
Abstract
Non-ampullary duodenal adenocarcinoma (DAC) is a rare malignancy. Little information is available concerning the histopathological prognostic factors associated with DAC. Carbonic anhydrases (CAs) are metalloenzymes catalyzing the universal reaction of CO2 hydration. Isozymes CAII, CAIX, and CAXII are associated with prognosis in various cancers. Our aim was to analyze the immunohistochemical expressions of CAII, CAIX, and CAXII in normal duodenal epithelium, duodenal adenomas, and adenocarcinoma and their associations with clinicopathological variables and survival. Our retrospective study included all 27 DACs treated in Oulu University Hospital during years 2000–2020. For comparison, samples of 42 non-ampullary adenomas were collected. CAII expression was low in duodenal adenomas and adenocarcinoma. CAIX expression in adenomas and adenocarcinoma was comparable with the high expression of normal duodenal crypts. Expression patterns in carcinomas were largely not related to clinicopathological features. However, low expression of CAII associated with poorer differentiation of the tumor (p=0.049) and low expression of CAIX showed a trend for association with nodal spread, although statistical significance was not reached (p=0.091). CAII and CAIX lost their epithelial polarization and staining intensity in adenomas. CAXII expression was not detected in the studied samples. CAs were not associated with survival. The prognostic value of CAII and CAIX downregulation should be further investigated. Both isozymes may serve as biomarkers of epithelial dysplasia in the duodenum.
Introduction
Non-ampullary duodenal adenocarcinoma (DAC) is a rare malignancy constituting only 1.5% of all gastrointestinal cancers but 55% of all small bowel carcinomas. 1 The incidence of DAC has been rising during the last decades, as shown in population-based studies from the Netherlands 2 and Sweden. 3 According to single-center retrospective reports, the 5-year overall survival varies between 38% and 57% after surgery with curative intent.4,5 Histological subtype, regional nodal positivity, and American Joint Committee on Cancer (AJCC) stage have been associated with overall survival.6,7 However, due to the rarity of the disease, very limited information is available regarding histological prognostic factors associated with DAC.
Carbonic anhydrases (CAs) are zinc-containing metalloenzymes catalyzing the reversible hydration of CO2 to bicarbonate and protons. Thus far, 12 catalytically active isoforms have been identified in humans. 8 Cytosolic CAII and membrane-bound isoforms CAIX and CAXII are considered tumor-associated CAs. 8 Although their basic function is to regulate pH homeostasis of the body, 9 they have other important physiological roles, such as regulation of glycolysis and CO2 transport. 9
Nearly all cancer types use glycolytic metabolism in both the presence and absence of oxygen, 10 leading to the accumulation of lactic acid and increased pCO2, which in combination acidify the extracellular milieu. 11 Tumor acidity and hypoxia, the latter resulting from malignant cells rapidly outgrowing their blood supply, are the two conjoined key features of cancer progression.11–14 CAII, CAIX, and CAXII all contribute to acidification of the tumor microenvironment and support increased glycolysis in tumors. Cytosolic CAII regulates intracellular pH and lactate flux via collaboration with monocarboxylate transporters (MCTs) 1 and 4 and Na+/H+-transporter-1 (NHE-1).15,16 Extracellular acidosis is primarily generated by extracellular-facing CAIX and CAXII, which catalyze CO2 hydration and build up hypercapnic acidosis. 13 CAIX and CAXII also maintain the alkaline intracellular pH of tumor cells and thus preserve their viability, presumably in association with membrane-bound ion transporters. 17 Thus, pH regulation in tumor cells and oncogenic metabolism are considered CA-dependent processes. 11
CAII is the most widely distributed CA isoform of the human body and present throughout the gastrointestinal tract, including the small intestine and duodenum. 18 Under physiological conditions, the role of CAII in the duodenum is likely related to the luminal chemosensing process through which CAII-dependent intracellular acidification and HCO−3 secretion are triggered.19,20 In several cancers, such as pancreatic and gastric adenocarcinomas, CAII downregulation associates with poor prognosis.21,22 The isoforms CAIX and CAXII are hypoxia inducible, and mainly regulated by hypoxia-inducible factor 1α (HIF-1α). 17 The expression of CAIX is very limited in normal human tissues, 18 but it is present in the gastric and intestinal epithelia, with intensive expression in the duodenum. 23 High CAIX expression is associated with poor prognosis in many solid tumors.17,24–27 In contrast, CAXII is present in many normal human tissues, such as the breast, endometrium, large intestine, and renal epithelia,28–31 but absent in the human duodenum. 30 Nevertheless, CAXII is expressed in several cancers,32,33 although it is not necessarily found in the corresponding normal tissues, 34 and has a variable association with prognosis. 31
DAC develops through an adenoma-adenocarcinoma sequence.35,36 The expression of tumor-associated CAs in duodenal adenomas and adenocarcinoma is poorly documented; only one study 37 on the role of CAIX in DAC is available. The aim of our current study was to describe in detail the expression patterns of CAII, CAIX, and CAXII in the normal duodenal epithelium, duodenal adenoma and adenocarcinoma and to clarify their associations with clinicopathological variables and survival in DAC. Finally, to elaborate the relationship between CA expression with hypoxia and hypoxia-related aberration of metabolism in the tumor microenvironment in DAC, we performed additional immunohistochemistry on the hypoxia marker HIF-1α and two downstream hypoxic markers related to tumor metabolism, MCT4 (monocarboxylate transporter 4) 38 and GLUT1 (glucose transporter 1). 39
Materials and Methods
Study Design
We designed a retrospective cohort study from a single-institution tertiary care hospital in Oulu, Finland. All 27 patients diagnosed with sporadic, duodenal non-ampullary adenocarcinoma at Oulu University Hospital during 2000–2020 were identified and included. For comparison and to evaluate CA expression along the adenoma-carcinoma sequence, we assembled 42 cases of duodenal non-papillary adenomas from 2014 to 2015, including specimens from surgical and endoscopic resections and biopsy material.
Data Collection
The use of samples and paraffin blocks, as well as data inquiry, was approved by the Oulu University Hospital Ethics Committee (EETTMK: 81/2008) and by the National Supervisory Authority for Welfare and Health (VALVIRA; Approval No. 10832/06.01.03.01/2014). All procedures performed in our study were in accordance with the ethical standards of the Oulu University institutional research committee and with the 1964 Declaration of Helsinki and its later amendments. Patient consents for participation or publication could be waived due to data anonymization. No experiments regarding animals were performed.
