
Abstract
Phosphorylated biomarkers are crucial for our understanding of drug mechanism of action and dose selection during clinical trials, particularly for drugs that target protein kinases, such as DNA-damage-response (DDR) inhibitors. However, tissue fixation conditions needed to preserve DDR-specific phospho-biomarkers have not been previously investigated. Using xenograft tissues and tightly controlled formalin fixation conditions, we assessed how preanalytical factors affect phosphorylated DDR biomarkers pRAD50(Ser635), ɣH2AX(Ser139), pKAP1(Ser824), and non-phosphorylated biomarkers cMYC and ATM. Cold ischemia times ranged from 15 min to 6 hr, and the fixation duration ranged from 24 hr to 4 weeks. Epitopes pRAD50 and pKAP1 appeared the most labile assessed with staining loss after just 15 min of cold ischemia time, while ATM was more robust showing consistent expression up to 1 hr of cold ischemia. Notably, ɣH2AX expression was lost with formalin fixation over 48 hr. The use of core needle biopsies where possible and novel fixation methods such as the 2-step temperature-controlled formalin approach may improve phosphorylated biomarker preservation; however, practical challenges may affect wider clinical application. The most essential tissue-processing step when downstream analysis includes DDR phosphorylated biomarkers is immediate tissue submersion in formalin, without delay, upon excision from the patient, followed by room temperature fixation for 24 hr.
Introduction
Biomarkers have been used in cancer therapy for decades to aid diagnosis and give insight into disease prognosis. We are now in an era of personalized oncology medicines, placing further importance on accurate detection of tumor biomarkers in patient samples. Personalized medicines such as anti-programmed death-ligand 1(PD-L1/anti-programmed cell death protein-1 (PD-1) immunotherapies and estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor 2 (HER-2) targeted drugs rely on immunohistochemistry (IHC) on patient tissue samples to guide therapy selection, based on the presence of the target biomarker.1 –3 IHC assays against PD-L1, ER, PR, HER2, and Ki67 are widely used across clinical sites, well-studied, and robust against delays of tissue fixation (Table 1).4 –6 Beyond the use in companion diagnostic assays, IHC is now regularly used to assess drug mechanism of action of new medicines in clinical trials. However, with the exponential growth in targeted-kinase inhibitors, there is increasing importance on understanding the robustness of phosphorylated epitopes in tumor tissues, which are frequently used to support pharmacodynamic (PD) biomarker assessments during drug development.
Review of Existing Literature Around Cold Ischemia Times and Tissue Biomarkers.
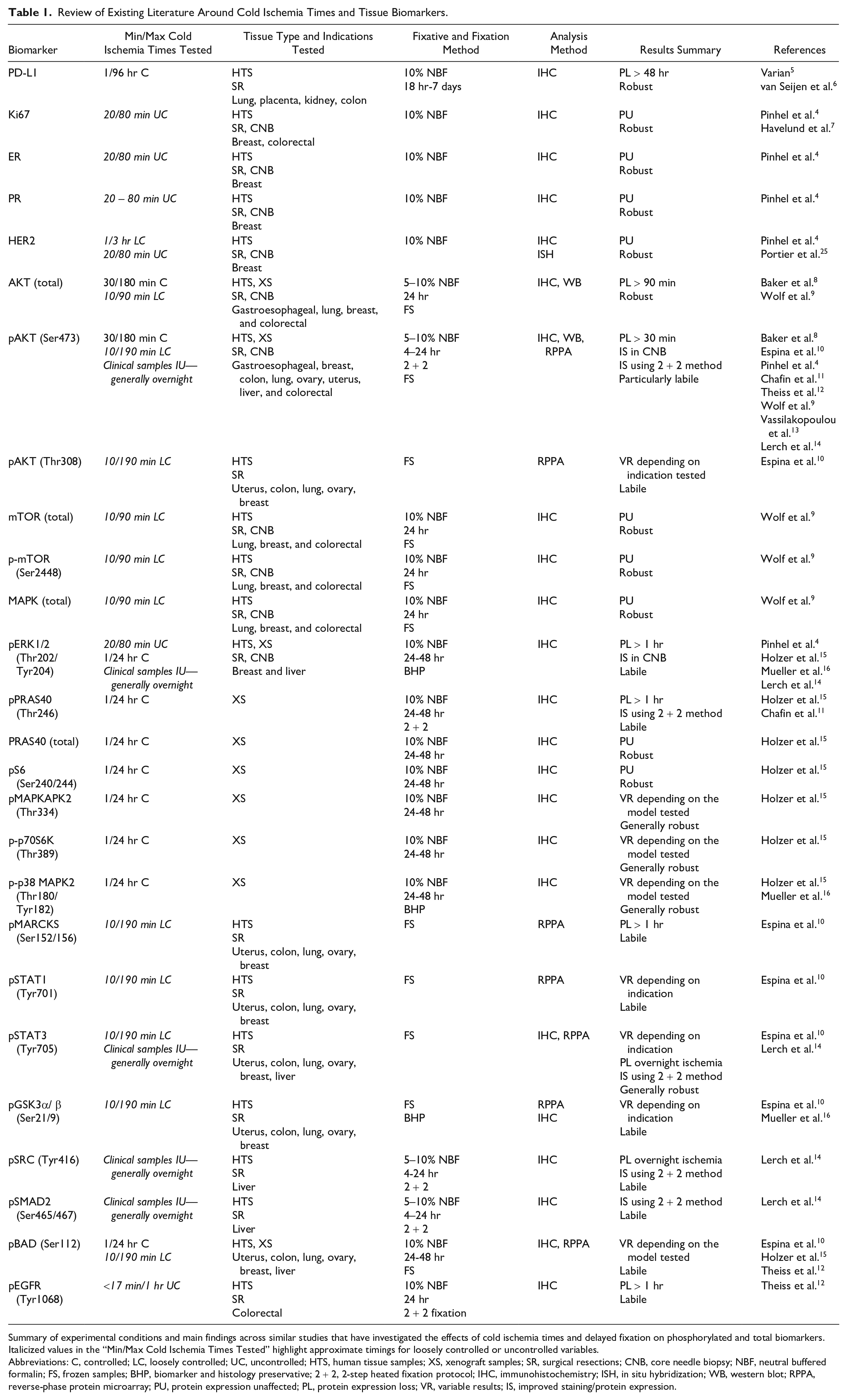
Summary of experimental conditions and main findings across similar studies that have investigated the effects of cold ischemia times and delayed fixation on phosphorylated and total biomarkers. Italicized values in the “Min/Max Cold Ischemia Times Tested” highlight approximate timings for loosely controlled or uncontrolled variables.
