunostaining of trephine biopsies for staging DLBCL. IHC techniques are generally well established, available in most centers, and relatively cost effective. They enable the examination of a greater number of levels of the biopsy in a more comprehensive and sensitive manner and are useful in the detection of additional clusters of malignant cells and that of scattered malignant cells among normal hemopoietic cells.
Despite the use of more realistic measures of routine histological diagnosis such as unilateral biopsies and assessment of less than optimal trephine lengths, we have been able to show that immunostaining in experienced hands is more effective at predicting survival than routine histology. There are several other limitations of this study besides those inherent to retrospective data. We acknowledge that results of IHC analysis are subjective and can be very variable in less experienced hands. Also, there may be a degree of variability caused by the use of different antigen retrieval methods and processing of specimens (Miller et al. 2000).
In summary, we showed that IHC analysis using B-and T-cell markers detects morphologically inapparent marrow involvement in ∼11% of cases of DLBCL at initial diagnosis. Moreover, immunostaining alone is a stronger predictor of survival than routine histology alone. Although the findings are interesting and suggest that routine immunostaining should be incorporated into staging of DLBCL, further large series of prospective data are required to corroborate the findings, especially in the rituximab era. Further studies are also required to establish whether the lack of light chain expression on BM trephine samples is related to a biological phenomenon.
Footnotes
Acknowledgements
The authors acknowledge the financial support provided for the study by the Private Practice Trust Fund, The Canberra Hospital, and the equipment grant provided by The Leukaemia Foundation, Australia. The principal investigator/author received a supplementary scholarship from the Arrow Bone Marrow Transplant Foundation, New South Wales, for the project.