Hematoxylin and eosin–stained sections from paraffin-embedded tissue specimens were collected from the archives of the Department of Pathology, Oulu University Hospital, Finland. After re-evaluation, sufficient biopsy samples or paraffin tissue blocks for immunohistochemistry of 22 DAC and 35 adenoma cases were available, which then comprised the final study group. The cohort included 16 cancer patients with samples from surgical specimens and 6 cancer patients with only biopsy material available for analyses. Duodenal adenomas included 25 cases with low-grade dysplasia (LGD) and 10 cases with high-grade dysplasia (HGD), all with the tubular adenoma subtype. Normal duodenal epithelia included in the samples were evaluated for comparison. Ampullary and pancreatic cancers were excluded by carefully assessing the endoscopic footage, patient records, original pathologist’s assessment, and reassessed histological findings by an experienced gastrointestinal pathologist (T.J.K.). Survival data available until the end of 2019 were acquired from Statistics Finland. Other relevant clinical data were collected from patient records at Oulu University Hospital.
Histopathological and Immunohistochemical Analyses
The samples originally used for routine clinical decision-making were retrieved and used in this study. A tissue block or biopsy sample most representative of the tumor component was selected for immunohistochemistry. All tumors were restaged according to the AJCC Cancer Staging Manual 8th edition for small intestinal adenocarcinoma. 40 As pathological stage could only be determined for the operated patients (n=16), we also re-evaluated the pretreatment computed tomographies for clinical stage. The WHO Classification for Tumours 5th edition 41 was used for histopathological classification and regrading by an expert gastrointestinal pathologist (T.J.K.). Immunohistochemical staining of CAs was performed at the Faculty of Medicine and Health Technology, Tampere University, Finland. Immunohistochemistry was conducted using polyclonal rabbit sera against human CAII and CAXII and a monoclonal anti-human CAIX antibody (M75), as described for polymer-based detection by Viikila et al. 42 The antibodies have been previously characterized and shown to be specific for each isozyme.28,43,44 The stained sections were digitalized using NanoZoomer S60 (Hamamatsu Photonics; Hamamatsu, Japan). HIF-1α, MCT4, and GLUT1 immunostainings were performed in the Department of Pathology, University of Oulu, Oulu, Finland, and conducted with rabbit polyclonal antibodies for HIF-1α (NB 100-449; Novus Biologicals), MCT4 (H-90; cat. no. sc-50329; Santa Cruz Biotechnology), and GLUT1 (Ref. 355A-16; Cell Marque), all with a high-temperature antigen retrieval of the sections with citrate buffer, and detection with Dako Envision. 45
For all immunostainings, immunoreactivity in the lesions was analyzed by two independent researchers (M.N., H.H.) who were blinded to the clinical data. Internal positive controls were used in the assessment of staining intensity: pancreatic acinar cells for CAIX and CAXII, and red blood cells, and pancreatic ductal cells for CAII. The presence, and intensity of staining (absent, weak, moderate, strong; 0–3), and the proportion (percentage) of stained cells (0–100%) were separately assessed in normal epithelial cells, in the epithelium in LGD and HGD, and in the bulk, and invasive front of the carcinoma. Some cases of HGD showed areas fulfilling the criteria of LGD, and in some adenocarcinomas, an adjacent area classified as dysplasia was present. These lesions were annotated by an experienced pathologist (T.J.K.) and assessed as separate lesions. For each lesion, the mean of the independent evaluations was used if the evaluations differed by at most 1 for the intensity assessment score or less than 30% for the percentage assessment. Consensus was reached by re-evaluation if the discrepancy was wider. The intensity values were multiplied by the percentage of positive cells to obtain a histoscore (0–300), 46 which was further dichotomized into two equally sized groups by the median value for each CA isozyme.