Abbreviations: C, controlled; LC, loosely controlled; UC, uncontrolled; HTS, human tissue samples; XS, xenograft samples; SR, surgical resections; CNB, core needle biopsy; NBF, neutral buffered formalin; FS, frozen samples; BHP, biomarker and histology preservative; 2 + 2, 2-step heated fixation protocol; IHC, immunohistochemistry; ISH, in situ hybridization; WB, western blot; RPPA, reverse-phase protein microarray; PU, protein expression unaffected; PL, protein expression loss; VR, variable results; IS, improved staining/protein expression.
Kinases are common targets of oncology drugs because dysregulation of their signaling pathways frequently contributes to both the onset and progression of cancer. There are 113 drugs targeting kinases currently approved, including both kinase inhibitors and monoclonal antibodies, and hundreds more in clinical development. Protein kinases play an essential role in posttranslational modifications by catalyzing the transfer of phosphate groups by adenosine triphosphate hydrolysis to a specific amino acid on a target substrate. 17 These phosphorylation events allow tight regulation of fundamental cellular processes such as cell growth, cell division, cell death, DNA repair, signal transduction, gene transcription, and protein synthesis. To understand if drugs targeting kinase inhibitors have achieved sufficient target engagement to reach an efficacious dose, analysis of changes to phosphorylated biomarkers in patient tumor tissues after the therapy is crucial. However, increased lability of phosphorylated epitopes compared with their non-phosphorylated counterparts should be a consideration in clinical trial design to ensure the accuracy of the PD biomarker data generated.
Collection and formalin fixation of tumor tissues followed by processing into a formalin-fixed paraffin-embedded (FFPE) block is still the standardized technique used in clinical sites across the globe for biomarker analysis. Accuracy of the biomarker analysis, particularly for IHC, is dependent on the quality of the tissue provided. A number of studies have found quality varies across clinical sites as tissue collection, fixation, and tissue processing protocols are not standardized or regulated.8,9,14,18 The College of American Pathologists (CAP) defines cold ischemia time as the time from excision of the specimen from the surgical site to the time the tissue is placed in the fixative. 19 Extended cold ischemia times have been shown to cause tissue degradation and loss of epitopes4,8 –10,12,14,15 and preanalytical artifacts such as false localization of protein expression, indistinct nuclear chromatin staining, and loss of cellularity caused by insufficient or prolonged fixation have also been found.3,20
In line with a number of approved epidermal growth factor receptor (EGFR) targeted therapies and inhibitors against downstream targets of this pathway, phosphorylated biomarkers related to the mitogen activated protein kinase (MAPK) and phosphatidylinositol-3 kinase (PI3K)/protein kinase B (AKT)/mammalian target of rapamycin (mTOR) signaling pathways have been the most comprehensively studied, including pMAPK, pSTAT1/3, pERK1/2, p-p38, pAKT, pGSK3β, and pPRAS40. These phospho-epitopes have shown variable amounts of lability when tissues are subjected to cold ischemia times ranging from 10 min to 24 hr.4,8 –10,14,15 See Table 1 for additional biomarkers studied and more detailed results. However, for the emerging DDR field of tyrosine kinase inhibitors, such as those targeting ataxia-telangiectasia-kinase (ATM) and ataxia-telangiectasia-mutated and Rad3-related (ATR) pathways, there are no studies investigating the lability of their downstream phosphorylated biomarkers such as pRAD50, phospho-histone H2A.X (ɣH2AX), and phospho-KRAB-associated protein-1 (pKAP1).21,22
The American Society of Clinical Oncology, together with CAP, provide guidance on how to collect, handle, fix, and process tissues before biomarker analysis, 23 but there is limited information available of the best practices to use for phosphorylated biomarkers that have more labile epitopes and may be more readily degraded by tissue proteases or phosphatases if not adequately fixed. One study recommended a rapid two-step approach to preserve phosphorylated biomarkers, achieved by a preincubation cold formalin step, to inhibit endogenous proteases, quickly followed by a brief heated formalin step, to accelerate penetration of the fixative and cross-linking of proteins 11 In addition to increasing the yield of downstream phospho-epitopes in IHC analysis, this method also presents the possibility to reduce fixation time from 24 hr to 4 hr.
Here, we use highly controlled xenograft experiments with unique methodology to test cold ischemia and extended fixation times within tight parameters, as well as compare alternative fixation practices. For the first time, we provide detailed IHC assessment of the effects of non-optimal fixation on phosphorylated biomarkers downstream of the DDR signaling pathways and propose additions to the guidelines surrounding tissue fixation for phospho-epitopes that are particularly labile.
Materials and Methods
Human Tissues
Human ovarian carcinoma samples were obtained from Avaden Biosciences with appropriate patient consent and ethical approval. All human tissue samples were obtained under AstraZeneca’s global bioethics policy (https://www.astrazeneca.com/content/dam/az/our-company/Documents/Bioethics-Policy.pdf).
Animal Studies
Patient-derived xenograft (PDX) sample CTG-2011 was derived from a patient with non-small-cell lung cancer (NSCLC) and obtained from Champions Oncology. Animal studies were performed in accordance with relevant guidelines and regulations. All other tissue samples were obtained from in vivo studies that were run in the United Kingdom in accordance with all relevant ethical regulations for animal testing and research, including UK Home Office legislation, the Animal Scientific Procedures Act 1986, AstraZeneca’s Global Bioethics Policy, and the Home Office Project Licenses P0EC1FFDF and PP3292652, which received ethical review and approval through the AstraZeneca Ethical Review Process. Xenograft models of NCI-N87 and SUM149PT cell lines were established in mice using the conditions described in Table 2. Mice weighed more than 18 g at the time of the first procedure. NCI-N87 tumors were collected from untreated control mice after reaching volumes of 0.200–0.700 cm3. Upon collection, tumors were immediately divided into 4 equally sized pieces (Appendix Fig. 1A) and either immediately fixed or left at room temperature before fixation depending on the experimental group, and these samples will be referred to as “TMA 1” (tissue microarray 1) hereafter. For 2-step protocol versus 1-step, a SUM149PT breast cancer xenograft model was used, and tumors were divided into two pieces (Appendix Fig. 1B); these samples will be referred to as “TMA 2” hereafter.
Description of Mouse Models Used to Generate Samples for Evaluation.

Samples from a gastric carcinoma NCI-N87 mouse model were used for TMA 1, while samples from a triple-negative breast cancer SUM149PT mouse model were used for TMA 2. Mouse models were selected based on sample availability.