Statistical Analysis
The Chi-square test was used to obtain p values when comparing categorical variables. The threshold for significance was set at p<0.05. Cohen’s kappa was calculated to analyze interobserver agreement, where values between 0.01 and 0.20 indicated none to slight; 0.21 and 0.40, fair; 0.41and 0.60, moderate; 0.61 and 0.80, substantial; and 0.81 and 1.00, almost perfect agreement. 47 One-way ANOVA with Tukey’s post hoc analysis was employed to compare differences between independent groups with continuous variables. The Kaplan–Meier method was applied to compare survival between groups and the log-rank test to analyze significant differences between groups. Multivariable analysis between groups was performed with a Cox regression model with the following covariates: sex (female/male), age (continuous), grade (1, 2, 3), and stage (I–II, III–IV) according to the 8th edition of the AJCC Cancer Staging Manual for small intestinal adenocarcinoma. 40 Hazard ratios (HRs) with 95% confidence intervals (CIs) were calculated. The statistical analysis was performed with IBM SPSS Statistics 24.0 (IBM Corp.; Armonk, NY).
Results
The patients’ median age was 68 years (range, 39–78 years), and 12 (50%) of 24 died during follow-up. The median follow-up time of the surviving patients was 50 months (range, 8–225 months). The patient demographics are summarized in Table 1.
Clinicopathological Variables.
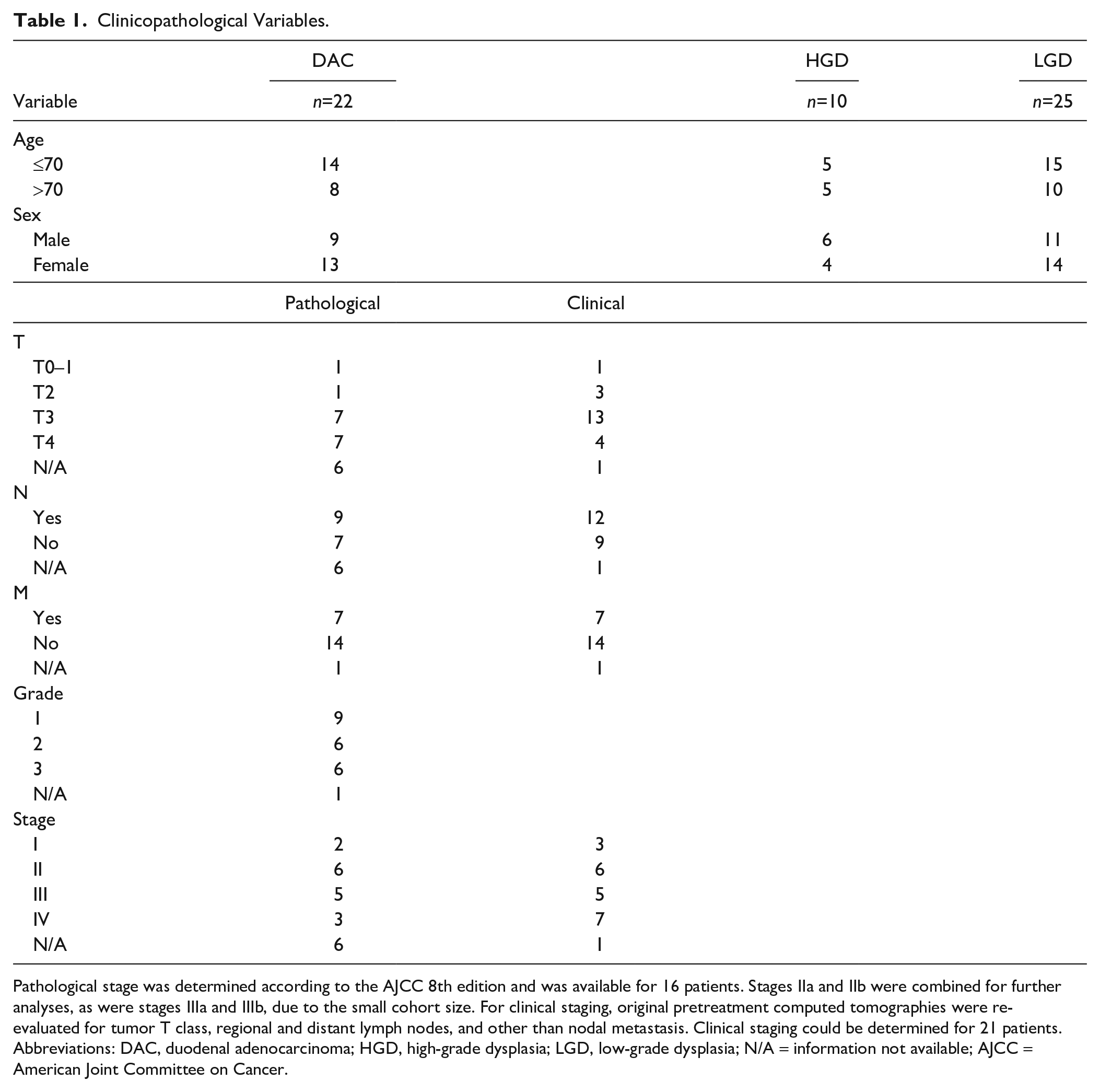
Pathological stage was determined according to the AJCC 8th edition and was available for 16 patients. Stages IIa and IIb were combined for further analyses, as were stages IIIa and IIIb, due to the small cohort size. For clinical staging, original pretreatment computed tomographies were re-evaluated for tumor T class, regional and distant lymph nodes, and other than nodal metastasis. Clinical staging could be determined for 21 patients. Abbreviations: DAC, duodenal adenocarcinoma; HGD, high-grade dysplasia; LGD, low-grade dysplasia; N/A = information not available; AJCC = American Joint Committee on Cancer.
Expression Patterns of CAII, CAIX, and CAXII in the Normal Duodenal Epithelium, Dysplasia, and Duodenal Adenocarcinoma
Substantial interobserver agreement was achieved in the assessment of immunohistochemical staining with Cohen’s kappa of 0.71. The characteristic expression patterns and histoscores of CAII and CAIX in the normal duodenal epithelium, LGD, HGD, and the carcinoma bulk and invasive front area are described in Figs. 1 to 4 and Table 2. The expression of CAXII was completely absent in all the lesions examined.
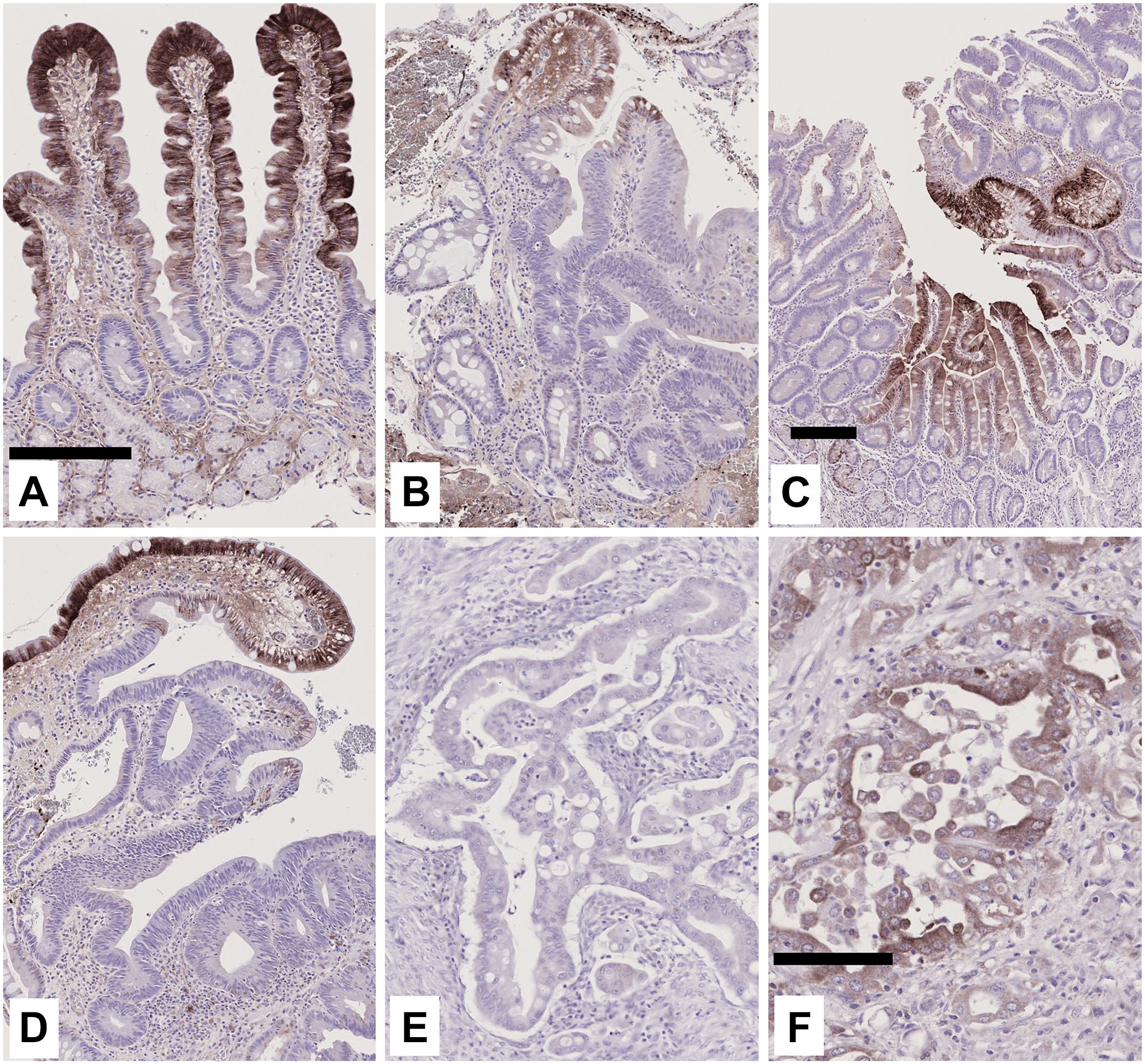
Characteristic immunohistochemical expression of CAII in duodenal lesions. In the normal duodenal epithelium (A), cytosolic expression of CAII is confined to the upper region of the villi; staining in the crypts, and Brunners’ glands is faint and occasional. In regions of low-grade adenoma (B, C), typical, strong staining in the surface region is lost, thus clearly denoting the dysplastic area in the epithelium. In high-grade dysplastic adenomas (D), expression is diffuse and weak, similar to that in low-grade adenomas. The adenocarcinoma bulk (E), and invasive front (F) show mostly weak overall expression. Scale bar sizes: (A) = (B), (D), (E) 100μm; (C) 100μm; (F) 200μm.