Matrigel (#354234, Corning, New York USA, www.corning.com)
Tissue Fixation Protocols
All tissues were fixed in 10% neutral-buffered formalin (pH 7), supplied by Avantor Services 41G Oncology/Alderley Park Lab and Production Services, UK. For samples in TMA 1, two variables were explored: delay to fixative (cold ischemia) and extended fixation. For delay to fixative, tissue samples collected from xenograft models had cold ischemia times of 15 min, 30 min, 1 hr, 3 hr, or 6 hr, and there were two samples per condition (Table 3). After varying cold ischemia times, all samples were submerged in 10% neutral-buffered formalin for 24 hr. For extended fixation, samples were immediately submerged in 10% neutral-buffered formalin for 48 hr, 1 week, 2 weeks, or 4 weeks, and there were two samples per condition (Table 3). Two additional samples were immediately submerged in 10% neutral-buffered formalin for 24 hr and used as comparative controls for both variables. For samples in TMA 2, tumor tissues from each xenograft model were split into two samples: “A” and “B.” Sample B was immediately submerged in 10% neutral-buffered formalin for 24 hr (1-step fixation), and sample “A” was treated with the 2-step fixation protocol (Table 4). The 2-step fixation protocol was adapted from Chafin et al. 11 with 2 hr of fixation at 4C, followed by 2 hr in 45C formalin, and then 24 hr in formalin at room temperature.
Description of Sample Split and Fixation Conditions for Samples Used in TMA 1.
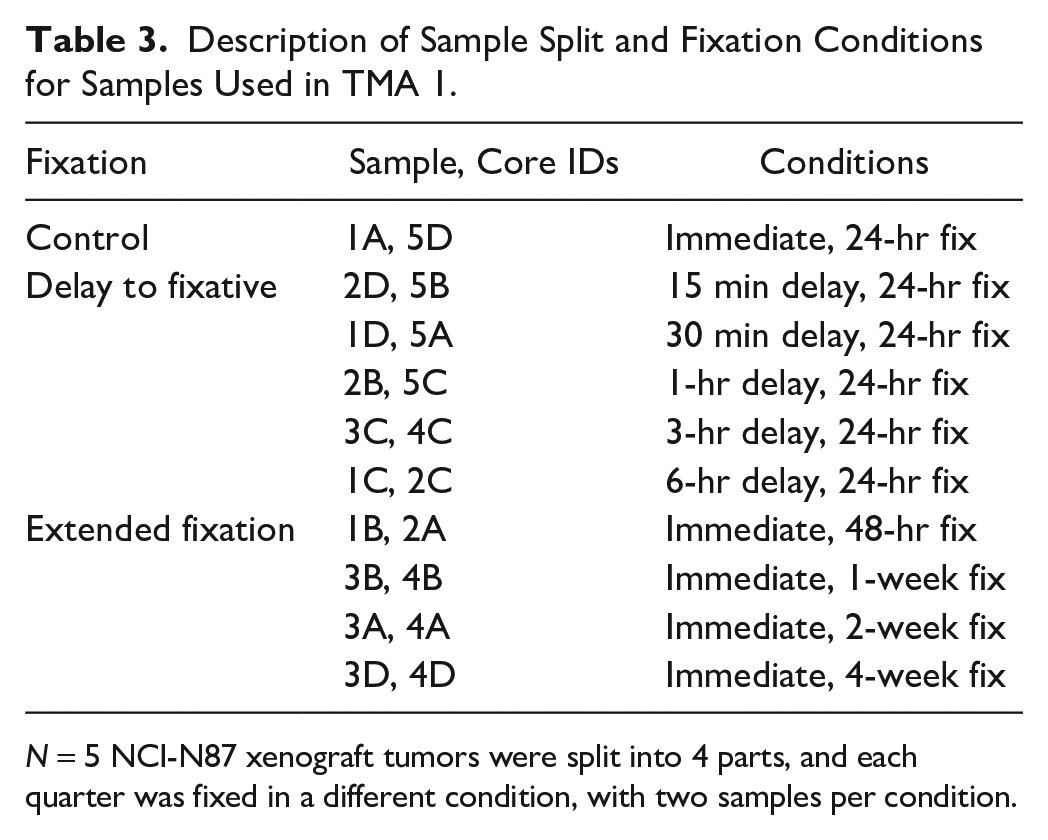
N = 5 NCI-N87 xenograft tumors were split into 4 parts, and each quarter was fixed in a different condition, with two samples per condition.
Description of Sample Split and Fixation Conditions for Samples Used in TMA 2.

N = 3 SUM149PT xenograft tumors were split into 2 parts; one half was fixed using the 1-step method, and the other half was fixed using the 2-step method.
Tissue Processing
After fixation, all tissues were transferred to 70% ethanol and processed into FFPE blocks using an automated program on a Leica ASP300S (Leica Biosystems, Wetzlar, Germany, www.leicabiosystems.com), described in Appendix Table 1.
Hematoxylin and Eosin Staining
Four-µm sections were taken from each FFPE block and left to dry overnight at 37C. Slides were then dewaxed in xylene, rehydrated through graded ethanols, before being stained for 5 min with Gills III Hematoxylin (Leica, #3801542E), followed by washing in running water, 1% acid alcohol (Leica, #110618), and Scott’s tap water and then staining in Eosin (Leica, #3801602E) for 3 min followed by running water, graded ethanols, and xylene. Slides were coverslipped using ClearVue mountant (#4212, Thermo Fisher Scientific, Waltham, Massacheusetts USA, www.thermofisher.com).
Tissue Microarray
Hematoxylin and eosin (H&E) slides of each block were visualized under a microscope to select tumor regions to punch cores from and place into the TMAs, which were constructed using the Tissue-Tek Quick-Ray Microarray System (Sakura Finetek, Torrence, California USA, www.sakuraus.com) and Quick-Ray molds with 3-mm-size cores. One core from the selected region (generally the center of the tumor) was taken per sample; there are two cores per experimental condition for TMA 1 (each core from one of five mice, samples distributed across different conditions) and three cores per experimental condition for TMA 2 (two samples per mouse, one per condition). The completed TMAs (Appendix Fig. 2) were then sectioned and H&E stained as described above.
Immunohistochemistry
IHC was carried out on 4-µm sections of human tissues and xenograft TMAs that had been left to dry overnight at 37C. Antibodies used and their corresponding tissue controls are detailed in Appendix Table 2. Matched-concentration IgG isotype control in place of the primary antibody step was tested during antibody validation. Staining of pRAD50 and ɣH2AX was carried out as described in Jones et al. 21 Staining of ATM was carried out as previously described. 24 Cellular myelocytomatosis (cMYC) and pKAP1 staining were carried out on the Ventana Discovery Ultra (Ventana Medical Systems, Roche Tissue Diagnostics, Tuscon, Arizona USA, www.roche.com), using EZ prep for deparaffinization; CC1 antigen retrieval at 100C for 64 min and 98C for 32 min for cMYC and pKAP1, respectively; followed by protein blocking with ChromoMap Inhibitor block (Roche) for 4 min. cMYC slides were incubated for 24 min with the predilute primary antibody cMYC (Y69) rabbit monoclonal (Roche, #790-4628). pKAP1 slides were incubated with casein antibody diluent (Roche 760-219), before antibody application, then incubated for 32 min with the pKAP1 antibody (Abcam ab133440) in 0.3% protein in 0.1M Tris buffered saline (pH 7.2) with 0.08% sodium azide (PSS) diluent (Roche 760-212). Detection was carried out using Anti-Rabbit HQ secondary (Roche) for 8 min, followed by Anti-HQ HRP (Roche) for 8 min, and then 3’,3’-Diaminobenzidine (DAB) staining. Hematoxylin II (Roche) and bluing reagent (Roche) were used for counterstaining nuclei.