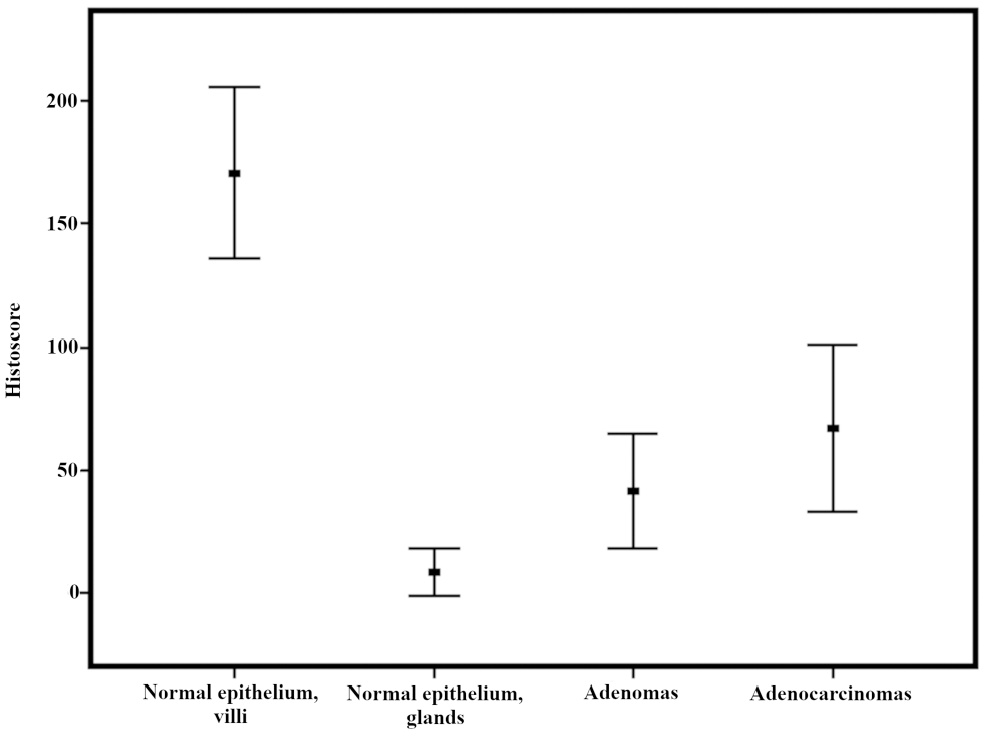
Histoscore of CAII immunohistochemical staining in duodenal lesions. See materials and methods for details.
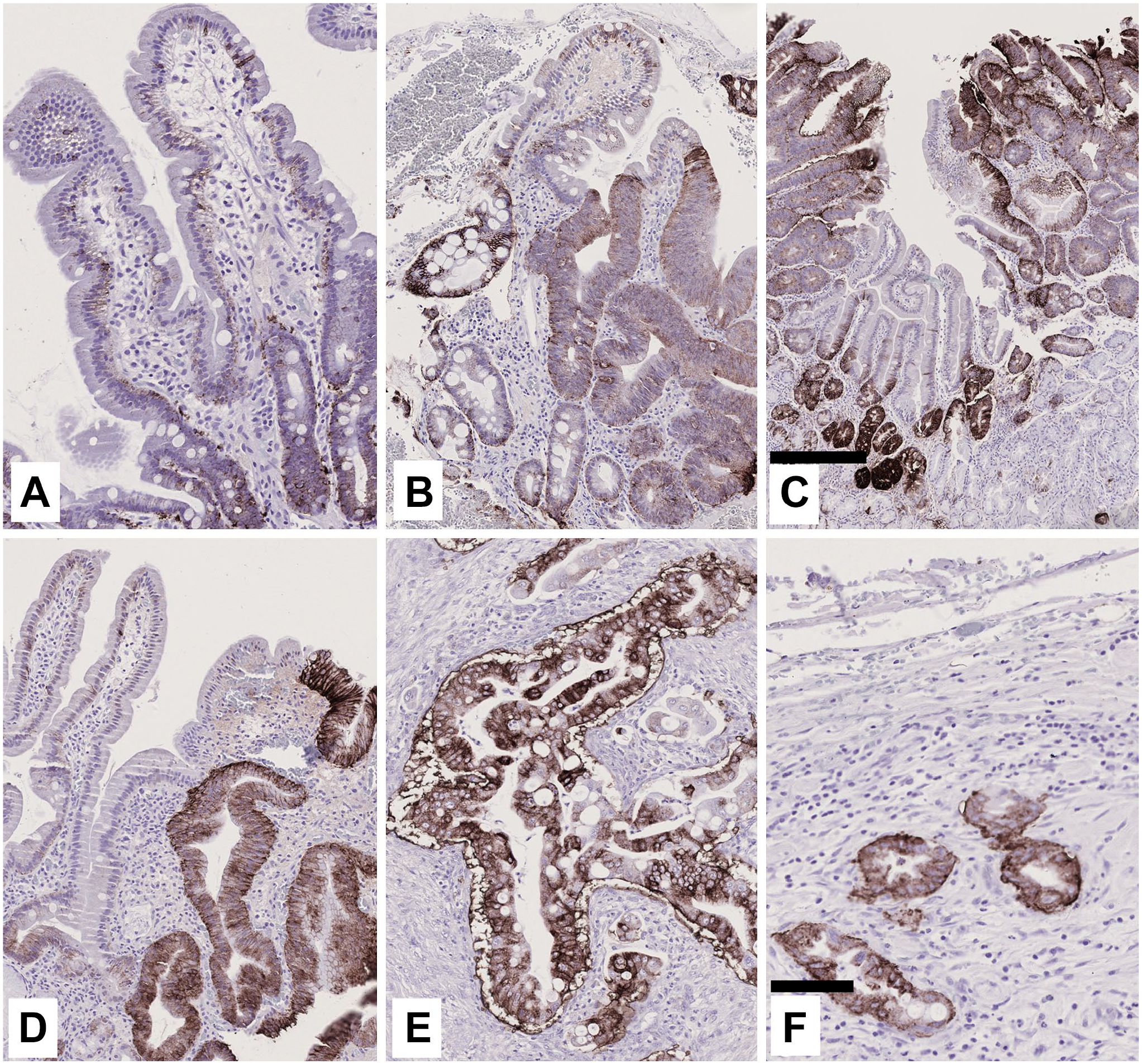
Characteristic immunohistochemical expression of CAIX in duodenal lesions. The normal duodenal epithelium (A) expresses CAIX almost exclusively in the basolateral cell membranes in duodenal crypt cells. In low (B, C), and high-grade (D) adenomas, positive staining marks the dysplastic regions in the same manner as CAII, but with an inverse staining order: moderately strong CAIX expression is seen throughout the dysplastic region, including the normally unstained upper villi. The adenocarcinoma bulk (E), and invasive front region (F) typically show diffuse staining with strong intensity, similar to that in adenomas. Scale bar sizes: (A), (B), (D), (E), (F) 100μm; (C) 300μm.
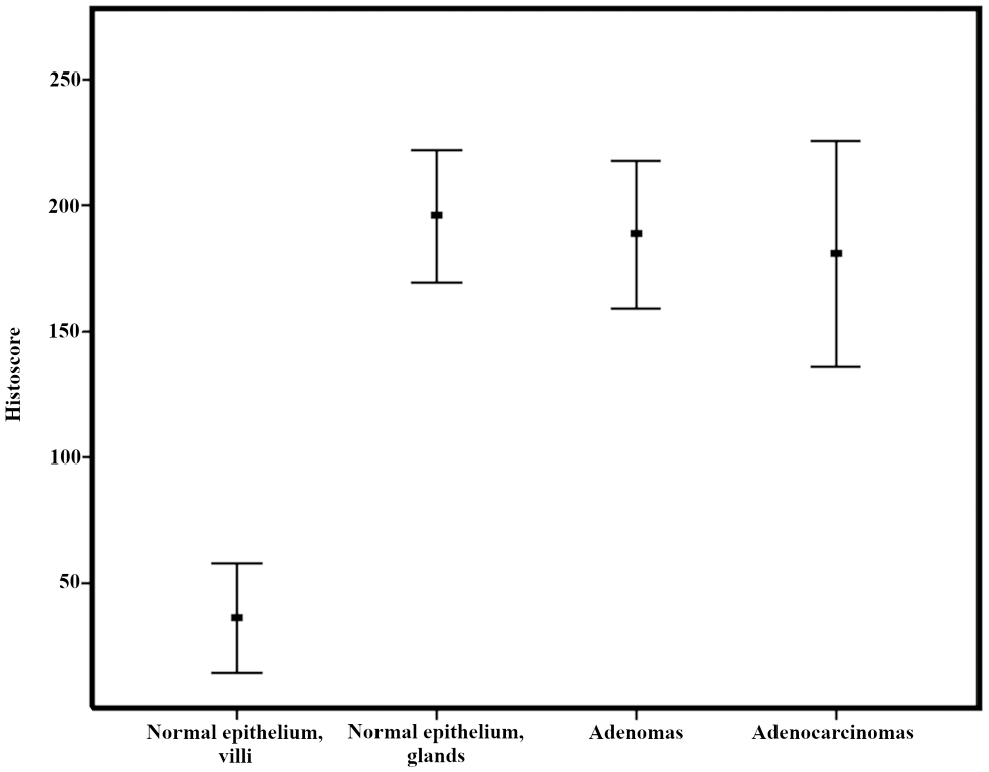
Histoscore of CAIX immunohistochemical staining in duodenal lesions.
Expression Levels of CAII and CAIX in the Normal Duodenal Epithelium, Adenoma, and Adenocarcinoma.
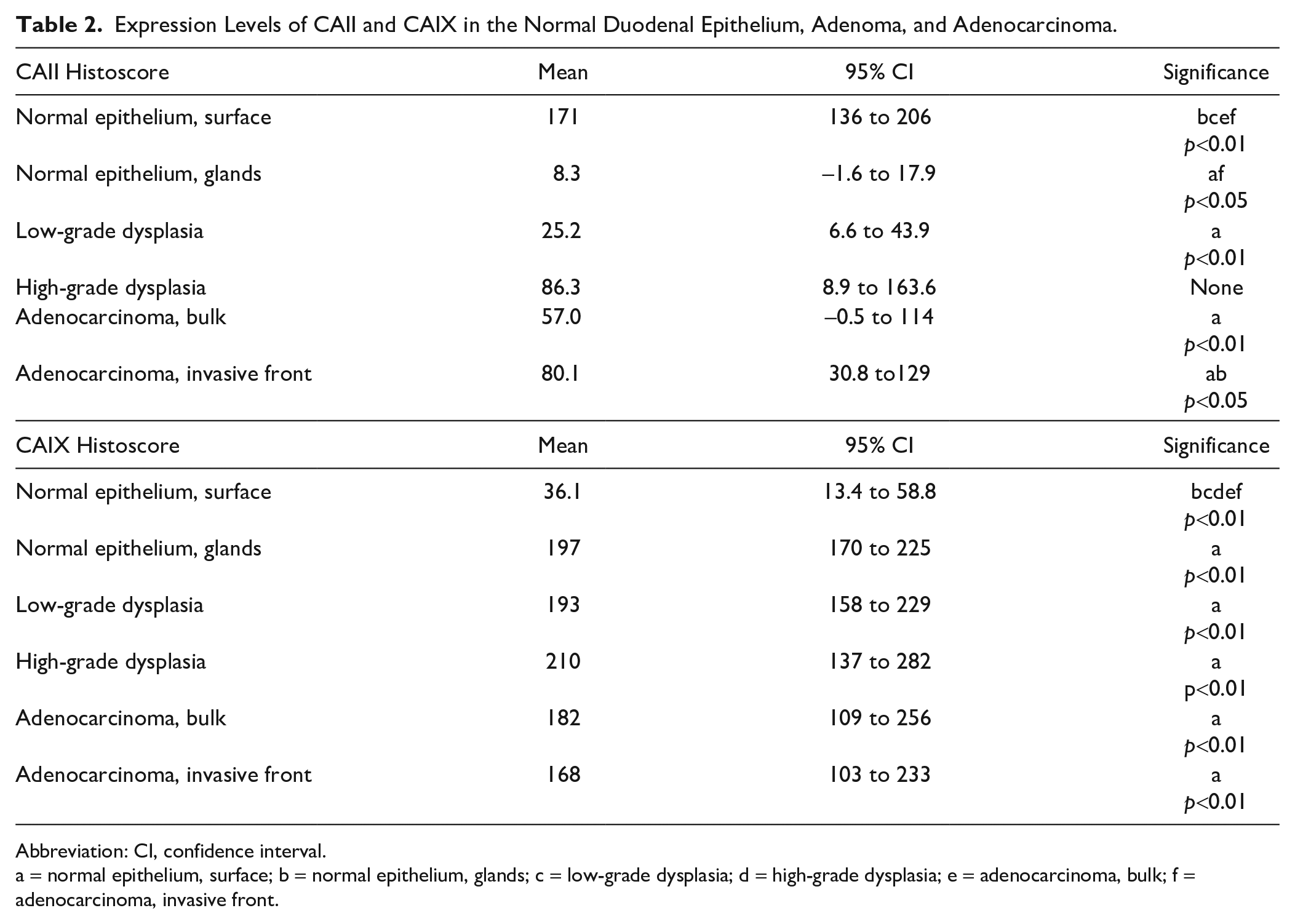
Abbreviation: CI, confidence interval.
a = normal epithelium, surface; b = normal epithelium, glands; c = low-grade dysplasia; d = high-grade dysplasia; e = adenocarcinoma, bulk; f = adenocarcinoma, invasive front.