IHC Image Analysis
All H&E and IHC slides were scanned at ×20 using the Aperio AT2 scanner (Leica). The image analysis of ɣH2AX was carried out on HALO (Indica Labs, Albuquerque, New Mexico USA, www.indicalab.com) using a tumor classifier to exclude any non-tumor cells and stroma, before applying a pixel quantification algorithm to calculate the percent-positive DAB-stained pixels per area of tumor tissue. Image analysis of pRAD50 and pKAP1 was carried out using the HALO cytonuclear algorithm to generate percent positivity as previously described in the study by Jones et al. 21 This same method was applied to the analysis of ATM and cMYC. Tumor classifiers and algorithms were adjusted per biomarker, and all data were quality checked by a pathologist.
Statistical Analysis
Paired t-test was performed using GraphPad Prism version 8.0.0 for Windows (GraphPad Software, San Diego, California USA, www.graphpad.com) to determine differences between two groups where samples were from the same mouse, and there were more than two replicates per group. A value of p<0.05 was considered significant.
Results
Differential Edge Biomarker Expression Indicates Fixation
In both the clinical and preclinical settings, tumor biopsies and resections are not always fixed immediately upon collection from patients or animals or may be too large for adequate fixation because of the time it takes for formalin to fully penetrate the sample. Digital image analysis of an ATM-stained human ovarian carcinoma sample illustrates a tissue fixation artifact known as an “edge effect” (Fig. 1A and B). Edge effect can occur when large tissue samples are placed into formalin and cells on the edge of the sample are immediately fixed and yield optimal IHC results, while cells in the center of the sample have had delay in fixation and suffer the detrimental effects of cold ischemia on antigen preservation (Fig. 1A). In this case, we use a heat map overlay of the positive cells to show strong positive ATM staining around the outside of the ovarian sample (on average up to 2-mm depth) but loss of staining toward the center of the tumor sample (Fig. 1B). We also show evidence of edge effect with pRAD50 staining in a PDX model from a NSCLC patient (CTG-2011), where high-intensity (3+) cells are lost in the center of the tissue (Fig. 1C and D). Of note, the edge effect is often more noticeable by eye with biomarkers that have more homogenous expression patterns such as ATM, rather than phosphorylated biomarkers that may be more heterogenous.

Inadequate penetration of formalin results in edge affect tissue artifact. (A) ATM IHC raw staining and digital image analysis overlay of an ovarian carcinoma sample. (B) Spatial analysis heatmap shows the density of tumor cells classified as ATM positive. (C) pRAD50 IHC raw staining and digital image analysis overlay of the CTG-2011 PDX sample. (D) Spatial analysis heatmap of density of 3+ positive pRAD50 tumor cells displaying how biomarker analysis is affected by the rate of formalin fixation. Blue markup indicates negatively stained cells, yellow 1+, orange 2+, and red 3+ positive cells. Heatmaps created using HALO AI spatial analysis workflow. Scale bars at 100 µm unless otherwise stated. Abbreviations: ATM, ataxia-telangiectasia-kinase; IHC, immunohistochemistry; PDX, patient-derived xenograft.
DDR Phosphorylated Biomarkers Are Highly Sensitive to Tissue Fixation Delays
To investigate how delays to formalin fixation affect tissue morphology and preservation of biomarker epitopes, we constructed a xenograft TMA containing samples with varying fixation conditions including cold ischemia times of 15 min, 30 min, 1 hr, 3 hr, and 6 hr (TMA 1). All IHC results are summarized in Table 5. Image analysis of the IHC stained TMA 1 highlighted the lability of particular phospho-epitopes when fixation is delayed, with pRAD50 and pKAP1 demonstrating a negative correlation between cold ischemia time and biomarker expression (Fig. 2A-D). Compared with the immediately fixed control sample, there was a 30% decrease in median pRAD50 tumor staining after just 15 min of cold ischemia and a 71% decrease in median tumor staining after 6 hr of cold ischemia (Fig. 2A and B). Although starting baseline levels of expression were lower for pKAP1, a similar decrease in tumor staining was observed following fixation delay, with a 44% decrease in median pKAP1 after 15 min of cold ischemia and a 78% decrease after 6 hr of cold ischemia (Fig. 2C and D). For ɣH2AX, there was no consistent loss of staining after any cold ischemia time; however, results were highly variable, with 3 hr and 6 hr of fixation delay resulting in a median 56% decrease and 16% decrease in positivity from the control, respectively (Fig. 2E and F).
Summary of IHC Image Analysis Results From TMA-1.

Percent positivity results from tumor regions analyzed for each biomarker (pRAD50, ɣH2AX, pKAP1, ATM, and c-MYC) from the optimally fixed cores. Subsequent columns of the table detail the percentage decrease from the optimal results, for image analysis results for all fixation conditions. Abbreviation: ATM, ataxia-telangiectasia-kinase; IHC, immunohistochemistry; TMA, tissue microarray.