The expression of CAII was generally cytoplasmic, with only occasional and faint staining in nuclei. In the normal duodenal epithelium, staining was present in all cells of the villus, but it was more intense in the villus tip region (Fig. 1A). The epithelium in duodenal crypts was virtually unstained, and only occasional cells in Brunner’s glands were positive (Fig. 1A). CAII staining in adenomas was less intense and extensive than that in normal villi (Table 2; Fig. 2), and the expression extended from the surface to deeper parts. Moreover, staining intensity was non-significantly higher in adenomas with HGD (Fig. 1D) than in adenomas with LGD (Fig. 1B and C). In DACs, positive staining for CAII (histoscore >0) was present in 54% of cases with weak to moderate intensity and extent. In carcinomas, CAII expression showed no polarization (Figs. 1E and F and 2; Table 2). CAII expression in carcinoma cells was weaker than that in the normal villus epithelium, but comparable to the levels in adenomas (Table 2; Fig. 2). CAII expression tended to be slightly weaker in the bulk (p=NS; Table 2; Fig. 1E) than in the invasive front (Fig. 1F) of the carcinoma. In the invasive front, the expression was significantly stronger than in the normal crypt epithelium, and weaker than in the villous epithelium (Fig. 1A and F, Table 2).
CAIX staining was confined to the basolateral cell membranes of expressing cells. The normal duodenal epithelium showed an inverse staining pattern for CAIX (Fig. 3A) compared with that of CAII (Fig. 1A). The epithelial cells lining the villi were negative for CAIX, but the crypt epithelium showed strong membrane-bound expression (Figs. 3A and 4). In the Paneth cells, both the cytoplasm and granules were CAIX-negative, but adjacent epithelial cells in the crypt bases always showed positive staining in their lateral membranes. Therefore, by resolution provided in light microscopy, it was not possible to conclude what was the contribution of Paneth cells to the positive CAIX staining between them and the adjacent cells. Positive expression comparable to that of the normal crypt epithelium was observed in LGD (Fig. 3B and C) and HGD (Fig. 3D). Resembling the pattern of CAII expression, CAIX staining in the dysplastic regions was detected throughout the lesion and was also present in the superficial parts facing the lumen (Fig. 3B–D). Positive staining for CAIX (histoscore >0) was present in 70% of DAC cases, whereas 30% were entirely negative for CAIX (histoscore = 0).
CAIX expression in adenocarcinoma tended to be lower than that in dysplastic lesions but remained moderately strong and pervasive in both the bulk (Fig. 3E) and invasive front (Fig. 3F) (Table 2).
As there was no significant difference between the tumor bulk and invasive front for CAII and CAIX expressions (Table 2), further analyses were based on invasive front expression.
Association of CA Expression With Clinicopathological Variables and Survival in DAC
In DAC, low CAII histoscore was associated with higher grade of tumor differentiation (p=0.049; Table 3). Low CAIX histoscore showed a trend for association with the presence of regional lymph node metastasis (p=0.091), but statistical significance was not reached. CAII and CAIX expression levels showed no other significant associations with clinicopathological variables, nor with overall or disease-specific mortality rates. Similarly, cases negative for CAIX (histoscore = 0; n=7) did not differ from those positive for CAIX expression (histoscore >0; n=17) with respect to clinicopathological features or prognosis (data not shown).
Associations Between CA Expression Levels and Clinicopathological Variables of DAC.
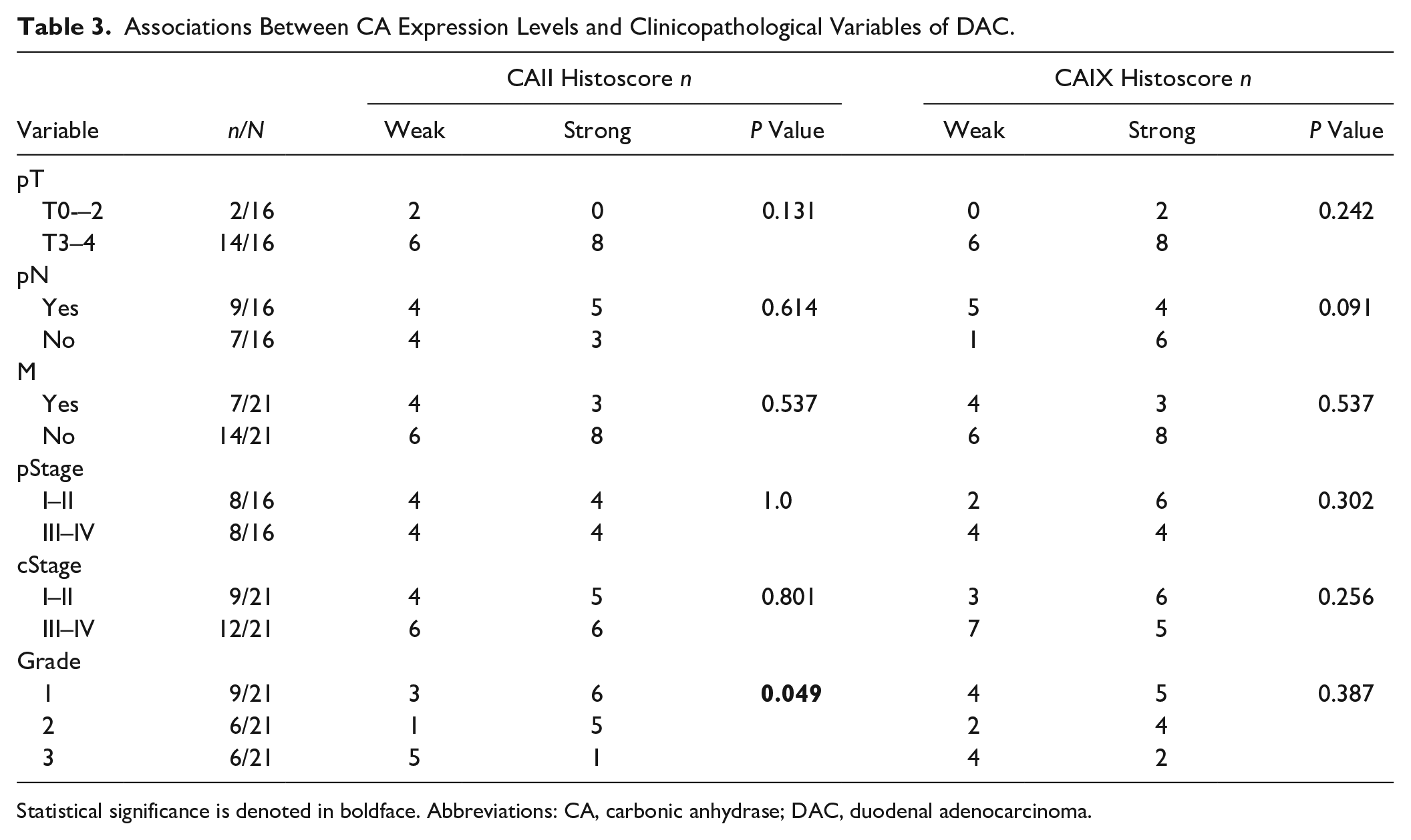
Statistical significance is denoted in boldface. Abbreviations: CA, carbonic anhydrase; DAC, duodenal adenocarcinoma.
Assessment of Hypoxia Markers in DAC
All the studied hypoxic markers, HIF-1α, GLUT1 and MCT4, were expressed in normal duodenal epithelium (Supplementary Fig. 1 and Supplementary Table 1). HIF-1α staining in DAC was both nuclear and cytoplasmic. The expression was moderately strong and diffuse in DAC but did not differ significantly from expression levels in the normal duodenum. GLUT1 was strongly expressed in the majority of carcinomas, when compared to normal epithelium (p<0.001). GLUT1 staining was seen in the membranes and cytoplasm. The membranous expression of MCT4 was moderately strong in carcinomas and significantly upregulated (p< 0.001) in comparison with normal epithelium. Although the hypoxic markers were all expressed in DAC, histoscores of HIF-1α, MCT4, and GLUT1 were neither correlated with each other nor with the expression levels of any of the studied CAs (Spearman’s rank order correlation). Furthermore, HIF-1α, MCT4, and GLUT1 expressions did not associate with the clinicopathological parameters or survival in DAC (data not shown).
Discussion
Our study showed that CAII and CAIX are expressed in the normal duodenal epithelium in characteristic patterns: CAII was mainly expressed in the villous epithelium, whereas CAIX was expressed in crypts. Both enzymes were found to be expressed in duodenal adenomas and adenocarcinomas. CAII expression levels were lower in adenoma and adenocarcinoma than in the normal villous epithelium. CAIX expression in tumors was comparable to the levels in the normal crypt epithelium, with no significant differences between adenoma and adenocarcinoma. Our case series, representing all available cases of primary non-ampullary DACs over a 20-year timespan in our center, still consisted of only 22 patients. This limited size of the series possibly explains why expression patterns of CAII and CAIX mostly did not reach significant associations with clinicopathological features. Low CAII expression was, however, significantly associated with poorer carcinoma differentiation, whereas low CAIX expression showed a trend for association with regional nodal spread.
The expression patterns described herein for CAII and CAIX in the normal duodenal epithelium are in agreement with previous observations.23,48 By enhancing HCO−3 extrusion, both CAs have been suggested to augment intracellular duodenal epithelial defense mechanisms against massive gastric acid and CO2 load.49,50 It has been proposed that the main function of CAII in the duodenum might involve “luminal sensing” of protons and initiating consequent neutralization and CO2 conversion.20,51,52 Such functions are plausible considering the localization of the isozyme predominantly in the luminal half of the villous epithelium. CAIX is characteristically present in the fastest proliferating cells of the crypts along the length of the human intestine, correlating with Ki-67 expression.23,53 The expression pattern was repeated in the duodenum, as shown by our results. In addition to a potential role in cell proliferation under physiological conditions, other functions have been suggested for CAIX. In studies involving knockout mice,54,55 Car9−/− mice exhibited considerable gastric pit cell hyperplasia and glandular atrophy, and the authors postulated that the enzyme may contribute to cell differentiation in the normal gastric mucosa.54,55 Interestingly, Gut et al. 55 observed that 3 of 15 Car9−/− mice developed sporadic duodenal adenomas and thus concluded that the loss of CAIX might contribute to adenoma formation. Nevertheless, Car9−/− mouse studies involving the duodenal mucosa per se have not been conducted.
The presence of CAII and CAIX in duodenal adenomas has not been examined before. In our study, the characteristic expressions of CAII and CAIX in the normal villous and crypt epithelium were converted to distinctly less intense but diffuse staining in dysplastic regions. The location-dependent staining of the isozymes was thus lost in dysplasia. The same phenomenon of lesser and more diffuse CAII and CAIX expression in dysplasia has been described in conventional adenomas of the colon and dysplasia of Barrett’s esophagus.56–58 In gastric intestinal metaplasia, the immunostaining pattern of CAIX is similar to that in the duodenal epithelium, but in gastric adenomas, CAIX expression is again low, and the polarized staining pattern is lost. 59 It appears that CAII and CAIX stains might be useful for histopathological diagnostics of dysplasia, at least for duodenal specimens.
CAII was present in 54% of DAC samples. CAII expression was low in comparison with normal villous epithelium. Weak expression of CAII was associated with poor differentiation of carcinoma. Although there are no previous studies about CAII in DAC, CAII expression is typically downregulated in other gastrointestinal adenocarcinomas. Low CAII expression is associated with poor survival in gastric cancer 21 and metastatic disease in esophageal adenocarcinoma. 57 CAII is mainly reported as downregulated in colorectal cancer, but one contradictory report has suggested that high CAII expression in colorectal cancer was associated with shorter survival.42,56,60 Our findings however appear to be in line with most previous studies on CAII in gastrointestinal adenocarcinomas. Mechanisms linking low expression of CAII to poor differentiation or prognosis are, largely unknown. Hulikova et al. 61 have suggested that CAII downregulation might stabilize intracellular pH of cancer cells in the presence of extensive extracellular pCO2 fluctuations, thus providing malignant cells survival benefit. Consistent with the proposed role as a tumor suppressor, overexpression of CAII has been shown to inhibit the growth of colorectal carcinoma cells. 62 Studies concerning regulation of CA2 and mechanisms of the prognostic effect are warranted.
Positive staining for CAIX was detected in 70% of DAC samples. We found that low CAIX expression showed a trend for association with regional lymph node metastases, but with no statistical significance (p = 0.091). No association with prognosis or other clinicopathological parameters were observed. A coinciding, significant association with high CAIX expression and lack of nodal spread was reached in the only previous study available, in which the authors, with a considerably larger cohort, also found worse overall survival in patients with low CAIX expression (26 vs 67 months). 37 The lack of prognostic significance in our study is most likely related to the small size of our case series and an obvious lack of statistical power. Due to the rarity of the disease, a larger national or international study on the prognostic value of CAIX in DAC is needed. 63 CAIX staining was absent in 30% of duodenal carcinomas. Although the possibility of negative staining due to technical reasons cannot be entirely excluded, most specimens had internal positive controls such as normal duodenal crypts, indicating the true absence of staining. Furthermore, the rate of absent CAIX staining was comparable to other gastrointestinal adenocarcinomas.27,64,65 Total negativity of staining was not related to stage or prognosis (data not shown).