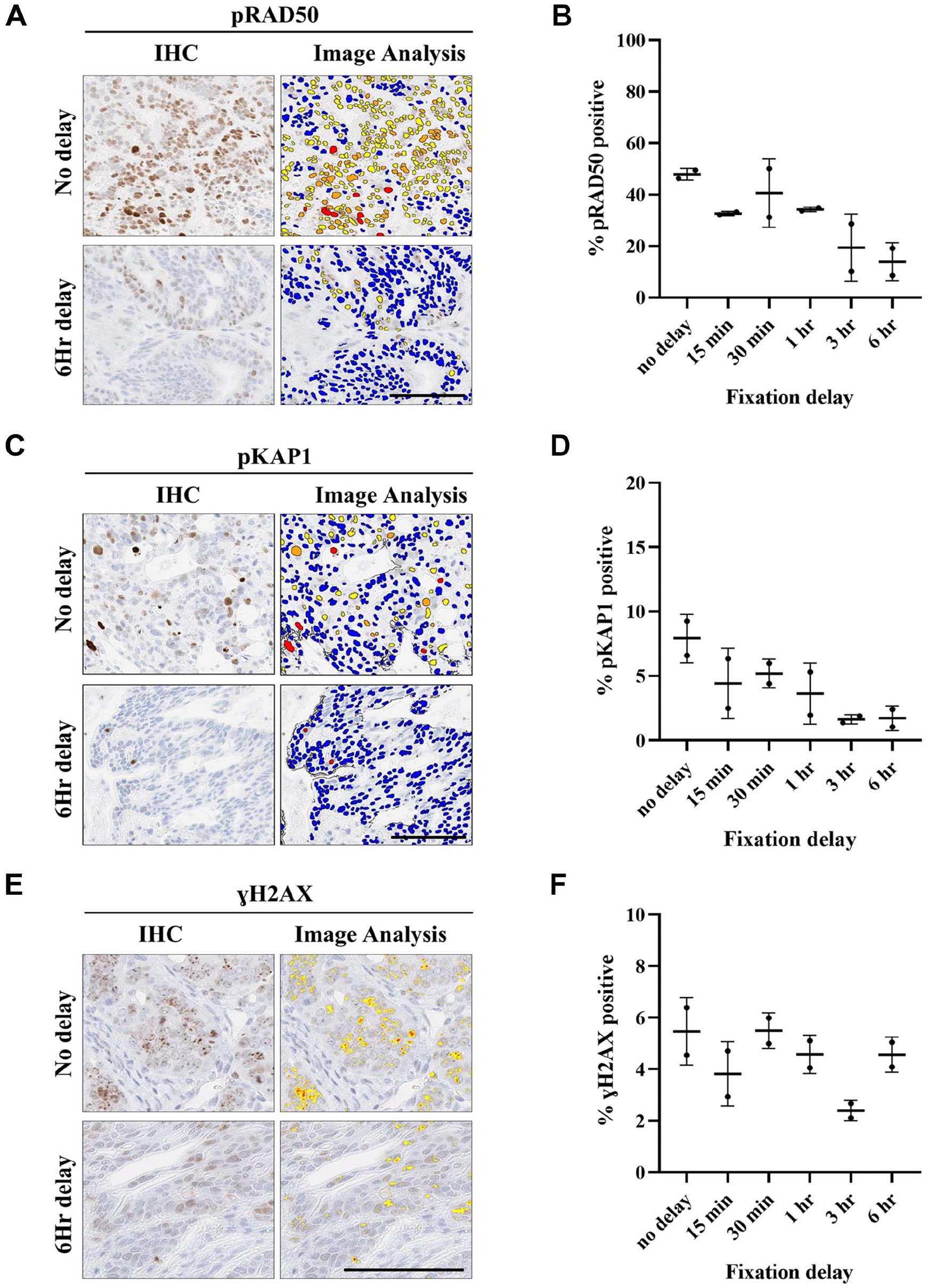
Phospho-epitope IHC staining results are affected by delay to fixation of as little as 15 min. In NCI-N87 xenograft samples, representative images of (A) pRAD50, (C) pKAP1, and (E) γH2AX staining and digital image analysis markup following immediate fixation (no delay) and fixation after a 6-hr delay. Image analysis results of change in percentage of positive tumor cell staining with increasing cold ischemia times (15 min 6 hr) for (B) pRAD50 and (D) pKAP1 and change in percentage of positive DAB-stained pixels per area of tumor tissue for (F) γH2AX. Blue markup indicates negatively stained cells, yellow 1+, orange 2+, and red 3+ positive cells. Data shown as median ± interquartile range. Scale bars at 100 µm. Abbreviation: IHC, immunohistochemistry.
Non-phosphorylated epitope ATM was less affected by delays to fixation, with median expression only dropping by 23% after the most severe cold ischemia condition of 6 hr, than the immediately fixed control (Fig. 3A and B). The c-MYC biomarker had lower baseline levels than ATM and appeared more sensitive to fixation delays than ATM but more robust than the phosphorylated targets, with a notable drop in median expression not observed until 1 hr of cold ischemia time (31% expression decrease from baseline) (Fig. 3C and D). This demonstrates biomarker-specific differences in epitope sensitivity to preanalytical factors such as cold ischemia time, with phosphorylated biomarkers being the most labile and variable.

Total protein biomarkers are more robust to fixation delays. In NCI-N87 xenograft samples, representative images of (A) total ATM and (C) cMYC staining and digital image analysis markup following immediate fixation (no delay) and fixation after a 6-hr delay. Image analysis results of change in percentage of positive tumor cell staining with increasing cold ischemia times (15 min 6 hr) for (B) ATM and (D) cMYC. Blue markup indicates negatively stained cells, yellow 1+, orange 2+, and red 3+ positive cells. Data shown as median ± interquartile range. Scale bars at 100 µm. Abbreviation: ATM, ataxia-telangiectasia-kinase.
Prolonged Tissue Fixation Has a Detrimental Effect on Some DDR Phosphorylated Epitopes
To determine whether prolonged tissue fixation of up to 4 weeks impacted IHC staining results, cores from TMA 1 treated with extended fixation times were analyzed by IHC and image analysis with the previously mentioned biomarkers (also summarized in Table 5). Compared with optimal conditions, there was little reduction in pRAD50 and pKAP1 biomarkers with extended fixation of 4 weeks (Fig. 4A to D). However, loss of staining was observed in ɣH2AX, with a 57% decrease in median staining after just 48 hr in formalin and 79% loss after 4 weeks in formalin, when compared with the optimal 24-hr fixed control (Fig. 4E and F). This result suggests that samples fixed for longer than 24 hr will not yield reliable ɣH2AX IHC results. The non-phosphorylated biomarkers ATM and c-MYC were stable following extended fixation times, with consistent staining even after 4 weeks in formalin (Fig. 5A to D). This suggests leaving clinical specimens for extended periods in formalin is less of a concern if samples are used to look at targets without posttranslational modifications.

Prolonged fixation induces loss of IHC staining signal in some phospho-epitopes. In NCI-N87 xenograft samples, representative images showing DAB staining after 4 weeks extended formalin fixation, compared with optimal fixation conditions (24 hr), for phospho-epitopes (A) pRAD50, (C) pKAP1, and (E) ɣH2AX after 4 weeks. Image analysis results showing change in percentage of positive tumor cell staining with increased time in fixative (24 hr, 48 hr, 1 week, 2 weeks, and 4 weeks) in phospho-epitopes (B) pRAD50 and (D) pKAP1 and change in percentage of positive DAB-stained pixels per area of tumor tissue for (F) ɣH2AX. Data are shown as median ± interquartile range. Scale bars at 100 µm. Abbreviation: IHC, immunohistochemistry.

Non-phospho-epitopes are unaffected by prolonged fixation. In NCI-N87 xenograft samples, representative images showing DAB staining after 4 weeks in extended formalin fixation, compared with optimal fixation conditions (24 hr), for total protein epitopes (A) ATM and (C) c-MYC. Image analysis results showing change in percentage of positive tumor cell staining with increased time in fixative (24 hr, 48 hr, 1 week, 2 weeks, and 4 weeks) for total protein epitopes (B) ATM and (D) cMYC. Data are shown as median ± interquartile range. Scale bars at 100 µm. Abbreviation: ATM, ataxia-telangiectasia-kinase.
Two-Step Fixation Method Improves DDR Phosphorylated Biomarker Preservation
Rapid, heat-induced fixation has been claimed to increase the yield of phosphorylated epitopes. 11 To test this with our DDR phosphorylated markers of interest, a second xenograft TMA (TMA 2) was created with matched samples fixed with either the standard 1-step protocol of 24 hr in formalin or the 2-step protocol (2 hr in cold formalin, 2 hr in hot formalin, finished with 24 hr in room temperature formalin). IHC staining with pRAD50 showed a 1.7-fold increase in expression when using the 2-step fixation method (Table 6); however, statistical analysis found the protocol used for fixation did not cause any significant differences in target expression (Table 6, Fig. 6A and B). However, a significant change was seen in ɣH2AX expression in the samples, increasing by 1.6-fold when following the 2-step method, (p=0.045) (Fig. 6A and C). These results support the claims that a 2-step fixation method could be beneficial for some DDR phosphorylated targets over the standard 1-step fixation method used in current clinical practice although biomarker expression changes were fairly modest.
Summary of IHC Image Analysis Results From TMA-2.
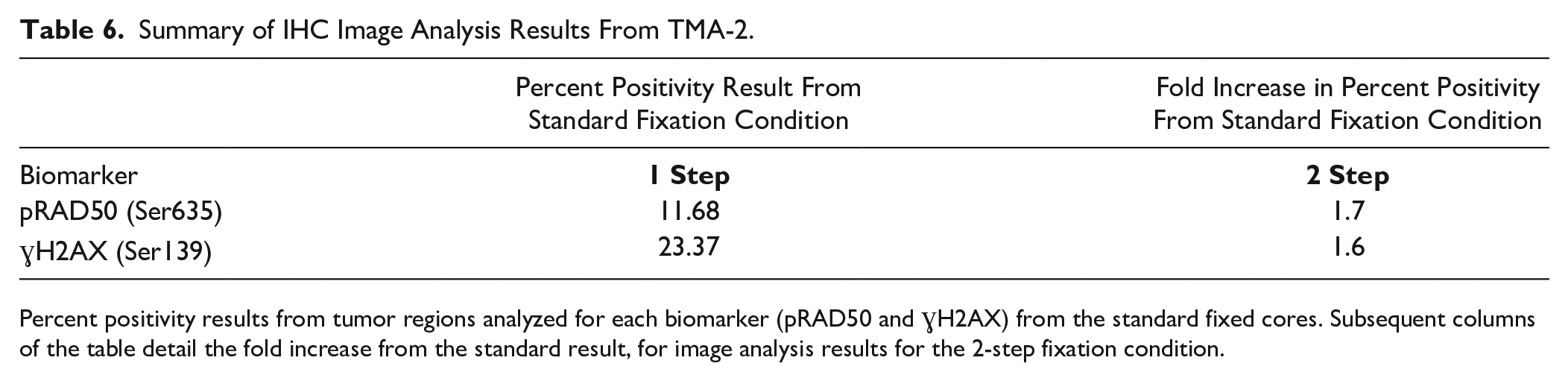
Percent positivity results from tumor regions analyzed for each biomarker (pRAD50 and ɣH2AX) from the standard fixed cores. Subsequent columns of the table detail the fold increase from the standard result, for image analysis results for the 2-step fixation condition.

Two-step fixation method improves the preservation of the ɣH2AX epitope, leading to more reliable downstream IHC staining and analysis. (A) In SUM149PT xenograft samples, representative images showing difference in DAB staining between paired samples fixed following 1-step or 2-step fixation methods. (B) Changes in percentage of positive tumor cell staining between the 1-step and 2-step fixation methods measured by digital image analysis, for pRAD50, and change in percentage of positive DAB-stained pixels per area of tumor tissue for ɣH2AX. Data shown as median ± interquartile range. *p=0.045 by paired t-test. Scale bars at 100 µm. Abbreviations: IHC, immunohistochemistry.
Discussion
We have focused on how best to preserve biomarker epitopes commonly used during the development of drugs that target the DNA damage response, including key phosphorylated biomarkers that are potentially more vulnerable to preanalytical factors than total protein biomarkers. We identified the most critical step for preservation of our DDR tissue antigens was to fix samples immediately upon collection, as even a short cold ischemia time of 15 min had a detrimental effect on the more labile phosphorylated targets like pRAD50 and pKAP1, and extended cold ischemia times of 3 hr or more reduced yield across all biomarkers tested. Exposure of tissues to extended fixation times was less problematic for downstream IHC analysis; however, this should still be avoided because there were interbiomarker variations in sensitivity to fixation longer than 24 hr. We found novel heated fixation methods may further preserve DDR phosphorylated biomarkers, but the benefits gained were relatively small considering the practical challenges for clinical sites to adopt this approach.
Preservation of tissue by appropriate fixation practices is not only important for the integrity of tissue and cell morphology but also for the reliability of biomarker staining in subsequent IHC analysis. Although CAP guidelines suggest cold ischemia time should be kept to less than 1 hr, 23 experimental studies have shown that cold ischemia times of up to 3 hr are acceptable for total protein markers such as ER, PR, HER2, HIF-1α, GLUT-1, Ki-67, and Bcl-2.7,25,26 Notably some biomarkers such as total PRAS40 and PD-L1 are very robust, even following 48 hr of cold ischemia.5,6,15 However, our data indicate the total protein biomarkers we tested (ATM and cMYC) are less robust and more in line with the CAP recommended guidelines to not go beyond 1 hr of cold ischemia during processing of clinical tissues. These differences are potentially due to increased sensitivity of the DDR IHC assays, as these are typically developed to differentiate patients into high and low expressors, rather than simply presence or absence of positive cells, as PD-L1, ER, and PR are typically used. There are also differences in the methodologies used to measure the cold ischemia cutoff point, with most other studies using clinical samples and manual pathology scoring. In contrast, we have used xenograft material, for tighter control of fixation conditions, and digital image analysis algorithms that allow increased sensitivity, and greater accuracy and precision, in detecting biomarker expression changes.