CAIX expression in gastric and colorectal carcinomas shows differences in comparison with CAIX expression in DAC. In gastric cancer, positive CAIX labeling has been reported in 50–60% of cases. The role of CAIX expression in gastric cancer is elusive—both studies indicating no association with clinicopathological variables or survival65,66 and studies showing significant association between high CAIX expression and poor survival have been reported.67,68 In comparison with colorectal cancer, the expression profile and possible role of CAIX in DAC are also divergent. Our study found that CAIX overexpression shows a trend for association with the absence of regional lymph node metastasis. In line with our finding, Gu and Kwon 37 showed with a larger data that also better differentiation, lower stage, lack of metastasis, and better survival associate with high CAIX expression. Regarding colorectal cancer, several groups have found variable levels of CAIX expression, but no significant association with clinicopathological variables or survival.42,60,64,69 However, many investigators still maintain that pharmacological inhibition of CAIX or knockout of CA9 reduce colorectal cancer cell growth, at least in hypoxic conditions.70–72 The oncological treatment protocols for colorectal cancer are currently adopted for the treatment of DAC. According to several genome-based biomarker studies,73–75 and supported by our results with CAIX here, it seems that DAC is an independent cancer entity with distinct differences in the genetic profile and in the role of CAIX in comparison with colorectal cancer. Future studies should be aimed to further assess these differences for more tailored treatment of DAC.
A relevant question is to what extent CAIX expression in gastrointestinal adenocarcinomas is regulated by hypoxia. Nakamura et al. 66 analyzed the expression patterns of CAIX in intestinal-type gastric cancer and concluded that instead of hypoxia and HIF-1α, CAIX overexpression was induced by hypomethylation of the CpG site at position-74 of the CA9 promoter. They also showed that strong CAIX expression and hypomethylation status of gastric glandular epithelium were preserved in intestinal-type adenocarcinoma. Our observation of strong CAIX expression in duodenal carcinoma, comparable to expression in the normal crypt epithelium, is consistent with the concept of hypoxia-independent regulation of CA9 in those cancers, where high endogenous CAIX expression is present, such as DAC or gastric intestinal–type adenocarcinoma. This concept is further supported by our supplementary immunohistochemistry performed on DAC samples with HIF-1α and hypoxic markers MCT4 and GLUT1. These markers were all expressed in carcinoma, but the expression levels showed no correlation with the expression of CAIX. This finding indicates that the microenvironment of DAC is probably hypoxic, like in the majority of solid tumors, and also supports the hypothesis that expression of CAIX is not solely hypoxia-dependent in normal duodenal epithelium or in DAC.
In addition to epigenetic alterations, other hypoxia-independent regulators of CAIX have been reported. These regulators, such as acidosis, cell density, and MAPK (mitogen-activated protein kinase)-pathway, however, might also function via HIF-1a. 76 On the contrary, CA9 is not induced in the presence of HIF-2α activation or promoter hypermethylation. 76 These factors possibly lead to low expression of CAIX seen in 30% of duodenal carcinomas in our study. Finally, activation of tumor suppressor gene TP53 might be involved. Although aberrant p53 is common in small intestinal adenocarcinomas, still more than 40% of DACs carry functional wild-type p53, 73 which is known for its capacity to downregulate CAIX. 77 Regulation of CA9 in cancer types, such as DAC or intestinal-type gastric cancer, still needs further evaluation.
One of the current concepts of function regarding CAIX in cancer is based on the relatively well-evidenced cooperation between CAIX and ion transporters. CAIX forms efficient transport metabolons with sodium-hydrogen antiporter (NHE-1), 78 bicarbonate transporters (AE1-3, NBCs),79,80 and lactate carriers (MCT1/4).81,82 These transporters have also been reported to be present in duodenal epithelial cells.83–86 However, based on recent evidence, transport metabolons promote cancer progression.87–90 Thus, as overexpression of CAIX in DAC might be beneficial, it is unlikely linked with the cancer-promoting metabolons in this cancer type.
The strength of our study is the homogeneous study population from a single tertiary care hospital catchment area, thus minimizing selection bias. In addition, interobserver agreement in the assessment of immunostaining was excellent. Due to the rarity of the malignancy, the limited number of cases remained the major weakness of the study, even though patients from a 20-year timespan were included. The use of immunohistochemistry as the only evaluation method of expression was justifiable, as the antibodies applied are well characterized,28,43,44 and the staining conditions were adequately controlled.
We conclude that CAII is downregulated in duodenal adenomas and adenocarcinoma. Low expression of CAII was associated with poorer tumor differentiation. CAIX expression levels in adenomas and adenocarcinoma were comparable to the high expression in proliferating cells of normal duodenal crypts. Low CAIX expression showed a potential trend for association with the presence of regional lymph node metastases. The possible positive prognostic value of high CAIX expression for this rare disease should be confirmed with a larger study using a validation cohort. We also suggest that both CAII and CAIX could represent markers of epithelial dysplasia, at least in the duodenum.
Supplemental Material
sj-pdf-1-jhc-10.1177_00221554211050133 – Supplemental material for Carbonic Anhydrases II and IX in Non-ampullary Duodenal Adenomas and Adenocarcinoma
Supplemental material, sj-pdf-1-jhc-10.1177_00221554211050133 for Carbonic Anhydrases II and IX in Non-ampullary Duodenal Adenomas and Adenocarcinoma by Minna Nortunen, Seppo Parkkila, Juha Saarnio, Heikki Huhta and Tuomo J. Karttunen in Journal of Histochemistry & Cytochemistry
Footnotes
Acknowledgements
The authors thank Ms. Marianne Kuuslahti for skillful technical assistance.
Competing Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
TJK and MN were involved in conceptualization; TJK and SP were involved in methodology; MN, TJK, and HH were involved in investigation; MN, TJK, and HH were involved in formal analysis; MN and HH were involved in data curation; TJK and SP were involved in selection of resources; MN was involved in writing—original draft preparation; MN, TJK, HH; SP, and JS were involved in writing—review and editing; TJK and HH were involved in validation; MN, TJK, and HH were involved in visualization; TJK and JS were involved in supervision; TJK and HH were involved in project administration; TJK, JS, and HH were involved in funding acquisition. All authors have approved the final version to be published and have agreed to be accountable for every aspect of the work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Vieno and Alli Suorsa Health Care Foundation (H.H.) and the Finnish Cultural Foundation (H.H.).
Data Accessibility Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request. The data are not publicly available due to ethical restrictions.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.