We build on existing research that shows phosphorylated epitopes are particularly sensitive to delays in tissue fixation.4,8 –14 The high lability of phospho-biomarkers is due to the presence of endogenous phosphatases that rapidly degrade these posttranslational modifications. Lack of blood flow and oxygen causes stress-induced biological changes in the tissue and can trigger signaling events that affect phosphorylation, 27 so the molecular composition of the tissue is changed by a delay to fixation after excision. 16 Our work aligns with a number of other studies that show phospho-epitopes such as pPRAS40, pEGFR, and pERK1/2 have loss of antigenicity after 1 hr of cold ischemia in clinical tissues.12,13 Consistently, pAKT(Ser473) is reported as the most labile with loss of staining after 30 min.8,10 However, often 1 hr is the minimum timepoint tested, which makes it difficult to draw direct comparisons to our phosphorylated DDR biomarkers that are lost by cold ischemia times as short as 15 min, even in studies using similar methodologies such as xenograft material and digital image analysis. 15
Our findings demonstrating edge effect with both phosphorylated and non-phosphorylated markers support concerns raised by others about inadequate preservation of epitopes during routinely fixed tissue resections 4 . Formalin is slow to penetrate tissue, estimated at around 1 mm per hour,28,29 resulting in loss of epitopes in the middle of large tissues. 30 Not only penetration rate but also routine clinical procedures can cause unavoidable fixation delays when working with tumor resections, for example, a drop in pAKT(Ser473) and pERK1/2 was evident in paired core-biopsies fixed immediately compared with resected material.4,9 Studies that have looked at how best to preserve phosphorylation in clinical tissues have focused on novel methods of fixation to speed up fixative penetration. These include using a 2-step approach of cold then hot formalin,11,31 which increased staining yield of phospho-markers such as pAKT(Ser473) and pPRAS40(Thr246). Others have used unique formulations of fixative such as biomarker and histology preservative (BHP) containing phosphatase inhibitors and permeation enhancers, improving IHC detection of phospho-markers including pERK(Thr202/Tyr204), pGSK3-α/β(Ser21/Ser9), and p38-MAPK, 16 or applied increased pressure (up to 15000 psi) to improve the rate of formaldehyde fixation. 30 Another study found the 2-step rapid fixation method better preserved pERK, pSRC, and in particular, pAKT(Ser473) and also recommended inclusion of a cold transport device with clinical specimens to log the exact time of fixation, as well as any discrepancies such as leaking during transit. 14 Although we note our findings are caveated by using relatively small tumor samples, we only saw small improvements in biomarker preservation using our adapted 2-step method of fixation compared with standard room temperature fixation. So, although the 2-step method could be helpful for low-prevalence targets or where detection of small changes in biomarker expression is needed, perhaps the practical challenges of implementing this in the clinic outweighs these modest gains in biomarker yield. Often these novel protocols are challenging to use at clinical sites where facilities to cool or heat formalin may not be readily available. As an alternative and to keep fixation practices standardized across clinical sites, we propose using core needle biopsy where possible or cutting tissue samples into slices of no more than 5-mm thickness and then immediately submerging in room-temperature formalin for 24 hr as the ideal fixation conditions.
Our results regarding length of formalin fixation for DDR biomarkers are in line with what others have found, suggesting a fixation time of 24 h is optimal and to cut up larger tissues to avoid the need for extended fixation times. 32 This is in concordance with the guidelines set out by the CAP, where the recommended fixation time for clinical tissues is 24 hr although fixation may vary between tissue types and up to 48 hr of fixation may be needed for larger samples. Typically, there is less concern around preanalytical factors caused by over-fixation than around cold ischemia time, with one study finding postmortem brain samples fixed for 14 years in formalin were still evaluable for neurodegenerative biomarkers, when incorporating specific antigen-retrieval methods into IHC practices. 33
Our results also highlight interbiomarker variations in sensitivity to formalin fixation variations, with ɣH2AX being more robust to fixation delays than pRAD50 and pKAP1 but sensitive to extended fixation times. As such, these findings should not be applied as “one size fits all” for markers with posttranslational modifications. Although less labile than the phospho-markers assessed, there were also clear differences for total protein markers, with c-MYC being more sensitive to fixation delays than ATM. For these reasons, we stress the importance of including individual fixation assessments in assay development and validation workflows that use FFPE samples for analysis, paying close attention to assays targeting phospho-epitopes, to understand the unique lability of each biomarker.
In summary, our results have continued to build on the existing knowledge that a key challenge to assessment of phosphorylated biomarker targets is their sensitivity to preanalytical factors compared with biomarkers without posttranslational modifications. For the first time, we have started to understand the differences between the lability of phosphorylated and non-phosphorylated epitopes involved in signaling the DNA damage response and crucially highlight the importance of immediate fixation upon excision from patient, the advantages of small tissue size to avoid edge effect, and the need to avoid extended fixation times beyond 24 hr. Where cold ischemia time is essential to allow for the dissection of resected specimens, we stress the importance of accurately recorded timings for caveating the use of labile phosphomarkers in downstream analysis. Novel fixation protocols may further preserve phospho-biomarker expression levels and should perhaps be considered where quantification of phosphorylated biomarkers is critical for drug development.
Supplemental Material
sj-docx-1-jhc-10.1369_00221554231174069 – Supplemental material for Epitope Lability of Phosphorylated Biomarkers of the DNA Damage Response Pathway Results in Increased Vulnerability to Effects of Delayed or Incomplete Formalin Fixation
Supplemental material, sj-docx-1-jhc-10.1369_00221554231174069 for Epitope Lability of Phosphorylated Biomarkers of the DNA Damage Response Pathway Results in Increased Vulnerability to Effects of Delayed or Incomplete Formalin Fixation by Elizabeth J. Wiseman, Jennifer I. Moss, James Atkinson, Hana Baakza, Emily Hayes, Sophie E. Willis, Paul M. Waring, Jaime Rodriguez Canales and Gemma N. Jones in Journal of Histochemistry & Cytochemistry
Supplemental Material
sj-tif-2-jhc-10.1369_00221554231174069 – Supplemental material for Epitope Lability of Phosphorylated Biomarkers of the DNA Damage Response Pathway Results in Increased Vulnerability to Effects of Delayed or Incomplete Formalin Fixation
Supplemental material, sj-tif-2-jhc-10.1369_00221554231174069 for Epitope Lability of Phosphorylated Biomarkers of the DNA Damage Response Pathway Results in Increased Vulnerability to Effects of Delayed or Incomplete Formalin Fixation by Elizabeth J. Wiseman, Jennifer I. Moss, James Atkinson, Hana Baakza, Emily Hayes, Sophie E. Willis, Paul M. Waring, Jaime Rodriguez Canales and Gemma N. Jones in Journal of Histochemistry & Cytochemistry
Supplemental Material
sj-tif-3-jhc-10.1369_00221554231174069 – Supplemental material for Epitope Lability of Phosphorylated Biomarkers of the DNA Damage Response Pathway Results in Increased Vulnerability to Effects of Delayed or Incomplete Formalin Fixation
Supplemental material, sj-tif-3-jhc-10.1369_00221554231174069 for Epitope Lability of Phosphorylated Biomarkers of the DNA Damage Response Pathway Results in Increased Vulnerability to Effects of Delayed or Incomplete Formalin Fixation by Elizabeth J. Wiseman, Jennifer I. Moss, James Atkinson, Hana Baakza, Emily Hayes, Sophie E. Willis, Paul M. Waring, Jaime Rodriguez Canales and Gemma N. Jones in Journal of Histochemistry & Cytochemistry
Footnotes
Appendix
Summary of Experimental Conditions and Main Findings for Biomarkers Tested in the Present Study.
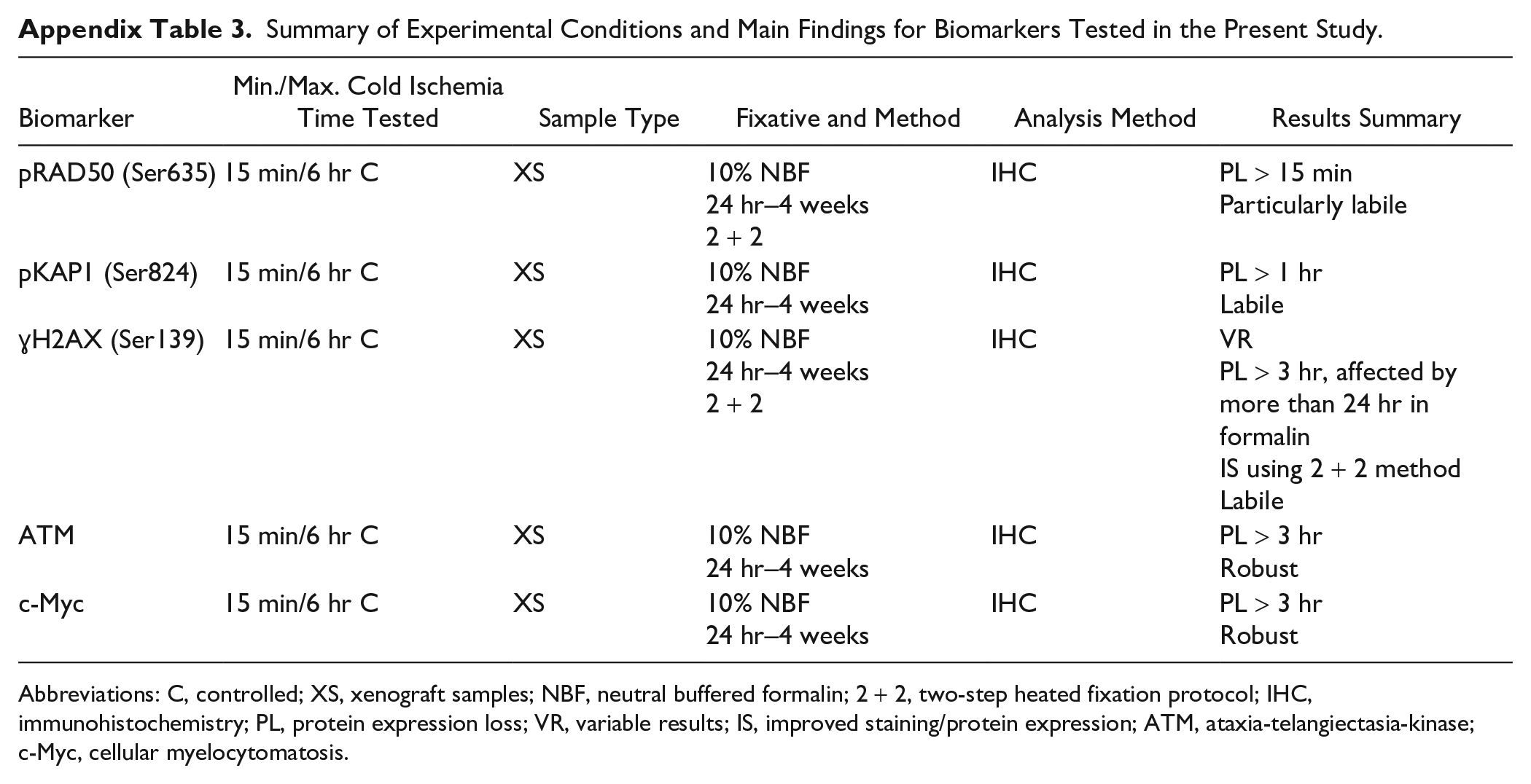
| Biomarker | Min./Max. Cold Ischemia Time Tested | Sample Type | Fixative and Method | Analysis Method | Results Summary |
|---|---|---|---|---|---|
| pRAD50 (Ser635) | 15 min/6 hr C | XS | 10% NBF
24 hr–4 weeks 2 + 2 |
IHC | PL > 15 min
Particularly labile |
| pKAP1 (Ser824) | 15 min/6 hr C | XS | 10% NBF
24 hr–4 weeks |
IHC | PL > 1 hr
Labile |
| ɣH2AX (Ser139) | 15 min/6 hr C | XS | 10% NBF
24 hr–4 weeks 2 + 2 |
IHC | VR
PL > 3 hr, affected by more than 24 hr in formalin IS using 2 + 2 method Labile |
| ATM | 15 min/6 hr C | XS | 10% NBF
24 hr–4 weeks |
IHC | PL > 3 hr
Robust |
| c-Myc | 15 min/6 hr C | XS | 10% NBF
24 hr–4 weeks |
IHC | PL > 3 hr
Robust |
Abbreviations: C, controlled; XS, xenograft samples; NBF, neutral buffered formalin; 2 + 2, two-step heated fixation protocol; IHC, immunohistochemistry; PL, protein expression loss; VR, variable results; IS, improved staining/protein expression; ATM, ataxia-telangiectasia-kinase; c-Myc, cellular myelocytomatosis.
Acknowledgements
The authors thank Jack Robertson for his digital image analysis guidance and Benjamin Phillips for his statistical support.
Competing Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The employees of AstraZeneca are clearly stated in author affiliations.
Author Contributions
All authors have contributed to this article as follows: concptualization of the study (GNJ), interpretation of data (GNJ), writing the manuscript (GNJ, EJW), performing and analysis of IHC experiments and visualizing data (GNJ, EJW, HB, EH, SEW), pathology evaluation and review (JRC, PMW), in vivo experiments and study materials (JIM, JA).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors affiliated with AstraZeneca were provided financial support in the form of salaries and research materials by AstraZeneca.
Ethics Approval
Human tissues described in this article were obtained with fully informed consent and transferred to AstraZeneca. AstraZeneca has a governance framework and processes in place to ensure that commercial sources have appropriate patient consent and ethical approval in place for collection of the samples for research purposes including use by for-profit companies. The AstraZeneca Biobank in the UK is licensed by the Human Tissue Authority (license no. 12109) and has National Research Ethics Service Committee (NREC) approval as a Research Tissue Bank (RTB) (REC no. 17/NW/0207) which covers the use of the samples for this project. Tissue samples were obtained from in vivo studies that were run in the UK in accordance with all relevant ethical regulations for animal testing and research, including UK Home Office legislation, the Animal Scientific Procedures Act (ASPA) 1986, AstraZeneca’s Global Bioethics Policy, and the Home Office Project Licenses P0EC1FFDF and PP3292652, which received ethical review and approval through the AstraZeneca Ethical Review Process.
Data Availability
All data are provided in the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.